Article Text

Abstract
Background With widely usage of flow diverter in intracranial aneurysm treatment, some previously used predictors may not be effective in evaluating the recurrence risk. We aimed to comprehensively re-evaluate the predictors of intracranial aneurysm outcome with various endovascular treatment methods and devices.
Methods This is a prospective registered study. We analysed 6-month and 18-month follow-up angiographic data from the prospective study. Data on patient demographics, aneurysm morphology and type of treatment were recorded. Patient-specific haemodynamic simulations were performed. An unfavourable angiographic outcome was defined as recurrence of aneurysm in cases with coiling or stent-assisted coiling, patency of aneurysm in cases with flow diverters or retreatment during follow-up.
Results In total, 165 patients (177 intracranial aneurysms) with at least one angiographic follow-up data were analysed. For the short-term (6-month) results, after univariate analysis, the demographic, morphological and treatment-related factors did not achieve significantly statistical differences. The reduction ratio (RR) of velocity at aneurysm neck after embolisation was significantly lower in the unfavourable angiographic group than the favourable angiographic outcome group (p=0.002). After the Cox regression analysis, the RR of velocity at aneurysm neck was the only independent factor associated with favourable angiographic outcome (OR 0.028; p=0.001) and had an acceptable area under the curve (0.714) with a clear cut-off value (46.14%). Similarly, for the analysis of midterm (18-month) results, the RR of velocity at the aneurysm neck was the only independent significant factor for the unfavourable angiographic outcome (OR 0.050; p=0.017). The area under the curve was 0.754 and the cut-off value was 48.20%.
Conclusions The haemodynamics showed an independent effect on angiographic follow-up results and may provide helpful suggestions for clinical practice in the future.
- aneurysm
- blood flow
- angiography
- intervention
- stroke
Data availability statement
Data are available upon reasonable request. In addition to the data published within this article, anonymised data can be obtained by request by any qualified investigator.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Endovascular treatment of intracranial aneurysms has been widely performed along with the rapid development of technology and materials.1 However, a major drawback of endovascular embolisation is its relatively high recurrence rate (6.1%–33.6%) compared with surgical clipping.2–5 The large aneurysm size has been regarded to be associated with aneurysm recanalisation.3 5 During the last decade, however, flow diverters designed to modify the blood haemodynamics have been proven more effective (90% complete occlusion rate) in the endovascular treatment of large and giant intracranial aneurysms.6–8 Therefore, we consider that morphological factors, such as aneurysm size, may no longer be predictive in aneurysm recurrence because more optimal treatment strategy could be chosen in this new era. Thus, a re-evaluation of predictive factors from multidimensional analyses associated with the angiographic outcome of intracranial aneurysms after a variety of interventions is needed.
As the concept of flow remodelling is accepted, flow analysis after the endovascular treatment is necessary and the computational fluid dynamics (CFD) is a valuable tool for this. Some previous haemodynamic studies have focused on the aneurysm outcomes after endovascular treatment, including flow diverter treatment.9–11 However, all such studies were retrospective analyses, and none of them involved simulations using patient-specific inflow boundary conditions. The evidence based on these results is therefore still weak. Additionally, most of haemodynamic studies had a small sample size. In a previous study, 283 aneurysms were included to explore the haemodynamic effect on the angiographic outcome.12 However, the results were still based on a retrospective design without patient-specific simulation, and no flow diverter cases were included.
Therefore, we designed a clinical prospective study to explore the predictive factors associated with angiographic outcomes of aneurysms after endovascular treatment, especially with respect to the haemodynamics. With various devices applied and optimal treatment strategy chosen, our hypothesis is that the haemodynamics may be one of the final independent mechanisms and previously used predictors of recurrence, like aneurysm size, may no longer be effective. Unlike previous studies, both patient-specific aneurysm geometry and patient-specific inflow boundary conditions were used in the computational simulations. We aimed to comprehensively re-evaluate the predictors of angiographic aneurysm outcome with various endovascular treatment methods and devices. Cases with conventional endovascular treatment (coiling or stent-assisted coiling) and flow diverter therapy were included in this study. We believe that the findings of the present study are beneficial to clinical practice, and the haemodynamic-guided endovascular intervention may be used in the future.
Materials and methods
Study population
This prospective observational registry study was performed in our centre. This study has been registered at http://www.clinicaltrials.gov, and the protocol has been published.13 The study was approved by the institutional review board of our hospital. Informed consent was obtained from each study patient or their relatives during hospitalisation and all their data were collected anonymously. Patients were recruited in strict accordance with the previously published criteria.13 Briefly, patients who had been diagnosed with a saccular aneurysm and treated endovascularly were included in this study. The exclusion criteria were previous treatment of an intracranial aneurysm by an endovascular approach, the presence of a brain arteriovenous malformation, the presence of a dissecting aneurysm, treatment by parent vessel occlusion, treatment by a covered stent, and missing or unsatisfactory three-dimensional aneurysm images for the simulation. Ultimately, from August 2016 to March 2017, 200 patients (217 aneurysms) were eligible and enrolled in this prospective study.
Demographic and clinical data
The patients’ baseline characteristics, aneurysmal morphology and treatment-related factors were recorded and analysed. The baseline characteristics were age, sex, history of cigarette smoking and alcohol drinking, and hypertension. The morphological factors were aneurysm size (maximum size), aspect ratio (dome-to-neck ratio), size ratio (dome-to-parent-vessel-diameter ratio), shape (irregular: blebs, nipples or multiple lobes), sidewall/bifurcation, location (anterior/posterior circulation) and whether the aneurysm was ruptured or unruptured.14 15 The treatment-related factors were the treatment technique, including conventional treatment (coiling and stent-assisted coiling) or flow diverter treatment; the packing density; and the follow-up time interval.
In our centre, the treatment strategy was discussed and decided by our weekly peer-reviewed endovascular conference. If the aneurysm neck was narrow (<4 mm) or the dome–neck ratio was favourable (>2), endovascular treatment was performed by coil embolisation. If the aneurysm neck was wide (≥4 mm) or the dome–neck ratio (≤2) was unfavourable, a stent-assisted coiling technique was preferred. However, if aneurysms were larger than 10 mm or aneurysm was unfavourable for conventional coiling or stent-assisted coiling, the aneurysm was preferably treated by a flow diverter. In our centre, the anticoagulant and antiplatelet strategy in endovascular procedure has been reported previously.16 Briefly, after the femoral sheath placement, a bolus of standard heparin (70–100 IU/kg) was administered, and 1000 IU/hour will be followed to maintain an activated clotting time of ≥250 s. The dual-antiplatelet therapy (aspirin 100 mg/day, clopidogrel 75 mg/day) was given for 3–5 days before procedure if the patients with unruptured aneurysms. If the patients with ruptured aneurysms, the oral doses of clopidogrel and aspirin (300 mg each) were given 2 hours before stent placement. Clopidogrel (75 mg/day) was administered for 4–6 weeks and aspirin (100 mg/day) for at least 6 months after the procedure. The patient who received flow diverter treatment will be given dual-antiplatelet therapy for at least 6 months. In the published protocol, the follow-up period was designed as 6 months. However, with the extension of time, the recurrence rate of aneurysm treated by conventional endovascular treatment increased and the complete occlusion rate of aneurysm after flow diverter deployment also increased.17 18 Therefore, to improve the dependability of the results, the data with a longer follow-up term are also needed. For this purpose, midterm angiographic follow-up (18 months) with digital subtraction angiography (DSA), CT angiography (CTA) or magnetic resonance angiography (MRA) was also performed. For the midterm angiographic follow-up, considering the artefact, DSA was preferred in the cases with coils, and CTA or MRA may be used in flow diverter cases. An independent angiographic committee comprising three neurointerventionalists with 10 years of experience and who were blinded to the simulation results evaluated the initial treatment results and follow-up results. We evaluated the treatment results of conventional coiling and flow diverter therapy by two different methods. The results of conventional treatment were evaluated using the following classification: complete occlusion, residual neck and residual aneurysm. Aneurysm recurrence was defined as any increase in contrast filling of the aneurysms during follow-up. Recurrence was defined as an unfavourable angiographic outcome, and stable cases were considered favourable angiographic outcomes. For flow diverter treatment, a favourable angiographic outcome was defined as complete (100%) or near-complete (>90%) occlusion of the aneurysm at follow-up. Aneurysms showing patency or partial occlusion (<90%) were defined as unfavourable angiographic outcomes. Additionally, aneurysms retreated during the follow-up were considered as unfavourable outcomes for the final analysis. In such cases, the haemodynamic data of the initial treatment, not the retreatment, were used. According to the angiographic follow-up results, all cases were divided into two groups for further analysis: the favourable angiographic outcome group and the unfavourable angiographic outcome group.
Computational modelling and haemodynamic simulation
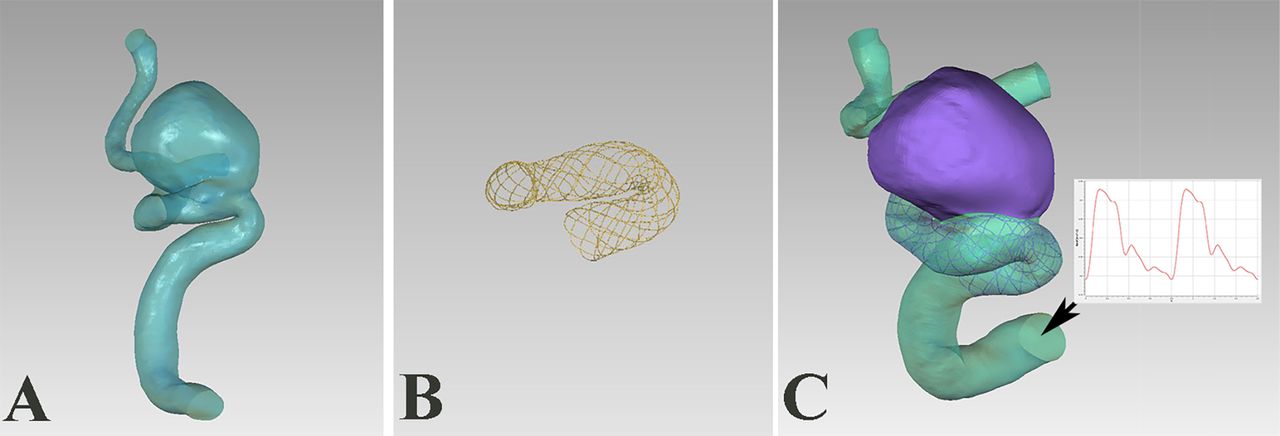
As we described previously, three-dimensional patient-specific aneurysm models were reconstructed from rotational angiography images. In cases involving stent deployment, the virtual stenting technique was used for the simulation.19 As we previously reported, we were able to virtually reconstruct all types of stent used in clinical treatment, including laser-cut stents and braided stents (including flow diverters).20 21 The data used in stent modelling were from the actual stent. The intra-aneurysmal coil mass was simulated by the porous media method (figure 1), and the parameter setting in coil modelling was calculated based on the packing density.13 Then the CFD simulations were performed. All computational models were saved as stereolithography format files and imported into ICEM CFD software (ANSYS, Canonsburg, Pennsylvania, USA) to create the volume grids used for fluid dynamics calculation. After meshing, each case was imported into ANSYS CFX V.14.0 software (ANSYS) to perform the flow simulation under pulsatile flow conditions. To obtain more accurate results in this prospective study, the inflow boundary condition was set as patient specific and a pulsatile period velocity profile was obtained by transcranial Doppler in each case before the treatment. The patient-specific pulsatile velocity boundary conditions were imposed at the model inlet using a superposition of Womersley velocity profiles. Other settings and assumptions of the simulations were made as previously described.22
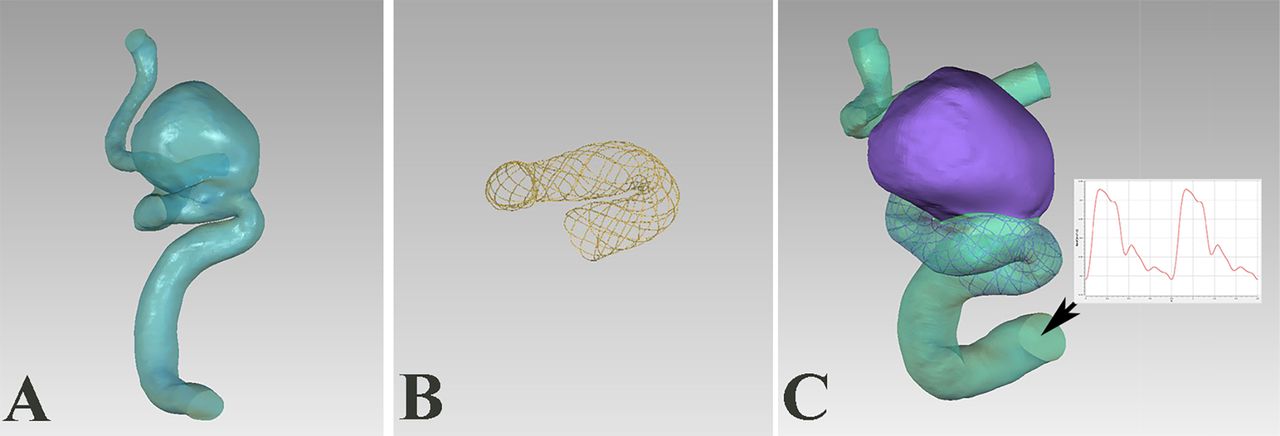
The computational fluid dynamics model. (A) Patient-specific aneurysm geometry. (B) Stent simulated by a novel virtual stenting workflow. (C) The stent was virtually deployed in the parent vessel, and the aneurysm was virtually filled with porous medium.
After the CFD simulations, the results at the aneurysm dome and neck were carefully examined. In each case, we extracted the average blood flow velocity and average wall shear stress (WSS) at peak systole both before and after treatment. The reduction ratio (RR) of each parameter, defined as (pretreatment parameter−post-treatment parameter)/pretreatment parameter, was calculated for further analysis. The changes in the flow pattern in the aneurysm sac after endovascular treatment were also analysed, including the changes of the vortices and flow impingement.
Statistical analysis
This prospective cohort was divided into two groups according to the follow-up results: the unfavourable angiographic outcome group and the favourable angiographic outcome group. Data are presented as mean and SD or median (quartile) for quantitative variables and as frequency for qualitative variables. Risk factors associated with unfavourable aneurysm angiographic outcomes were analysed. The recorded data were assessed by univariate analysis using Student’s t-test, the Wilcoxon test or the χ2 test, as appropriate. Multivariate Cox proportional hazard regression was then performed, and all variables with a p value of <0.20 in the univariate analysis were included. Statistical significance was recognised at p<0.05. Receiver operating characteristics (ROC) analysis was performed for statistically significant parameters. The area under the ROC curve (AUC) was calculated and the optimal threshold was identified. Statistical analyses were performed using IBM SPSS Statistics for Windows, V.21.0 (IBM, Armonk, New York, USA).
Results
From August 2016 to March 2017, according to the inclusion criteria, 200 patients with 217 aneurysms were enrolled in this prospective study. Ultimately, 165 patients (177 intracranial aneurysms) underwent short-term angiographic follow-up (follow-up period: 6.6±1.9 months). Unfavourable angiographic outcomes occurred in 23 (13.0%) aneurysms, and favourable angiographic outcomes occurred in 154 (87.0%). Moreover, 125 patients with 132 aneurysms received midterm angiographic follow-up (follow-up period: 18.5±5.4 months). Of the 132 intracranial aneurysms, unfavourable outcomes occurred in 15 aneurysms (11.4%). Three aneurysms underwent retreatment (one each with coiling, stent-assisted coiling and flow diverter) by the time of the short-term follow-up (6 months). Among the 132 intracranial aneurysms, 127 cases did not change between favourable or unfavourable outcome status between short-term and midterm follow-up. Two aneurysms treated with flow diverters with unfavourable short-term outcome changed to favourable midterm outcome. In contrast, three aneurysms treated with coils that had favourable short-term outcome changed to unfavourable midterm outcome.
Short-term results analysis
As shown in table 1, the patients’ demographics and morphological factor were analysed between the unfavourable angiographic outcome group and the favourable angiographic outcome group. However, no significant difference was found in any demographic and morphological factor between the two groups. The aneurysm size was larger in the unfavourable than favourable angiographic outcome group, but the difference was also not statistically significant (p=0.217).
Results from univariate statistical analysis for all variables in the short-term angiographic follow-up results
Among the 177 aneurysms, 41 were treated with coiling, 96 were treated with stent-assisted coiling and 40 were treated with flow diverter deployment. According to the follow-up results, favourable results were obtained in 32 (78.0%) aneurysms treated with coiling, 88 (91.7%) aneurysms treated with stent-assisted coiling and 34 (85.0%) aneurysms treated with flow diverters. The difference in the outcomes of the treatment methods was not statistically significant (p=0.086). Other treatment-related factors were shown in table 1.
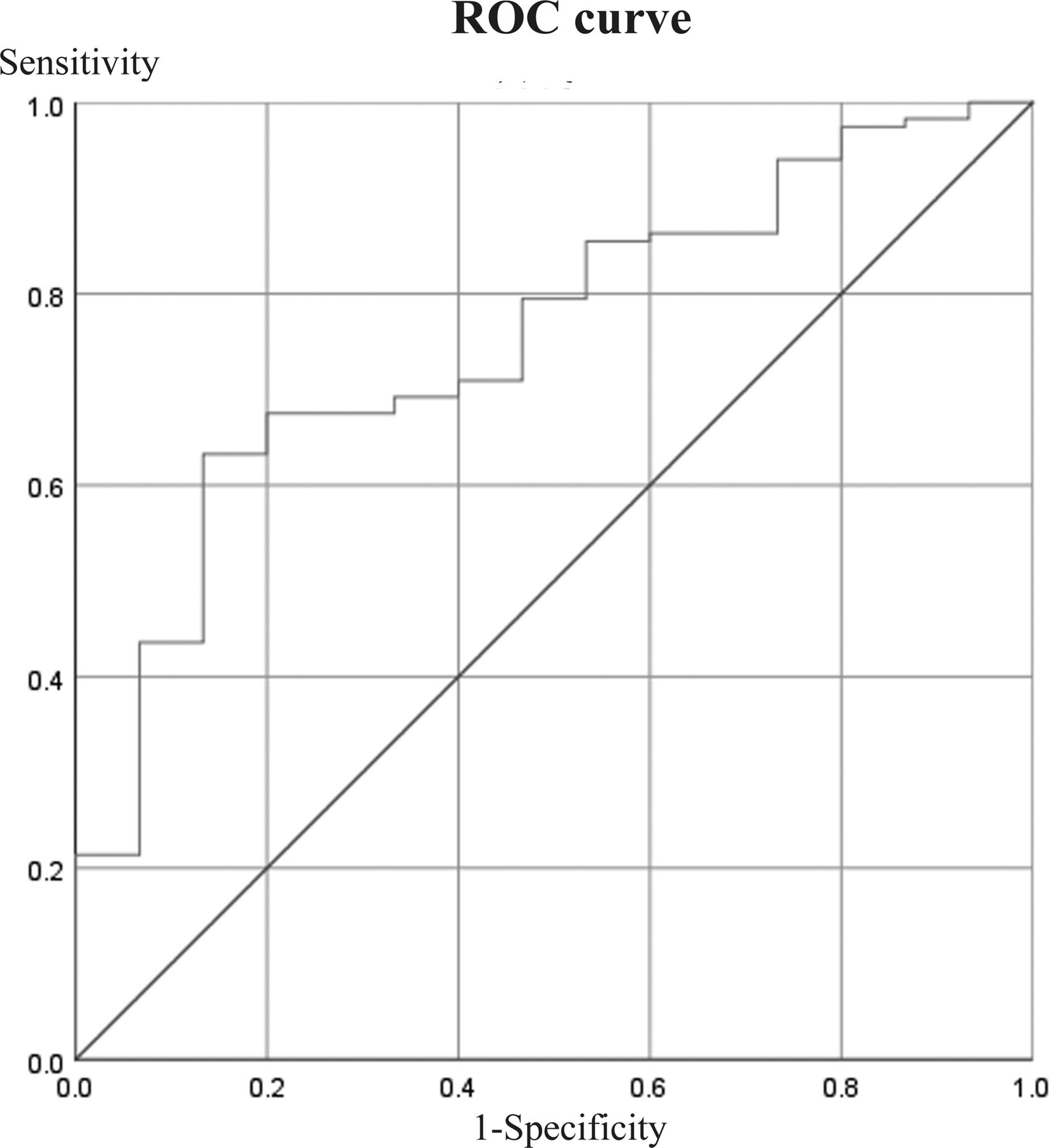
For the haemodynamic factors, the RR of velocity at the aneurysm neck was significantly lower in the unfavourable angiographic outcome group than the favourable angiographic outcome group (43.4%±22.7% vs 59.3%±22.8%, p=0.002), while the RR of WSS at the aneurysm neck was not significantly different between the two groups (median: 48.0% vs 19.5%, p=0.072) (figures 2 and 3). At the aneurysm dome, the RR of velocity (p=0.073) and WSS (p=0.488) showed no significant differences. After the Cox regression analysis, the RR of velocity at the aneurysm neck was the only independent significant factor for an unfavourable angiographic outcome (OR 0.028; 95% CI 0.004 to 0.213; p=0.001) (table 2). To identify optimal thresholds for favourable angiographic outcomes after endovascular treatment, receiver operating characteristic analysis was performed for the RR of velocity at the aneurysm neck. The RR of velocity at the aneurysm neck had an acceptable area under the curve (0.714) and clear cut-off value (46.14%) (figure 4).
Multivariate Cox proportional hazard regression analysis for the short-term angiographic follow-up results
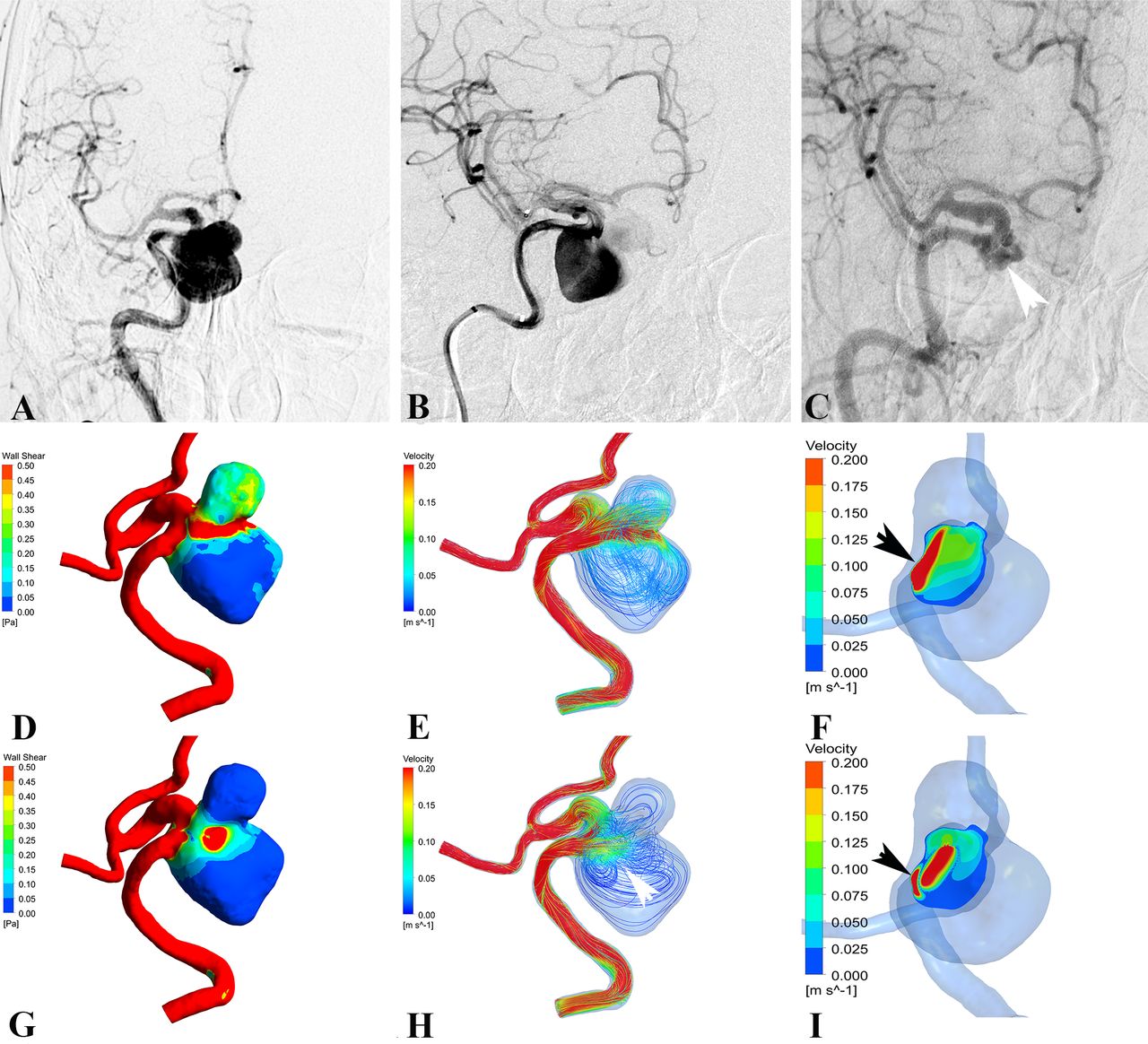
Haemodynamic changes in a case with a favourable angiographic outcome treated by stent-assisted coiling. (A) Three-dimensional digital subtraction angiography showed the aneurysm in the right internal carotid artery. (B) Immediate angiographic result after the stent-assisted coiling demonstrated complete occlusion. (C) Follow-up angiography after 6 months showed that the aneurysm had remained stable. Haemodynamics before treatment: (D) wall shear stress, (E) streamline and (F) the velocity at the neck. Haemodynamics after treatment: (G) wall shear stress, (H) streamline and (I) the velocity at the neck. After endovascular treatment, significant reductions in all shear stress and velocity were demonstrated (G–I), and no high-flow region at the neck was observed.
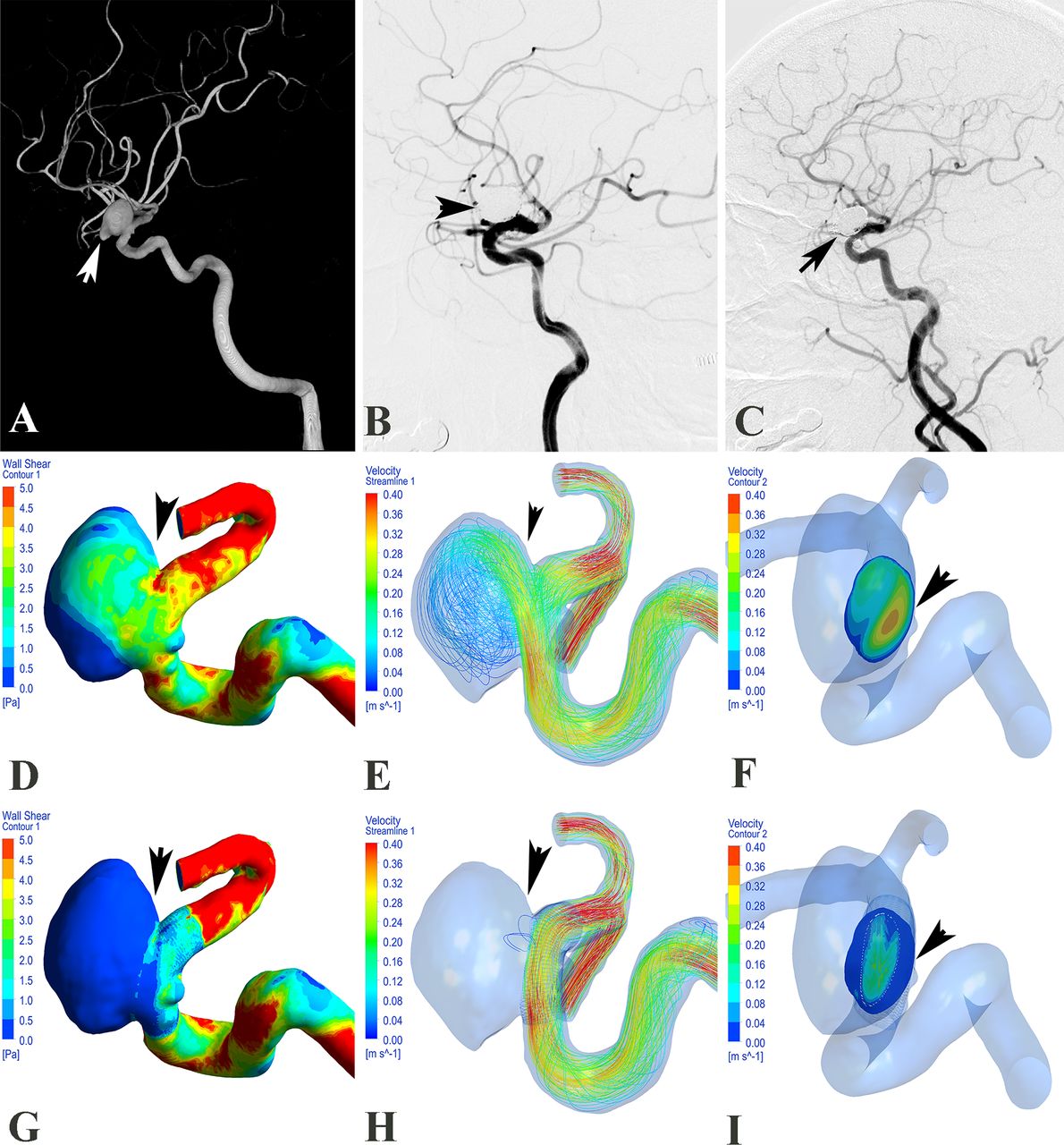
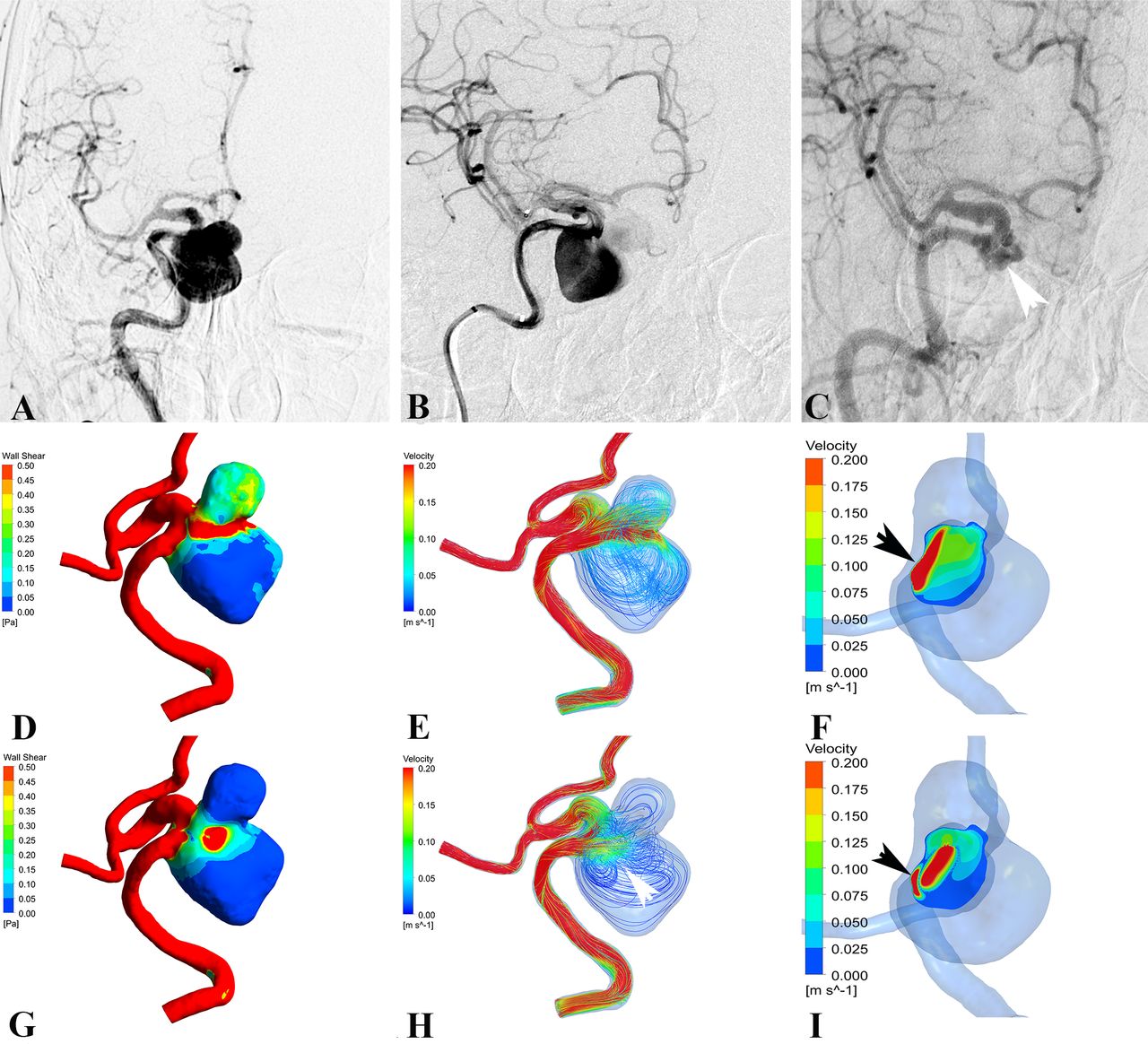
Illustrations of haemodynamics in a case with an unfavourable angiographic outcome at follow-up. (A) Digital subtraction angiography of the right internal carotid artery (frontal view) showed the aneurysm. (B) The aneurysm was treated with Pipeline Embolization Device (PED), and the frontal view of the right internal carotid artery showed significant stasis after PED deployment. (C) Follow-up angiography after 10 months showed unfavourable angiographic outcome of the aneurysm. Haemodynamics before treatment: (D) wall shear stress, (E) streamline and (F) the velocity on the neck plane. Haemodynamics after treatment: (G) wall shear stress, (H) streamline and (I) the velocity on the neck plane. After the treatment, the high-flow regions on the aneurysm neck plane were still presented (F and I, black arrows), although the overall haemodynamics was decreased. The patient’s region of aneurysm at follow-up angiography was coincident with the area which was still impacted by blood flow after the flow diverter treatment (white arrows).
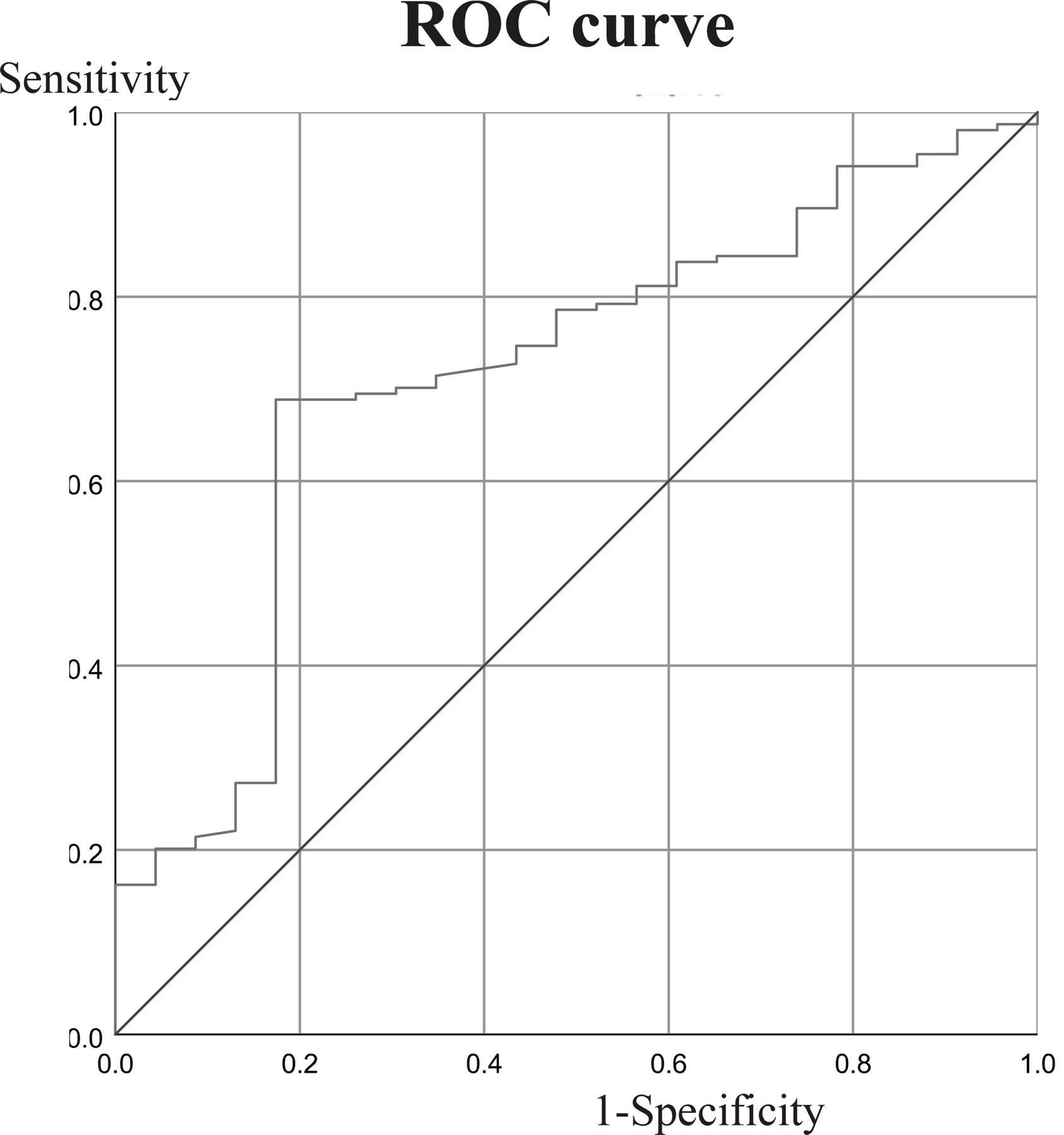
Receiver operating characteristic (ROC) curves for the reduction ratio of velocity on the aneurysm neck in the short-term angiographic follow-up results. The reduction ratio of velocity at the aneurysm neck had a clear cut-off value (46.14%) and acceptable area under the curve (0.714).
In addition to quantitative parameters, qualitative characteristics such as the flow pattern in the aneurysm dome were also analysed. Because the aneurysm sac was filled with coils after coil embolisation (coiling alone and stent-assisted coiling), the vortices were dampened (figure 2) and the complex flow pattern was simplified (figure 3), or even the flow pattern could not be observed in the aneurysm (figure 2). Among the 40 aneurysms treated with flow diverters, the vortices in 24 aneurysms showed minimal changes (intensity weakened), while the original vortices disappeared after flow diverter placement in the other 16 aneurysms. In figure 3 of an incomplete occlusion case after flow diverter treatment, a concentrated flow impingement could be observed after treatment, and such region, was coincident with the patent area at the follow-up (figure 3, white arrows).
Midterm results analysis
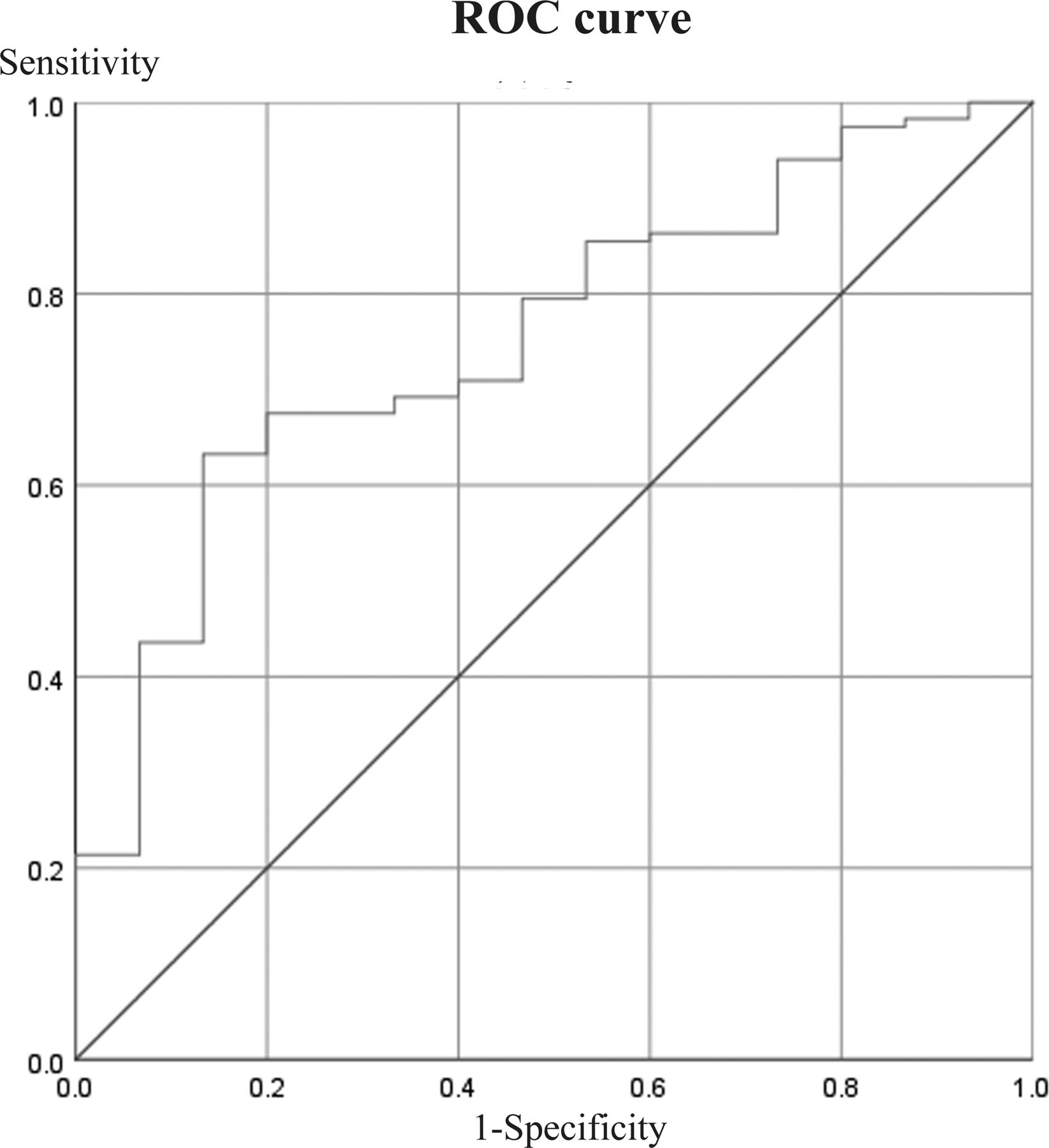
Of the 132 aneurysms, 27 were treated with coiling, 76 with stent-assisted coiling and 29 with flow diverters (table 3). Favourable angiographic results were achieved in 21 out of 27 (77.8%) cases treated with coiling, 70 out of 76 (92.1%) cases treated with stent-assisted coiling and 26 out of 29 (89.7%) cases treated with flow diverters. After univariate analysis, similarly to the short-term angiographic follow-up results, all the demographic, morphological and treatment-related factors did not achieve significantly statistical differences between the two groups (p>0.05). The RR of velocity at the aneurysm neck was the only factor significantly associated with the unfavourable angiographic outcome (p=0.001). After the Cox regression analysis, the RR of velocity at the aneurysm neck remained significance in predicting the unfavourable angiographic outcome (OR 0.050; 95% CI 0.004 to 0.585; p=0.017) (table 4). In the midterm follow-up results, the AUC for the RR of velocity at the aneurysm neck was 0.754 and the cut-off value was 48.20% (95% CI 0.636% to 0.871%) (figure 5).
Results from univariate statistical analysis for all variables in the midterm angiographic follow-up results
Multivariate Cox proportional hazard regression in the midterm angiographic follow-up results
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves for the reduction ratio of velocity at the aneurysm neck in the midterm angiographic follow-up results. The reduction ratio of velocity at the aneurysm neck had a clear cut-off value (48.20%) and acceptable area under the curve (0.754).
Discussion
To our knowledge, the present study is the first prospective registry study to focus on the haemodynamic mechanisms involved in the angiographic outcome of aneurysms after endovascular treatment. Our series included 165 consecutive patients (177 intracranial aneurysms) with at least one angiographic follow-up, including both patients who underwent conventional treatment (coiling and stent-assisted coiling) and those who underwent flow diverter treatment. This helped us to comprehensively evaluate and explore the real predictive factors that are associated with aneurysm outcomes by eliminating confounding factors. In this prospective study, we found that the RR of velocity at the aneurysm neck was the only independent significant factor for both short-term follow-up and midterm follow-up. This may be due to the optimal treatment strategies that were used in the study era with various treatment methods and devices.
Key results and interpretation
Many factors are reportedly associated with the aneurysm angiographic outcome after endovascular treatment. Some of these factors have been used in clinical practice to evaluate outcomes, and their efficacy has been proven during follow-up. Morphological factors such as the aneurysm size, treatment method (eg, stent-assisted or not) and embolisation results (eg, dense packing or not) are regarded as key factors associated with angiographic outcomes.3 5 23 24 However, none of these factors showed a significant relationship with the angiographic outcome in the present prospective study. After the Cox regression analysis, the RR of velocity at the aneurysm neck was the only independent significant factor for angiographic outcome in both short-term follow-up and midterm follow-up.
The results of the present study may reveal the common mechanism underlying aneurysm outcomes regardless of the aneurysm size, the treatment method used, or whether dense packing is performed in this new age of endovascular treatment. We believe that this may be due to more rational treatment decisions and options, especially after the flow diverter was introduced for the management of large or giant aneurysms in the last decade.5–7 Before the flow diverter, a large or giant aneurysm was a problem for neurointerventionalists.12 25 This is because most previous studies did not include flow diverter cases in the analysis. After the application of flow diverters, treatment decisions have become more optimised. The reported rate of complete occlusion of aneurysms after flow diverter treatment is about 90%. Under this benefit, aneurysms of various sizes have been treated accordingly by different optimal methods, and the overall outcome has therefore improved. This is why the aneurysm size was not a significant predictor in the present study, and we do not believe that it will be a key factor of the angiographic outcome in the future.
Our results also suggest why the treatment method was not associated with the angiographic outcome in the present study. Treated by conventional endovascular embolisation (coiling and stent-assisted coiling), the small aneurysms could usually achieve favourable angiographic outcome. However, the recurrence rate was relatively high for the large or giant aneurysms treated by conventional treatment.26 Right now, treated by flow diverter, the large or giant aneurysms could also achieve favourable angiographic outcome which is as good as the results of small aneurysm treated by conventional embolisation.27–29 Therefore, the aneurysms could be well managed by the optimal treatment method according to the different aneurysm size, location or other morphological features. In our present study, the angiographic outcome did not show statistical difference among treatment methods. In our series, treatment-related decisions were made after thorough discussion and consideration. Every patient underwent individualised treatment in order to obtain the best aneurysm outcome. For example, the large aneurysm would not be treated by conventional coiling for the relatively high recurrence rate and flow diverter will be done. Therefore, the differences in the aneurysm outcomes among these treatment methods were not statistically significant.
This is also the reason why the packing density was not associated with the angiographic outcome. For the conventional techniques, high packing density is one of the key factors to prevent aneurysm recanalisation.30 On the other hand, dense packing may be not necessary for the cases treated by flow diverter; meanwhile, such cases could also achieve favourable complete occlusion at follow-up. Therefore, the packing density was not the significant predictor in our study.
Generalisability
In the current era of endovascular treatment, predictive factors that were reported in previous studies may lose their capability.12 There may be no need to consider these factors in the future when we treat aneurysms endovascularly. For example, large or giant aneurysms showed a 90% complete occlusion rate after treatment with a flow diverter even no coils were inserted into the aneurysm sac.31 32 All of these results can be attributed to the mechanisms of flow dynamics. Haemodynamic factors are reportedly associated with the angiographic outcome of intracranial aneurysms after endovascular treatment.11 33 However, the relationship has not been studied well, and the evidence from retrospective studies remains weak. In the present prospective study, a large number of consecutive cases was included to perform the computational simulations. Both patients who underwent conventional treatment and those who underwent flow diverter treatment were included to ensure that we obtained the results with less bias. The use of an advanced virtual stenting technique, a patient-specific aneurysm model and inflow boundary conditions also ensured greater accuracy of the results compared with previous haemodynamic studies.
According to our results, the RR of velocity at the aneurysm neck was the only independent significant factor for the angiographic outcome after the Cox regression analysis. Briefly, the aneurysm was prone to having a favourable angiographic outcome if the velocity at the aneurysm neck was reduced significantly after endovascular treatment. Regardless of how large the aneurysm is or what treatment methods are used, the key point is to successfully modify the blood flow at the aneurysm neck.
The present study results remind us that the aneurysm angiographic outcome after endovascular treatment could be further improved by a patient-specific treatment strategy. Using a virtual stenting technique and CFD, we would be able to simulate all kinds of treatment strategies before performing the treatment by different stents or packing densities to identify the optimal technique with highly efficient flow modification. In the future, controlling for the complication rate, we could use a cost-effective method to achieve an effective reduction in velocity at the aneurysm neck, which could lead to the best angiographic outcome for the patients, such as more coil packing or another stent deployment. Such pre-procedure treatment planning and post-procedure haemodynamic assessment could provide us a chance to improve the angiographic outcome.
Limitations
This study had several limitations. First, a study using a multicentre database or a validation study in other centre is needed in the future. Second, similar to most CFD simulations, a rigid wall, laminar flow and Newtonian blood assumptions were used in the present study, and these might have introduced bias; however, the patient-specific settings used in our present research would produce more accurate results. Moreover, the porous media method was used to simulate an ideal coil mass without actual coil configuration and some potential operator factors were difficult to evaluate. We should be aware of these potential impacts.
Conclusion
As the optimal treatment strategy becomes more frequently used in this new era, some previously used factors such as the aneurysm size, treatment method and packing density may not be able to predict the angiographic outcome of intracranial aneurysms. The flow dynamics in the present study showed an independent effect on the angiographic outcome. Successful modification of flow velocity at the aneurysm neck could lead to a favourable angiographic outcome. These results may provide great help in clinical practice in the future.
Data availability statement
Data are available upon reasonable request. In addition to the data published within this article, anonymised data can be obtained by request by any qualified investigator.
Ethics statements
Patient consent for publication
Ethics approval
The ethics committee of our institutes approved this study (KY2016-023-01) and informed consent was obtained from each study patient or their relatives.
References
Footnotes
Contributors ZT performed the statistical analysis and the manuscript writing. WL and KW acquired the data. Yisen Z and Ying Z were responsible for aneurysmal model reconstruction and analysed and interpreted the data. SW was responsible for in-house software exploitation. JK and ZR were responsible for the manuscript editing and revising. XY and JL conceived and designed the research. XY handled funding and supervision.
Funding This work was supported by the National Key Research and Development Plan of China (grant number: 2016YFC1300800), the National Natural Science Foundation of China (grant numbers: 81801156, 81220108007, 81801158 and 81671139), Capital’s Funds for Health Improvement and Research (grant number: 2018-4-1077) and Beijing Hospitals Authority Youth Programme (code: QML20190503).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.