Article Text

Abstract
Background and purpose Diabetes mellitus (DM) is a common metabolic disorder with increased risk of cardiovascular and cerebrovascular complications. However, its relationship with risk of subarachnoid haemorrhage (SAH), the most devastating form of stroke, remains controversial.
Methods To evaluate the relationship between DM and risk of SAH, we performed a retrospective cohort study using a nationwide, population‐based, health screening database in Korea. We included participants without history of stroke who underwent a nationwide health screening programme between 2003 and 2004. Primary outcome was occurrence of SAH. Participants were followed up until development of SAH or December 2015. Multivariate Cox proportional hazards regression analysis was performed with adjustments for age, sex, systolic blood pressure, total cholesterol, body mass index, physical activity, smoking status, alcohol habit, household income and treatment with antihypertensive agents and statins.
Results Among 421 768 study participants, prevalence of DM was 9.6%. During a mean follow-up period of 11.6±1.9 years, 1039 patients developed SAH. Presence of DM was significantly associated with decreased risk of SAH (adjusted HR 0.68; 95% CI 0.53 to 0.86; p<0.001). Elevated level of fasting blood glucose was also negatively associated with risk of SAH (adjusted HR per 1 mmol/L increase 0.90; 95% CI 0.86 to 0.95; p<0.001).
Conclusion DM and elevated level of fasting blood glucose were inversely associated with risk of SAH. Further studies may elucidate the possibly protective, pathophysiological role played by hyperglycaemia in patients at risk of SAH.
- subarachnoid
- stroke
- aneurysm
Data availability statement
Data may be obtained from a third party and are not publicly available. The NHIS-HEALS data set supporting the conclusion of this article is available on request from the National Health Insurance Sharing Service (http://nhiss.nhis.or.kr/bd/ab/bdaba021eng.do). To gain access to the data, a completed application form, research proposal and an applicant’s approval documents from the institutional review board should be submitted to and reviewed by the inquiry committee of research support in the National Health Insurance Sharing Service. Currently, use of NHIS-HEALS data set is allowed only for Korean researchers.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Subarachnoid haemorrhage (SAH) is the most devastating form of stroke, which results in death or severe disability in 50%–70% of affected patients.1 2 A relatively younger age of onset and a high associated probability of long-term disability after occurrence of SAH impose a heavy burden on patients, their families and communities.3 4 Despite the significant global health problem with SAH, risk factors for SAH have not been adequately investigated in large cohorts.5 Diabetes mellitus (DM) is a common metabolic disorder and is a well-established cardiovascular risk factor for atherosclerotic disease involving coronary, peripheral and cerebral arteries. However, there are epidemiological data indicating a paradoxically reduced risk of aneurysmal disorders in patients with diabetes.6 7 The prevalence and incidence of aortic aneurysms are lower in patients with diabetes as compared with that in those without the disorder.8–10 Approximately >80% of cases of spontaneous SAH occur as a consequence of ruptured cerebral aneurysms.11 With regard to the potential role of DM against aneurysmal disorders, we hypothesised that the risk for SAH may be lower in diabetes compared with non-diabetes. Although DM is a common medical illness and SAH is a major life-threatening disorder, the relationship between SAH and DM has received little attention and still remains unclear. Investigation of the possible relationship may contribute to better understanding of the pathophysiology of SAH and allow researchers to identify potential therapeutic targets for intervention. In the current study, we aimed to evaluate the risk of SAH according to the presence of DM and fasting blood glucose levels using a nationwide, population-based, health screening cohort database in Korea.
Methods
Study design and data sources
This study was a retrospective cohort study conducted using the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea.12 NHIS-HEALS is a nationwide, population-based sample cohort, which includes 514 866 subjects (aged between 40 and 79 years) who participated in a free national health screening programme organised by the NHIS. Data collected as part of the health screening programme included physical examination findings, self-administered questionnaires for eliciting medical history and lifestyle details and results of blood laboratory investigations including fasting glucose. The national health screening programme in Korea can only be conducted at designated healthcare centres or hospitals. For maintenance and quality control of health screening programme, the NHIS of the Korea government has conducted the quality assessment activities on the human resource, facility, equipment and the reliability of laboratory tests of individual health screening centres. According to the quality reports of health screening, institutions receiving low grade are subject to administrative dispositions such as temporary suspension and cancellation of the designation. The results of the quality assessment of the institutions are available on the web page of the NHIS (https://hi.nhic.or.kr/ca/ggpca001/ggpca001_m02.do).
NHIS is a single-payer programme in Korea, and the NHIS-HEALS database contains complete health insurance claims data for all hospital visits, which include diagnostic code, procedure performed, prescriptions issued, demographic information (sex, age, annual household income) and mortality data between 2002 and 2015. Diagnostic codes are recorded at each hospital visit, according to the International Statistical Classification of Diseases, 10th Revision (ICD-10). Data from NHIS-HEALS were fully anonymised as per data privacy restrictions and did not contain any identifying information.
Participants and outcomes
We included stroke-free participants who underwent the health screening in 2003–2004. Index date was defined as the day on which each participant underwent a health screening programme. We excluded participants who had: (1) history of stroke, (2) <1 month of follow-up data available, (3) extreme values of fasting blood glucose (≤3 or ≥25 mmol/L), and (4) missing values for covariates. Primary outcome was the development of spontaneous (non-traumatic) SAH during the study period. Development of spontaneous SAH was defined as those participants who were admitted with a primary diagnosis of I60 (ICD-10 code for non-traumatic SAH), excluding I60.8 (meningeal haemorrhage and rupture of cerebral arteriovenous malformation), and underwent brain CT or MR angiography during admission.13 14 Patients with ICD-10 codes of S02, S04, S06, S07, S09, T02.0, T04.0 and T06.0 in their records were not captured in a bid to exclude those who had experienced outcomes of traumatic SAH. Study participants were followed up until the development of SAH, study end date (31 December 2015), loss of eligibility to the NHIS or date of death, whichever outcome occurred first.
Data collection
A patient was identified as suffering from DM if either the fasting glucose level during the health examination was ≥7 mmol/L or if the participant answered ‘yes’ in response to the question eliciting this medical history on the health examination questionnaire.15 The health examination data were used to collate information on relevant factors including age, sex, household income, body mass index (BMI), systolic blood pressure, fasting blood glucose, total cholesterol level, smoking habit, alcohol consumption and physical activity. Household income were stratified into three tertiles (low, middle, high). Based on BMI, patients were classified into one of the following four groups: low (<18.5 kg/m2), normal (18.5–25 kg/m2), obesity 1 (25–30 kg/m2) and obesity 2 (≥30 kg/m2).15 Smoking status was used to classify patients as ‘current smoker’, ‘ex-smoker’ or ‘never smoker’. Based on patients’ average weekly alcohol consumption, they were classified into groups of ‘<1 time’, ‘1–2 times’, ‘3–4 times’ and ‘≥5 times’.16 Depending on the number of days that patients reportedly exercised per week on average (regardless of the type or intensity of the workout), they were classified into one of the following groups: ‘<1 day’, ‘1–3 days’ and ‘≥4 days’. Treatments with antihypertensive medication (calcium channel blockers, ACE inhibitors, angiotensin receptor blockers, diuretics and beta blockers) and statin (atorvastatin, fluvastatin, lovastatin, pitavastatin, pravastatin, rosuvastatin and simvastatin) were determined by prescription of the medications between 1 year before and the date of the baseline health examination.
Statistical analyses
Clinical characteristics were represented as number (%) for categorical variables and as mean±SD for continuous variables. Differences in characteristics between groups were compared using the χ2 test and the independent t-test for categorical and continuous variables, respectively. Continuous variables included age, BMI, systolic blood pressure, total cholesterol and fasting serum glucose. We calculated the standardised mean difference for each variable between those with diabetes and non-diabetes.17 We constructed a cumulative incidence plot for SAH according to the presence of DM. HR and 95% CI for primary outcome were calculated based on a Cox proportional hazards regression analysis. We constructed (1) a model adjusted for age and sex, and (2) a model fully adjusted for age, sex, systolic blood pressure, BMI, total cholesterol, household income, lifestyle habits (exercise, smoking, alcohol), treatments with antihypertensive agents and statins, and interaction terms between systolic blood pressure and antihypertensive agents, and between total cholesterol and statins. The assumption of proportional hazards for DM and fasting glucose in Cox regression model was tested by calculating the Schoenfeld residuals using ‘cox.zph’ function in the R package, which were found to be satisfactory. The linear association between log hazard and level of fasting glucose is illustrated by constructing the flexible HR curve using the penalised spline smoothing functions of the ‘smoothHR’ package in R.18 Data manipulation and statistical analyses were performed using both SAS V.9.4 (SAS) and R software V.3.3.3 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/). A two-sided p value <0.05 was regarded as statistically significant.
Results
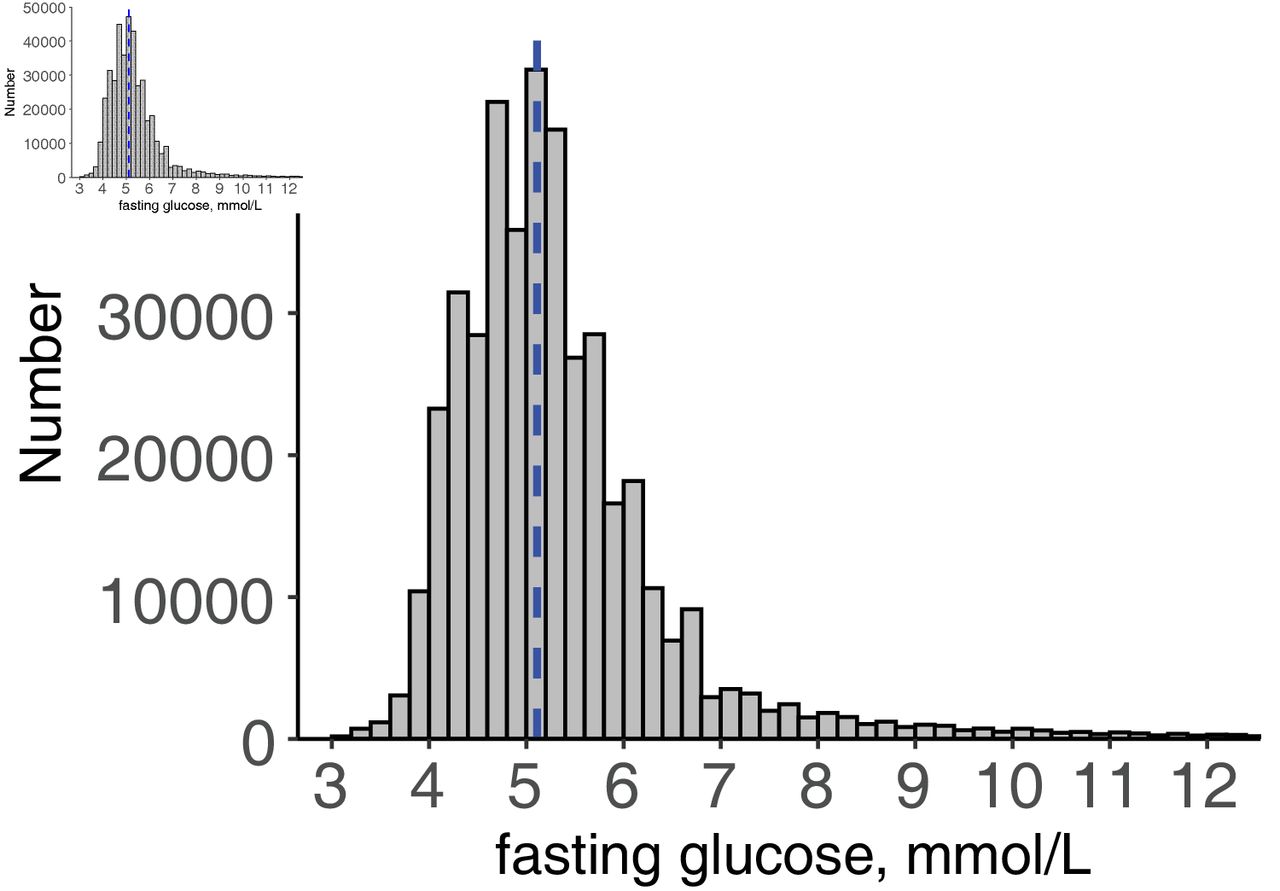
Following application of both inclusion and exclusion criteria, this study finally included 421 768 participants without history of stroke, who underwent health screening examination in 2003–2004 (figure 1). Mean age of the study population at the time of screening was 53.7±9.5 years, and males constituted 55.2% of the cohort (table 1). Mean level of fasting glucose was 5.43±1.58 mmol/L and figure 2 shows the distribution of fasting glucose level in the study population. In total, 9.6% of participants were identified as having DM. Compared with non-diabetes, those with diabetes were more likely to be male, older, receive treatments with antihypertensive agents and statins, and to have high systolic blood pressure, high total cholesterol and high fasting blood glucose levels. Both groups differed significantly with respect to factors including BMI, smoking habit, alcohol consumption, exercise and household income.
Baseline characteristics of the study population

Flow chart of patient inclusion and exclusion. NHIS-HEALS, National Health Insurance Service-National Health Screening Cohort.

Distribution of fasting glucose level in study population. Histogram represents the number of participants at each level of fasting glucose (intervals of 0.2 mmol/L). Blue dashed line indicates median value of fasting glucose (5.11 mmol/L).
The mean follow-up period was 11.6±1.9 years. During the study period, 1039 subjects developed primary outcome (spontaneous SAH). Figure 3 illustrates the cumulative incidence curve of SAH, according to the presence of DM, which indicates that the risk of occurrence of SAH is lower in those with DM. On computing a hazards model adjusted for age and sex (table 2), patients with DM had significantly lower risk of SAH, as compared with non-diabetics (HR 0.73; 95% CI 0.58 to 0.93; p=0.010). Significance of DM as an independent factor did not change in fully adjusted models as well (HR 0.68; 95% CI 0.53 to 0.86; p<0.001). In the fully adjusted model, risk factors associated with SAH were female sex, old age, high systolic blood pressure and current smoking. Obesity was associated with lower risk for SAH. Instead of the presence of DM, incorporating level of fasting blood glucose as a possible risk factor in the model also revealed an inverse association between blood glucose level and risk of occurrence of SAH. Calculated HR per 1 mmol/L increase in fasting glucose in the age and sex-adjusted model and in that fully adjusted model for other covariates was 0.92 (95% CI 0.88 to 0.97) (p<0.001) and 0.90 (95% CI 0.86 to 0.95) (p<0.001), respectively. For further evaluation of the association between SAH risk and the continuous level of fasting glucose, we illustrate spline-based log HR curve (figure 4). A visual inspection of the HR curve indicates that the level of fasting glucose is in inverse linear relation to the log hazard. Our data clearly showed that the presence of DM and elevated levels of fasting glucose were negatively associated with risk of SAH, a critical cerebrovascular disorder.
Risk of subarachnoid haemorrhage according to the presence of diabetes mellitus

Cumulative incidence curve for subarachnoid haemorrhage according to diabetes mellitus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inverse linear association between fasting glucose level and the risk of subarachnoid haemorrhage. The curved black line and grey shadows represent the estimated log HR and 95% CIs taking the median value of fasting glucose (5.11 mmol/L) as reference (HR=1.0) using penalised spline smoothing function from the Cox regression model for subarachnoid haemorrhage. The HR curve shows that the level of fasting glucose is in inverse linear relation to the log hazard.
Discussion
This population-based cohort study showed that patients with DM were at a lower risk for spontaneous SAH, as compared with non-diabetics. Fasting blood glucose level was negatively associated with the risk of SAH. Other factors including female sex, old age, high blood pressure and current smoking habit were found to be independent risk factors for SAH. These are already well-established risk factors for SAH.7 19 20 This consistent finding of a positive association with known risk factors in the current study supports the reliability of our cohort data. The inverse association between DM and SAH was in line with the prior epidemiological reports for the negative relationship between diabetes and aortic aneurysms (another dilating aneurysmal vascular disorder).10 21 DM is known to be negatively associated with both the presence, size and growth rate of aortic aneurysms.9 22 A systematic review of existing literature on the topic, which included 17 large population prevalence studies, found a significantly lower risk of occurrence of abdominal aortic aneurysms in patients with diabetes (pooled OR 0.80; 95% CI 0.70 to 0.90; p<0.001).23 A longitudinal study of patients with abdominal aortic aneurysms showed an inverse association between aneurysmal growth rate and HbA1c levels both in diabetic individuals and in those without diabetes, indicating that chronically elevated blood sugar inhibits aneurysmal progression.24 Considering that a large aortic diameter and high growth rate are major risk factors for aneurysmal rupture, patients with diabetes may be at a lower risk of developing aortic aneurysm rupture.8 9
While prior studies consistently found a negative association of diabetes with aortic aneurysms, there were inconsistent reports on its relationship with SAH, which commonly occurs due to rupture of an intracerebral aneurysm.25 26 In the first report on this topic published in 1978, based on the Harvard Cooperative Stroke Registry data, only 2% of patients with aneurysmal SAH had DM, as compared with its presence in 13%–29% of patients diagnosed with other types of cerebrovascular diseases.27 In another age and sex-matched case–control study of 329 patients diagnosed with aneurysmal SAH, prevalence of DM was lower than that in the general population, although the differences did not reach statistical significance.28 Data reported in two systemic reviews demonstrated that presence of DM was significantly associated with lower risk of SAH in case–control studies, but not in longitudinal studies.7 25 In one meta-analysis, data from high-quality studies (n=5) found significant association between aneurysmal SAH and DM, but those derived from low to moderate-quality studies (n=13) did not.25 In a case–control study between two groups of 1058 and 484 patients with ruptured and unruptured intracranial saccular aneurysms, incidence of DM did not significantly differ.26 However, a recent large cohort study conducted using linked electronic health records in England, with a median follow-up duration of 5.5 years, demonstrated that type 2 diabetes was inversely associated with SAH (adjusted HR 0.48; 95% CI 0.26 to 0.89).29 The Million Women Study, a cohort study of British women, found women with DM had substantially reduced risk for SAH (relative risk 0.43; 95% CI 0.26 to 0.69) compared with other women.30 Factors including small sample size, high heterogeneity of the study population and lack of consideration of confounding variables can lead to conflicting results and limit the identification of the potential effect of DM on risk of SAH. We added an evidence for the significant relationship between DM and risk of SAH based on longitudinal cohort data in Korea. The inverse dose–response relationship between the level of fasting glucose and the risk of SAH also suggests the contributing role of glycaemic control on the development of SAH.
Our current study was based on data collected during a nationwide health screening programme, which enabled inclusion of a large study sample (>400 000) from the general population and allowed collation of information about known potential confounders such as systolic blood pressure, BMI, cholesterol level, physical activity level, smoking habit and alcohol consumption, an aspect frequently lacked in prior studies.31 Further, utilisation of national health claims data enabled long-term follow-up and allowed identification of patients diagnosed with a critical and highly fatal, though relatively rare, condition like SAH, which would have been difficult to achieve with conventional data collection methods. The present study strengthened by these factors showed an inverse association between risk of SAH and presence of DM or an elevated fasting glucose level, an association that remained significant even after allowing adjustments for the potential confounders. Our data support the existence of a possibly protective pathophysiological role of DM and hyperglycaemia in patients at risk of SAH.
There are some explanatory mechanisms for the protective role played by DM in dilating aneurysmal disorders.9 32 Diabetes induces atherosclerotic changes that cause stiffening of vessel walls, which are therefore more resistant to haemodynamic pressure and are less likely to undergo dilation and consequent rupture.31 Collagen cross-linking induced by advanced glycation end products generated in diabetes may protect against its proteolytic breakdown and thus play a protective role, preventing aneurysmal progression.33 Diabetic animal models showed decrease in both macrophage infiltration and neovascularisation within arterial walls, both proinflammatory processes involved in development and progression of aneurysms.9 Indeed, intraoperative findings have shown that DM was more frequent in stabilised intracranial aneurysms.34 Further, levels of plasmin and matrix metalloproteinase-2 and metalloproteinase-9 are suppressed in patients with diabetes, which may restrict fibrinolytic pathway, progressive degeneration and remodelling of aneurysmal vessel walls.10 22 35 Lifestyle, social habits and other known coexisting risk factors could be potential confounders in the relationship between DM and SAH. It is strongly recommended that patients with diabetes maintain healthy lifestyles and control modifiable cardiovascular risk factors such as blood pressure, obesity, physical activity and smoking habit, which may contribute to the paradoxically lower risk of SAH in observational studies.28 Frequent hospital visits by patients with diabetes may lead to an earlier diagnosis and treatment of cerebral aneurysms, thus mitigating an important risk factor for occurrence of SAH.26 Another explanation involves the protective role played by cardiovascular medications frequently prescribed to patients with diabetes. A large proportion of patients with diabetes suffer from hypertension and receive antihypertensive drugs, which reduce high blood pressure, a strong modifiable risk factor for SAH. Statins are also frequently prescribed to patients with diabetes, considering their increased cardiovascular risk. In vitro and in vivo studies suggest that statins can protect against rupture of cerebral aneurysm.13 Pleiotropic effects of antidiabetic medications may prevent further dilatation and rupture of an aneurysmal vessel wall. A nested case–control study found that metformin, sulfonylurea and thiazolidinedione-treated patients were at lower risk of aortic aneurysms.36 Unfortunately, these explanatory mechanisms for lower risk of SAH in patients with diabetes were principally evaluated with respect to aortic aneurysms, and relationship with SAH/cerebral aneurysm was not well elucidated. Further research is needed to evaluate the effects of DM on the process of formation and rupture of cerebral aneurysms.25 The exploration of a possibly protective role played by DM may help us identify potential therapeutic targets for management of those with unruptured cerebral aneurysms (which are relatively common in the general population, incidence 3%–5%), and who are at a high risk of developing SAH, a critical illness with high mortality.37
Besides these strengths, we also acknowledge certain limitations of the current study. First, this was an observational, retrospective cohort study. The observational study design cannot establish a causal relationship. Second, as it was difficult to distinguish patients with type 1 and type 2 diabetes based on health claims data, we could not further evaluate the difference in risk of SAH in those with either type of DM. Inclusion of participants aged 40–79 years may have automatically restricted the study of correlation with type 1 diabetes, which typically occurs in children. A prior cohort study in Finland reported that patients with type 1 diabetes are at an increased risk for non-aneurysmal SAH.38 Third, identification of patients who experienced spontaneous SAH, based on ICD-10 coding data in their records, may have limited accuracy. Because we determined the study outcome as admission with primary diagnosis of I60 and brain imaging, sudden death due to SAH without hospital visit could not be captured due to lack of the health claims codes for admission and examination. While we attempted to exclude cases with traumatic SAH to the best of our ability, it is possible that a certain number may have been included due to erroneous coding and may act as potential confounders. Fourthly, SAH also could arise due to arteriovenous malformations or other vascular aetiologies other than following rupture of cerebral aneurysms. The current study could not clearly distinguish between cases of aneurysmal and those of non-aneurysmal SAH. Fifth, NHIS-HEALS lacked data for haemoglobin A1c, the long-term indicator of glucose control. There is a need for further research whether there is difference in SAH risk according to the haemoglobin A1c in diabetes. Finally, our data are obtained only from the Korean population. Different ethnic and genetic backgrounds may influence baseline susceptibility to SAH.
Conclusion
This study, based on large population-based cohort data, demonstrated that patients with diabetes were at lower risk for spontaneous SAH. Exploration and identification of the underlying protective mechanisms may help us understand the pathophysiology of SAH and allow us to determine novel therapeutic targets, which can be used to prevent the fatal disorder.
Data availability statement
Data may be obtained from a third party and are not publicly available. The NHIS-HEALS data set supporting the conclusion of this article is available on request from the National Health Insurance Sharing Service (http://nhiss.nhis.or.kr/bd/ab/bdaba021eng.do). To gain access to the data, a completed application form, research proposal and an applicant’s approval documents from the institutional review board should be submitted to and reviewed by the inquiry committee of research support in the National Health Insurance Sharing Service. Currently, use of NHIS-HEALS data set is allowed only for Korean researchers.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board of the Yongin Severance Hospital (9-2020-0008), and requirement of informed consent was waived, considering the retrospective nature of the study and the use of anonymised data.
Acknowledgments
This study used the dataset of NHIS-HEALS (NHIS-2018-2-236) created by the National Health Insurance Sharing Service.
References
Footnotes
Contributors Concept and design: JHK, JK. Statistical analysis and interpretation of data: JK, JJ. Drafting of the manuscript: JHK, JK. Funding: JK. Critical revision of the manuscript and important intellectual contribution: JHK, JJ, JK.
Funding This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2020R1I1A1A01060447). This study was supported by a faculty research grant of Yonsei University College of Medicine for 2020 (6-2020-0163).
Disclaimer The funding body did not participate in the design, collection, analysis, or interpretation of data, or in the decision to submit the manuscript for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.