Article Text

Abstract
Objective The aims of this study are to clarify the long-term outcomes of brainstem arteriovenous malformations (AVMs) after different management modalities.
Methods The authors retrospectively reviewed 61 brainstem AVMs in their institution between 2011 and 2017. The rupture risk was represented by annualised haemorrhagic rate. Patients were divided into five groups: conservation, microsurgery, embolisation, stereotactic radiosurgery (SRS) and embolisation+SRS. Neurofunctional outcomes were evaluated by the modified Rankin Scale (mRS). Subgroup analysis was conducted between different management modalities to compare the long-term outcomes in rupture or unruptured cohorts.
Results All of 61 brainstem AVMs (12 unruptured and 49 ruptured) were followed up for an average of 4.5 years. The natural annualised rupture risk was 7.3%, and the natural annualised reruptured risk in the ruptured cohort was 8.9%. 13 cases were conservative managed and 48 cases underwent intervention (including 6 microsurgery, 12 embolisation, 21 SRS and 9 embolisation+SRS). In the selection of interventional indication, diffuse nidus were often suggested conservative management (p=0.004) and nidus involving the midbrain were more likely to be recommended for intervention (p=0.034). The risk of subsequent haemorrhage was significantly increased in partial occlusion compared with complete occlusion and conservative management (p<0.001, p=0.036, respectively). In the subgroup analysis, the follow-up mRS scores of different management modalities were similar whether in the rupture cohort (p=0.064) or the unruptured cohort (p=0.391), as well as the haemorrhage-free survival (p=0.145). In the adjusted Bonferroni correction analysis of the ruptured cohort, microsurgery and SRS could significantly improve the obliteration rate compared with conservation (p<0.001, p=0.001, respectively) and SRS may have positive effect on avoiding new-onset neurofunctional deficit compared with microsurgery and embolisation (p=0.003, p=0.003, respectively).
Conclusions Intervention has similar neurofunctional outcomes as conservation in these brainstem AVM cohorts. If intervention is adopted, partial obliteration should be avoided because of the high subsequent rupture risk.
Trial registration number NCT04136860.
- arteriovenous malformation
- intervention
- brain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Brainstem arteriovenous malformations (AVMs) are defined as AVMs involving the midbrain, pons or medulla. They constitute approximately 2%–6% of all intracranial AVMs1–3 and pose substantial management challenges because of the deep location and involving important eloquent region.4 5 Previous studies reported that 45.4%–92.0% of the brainstem AVMs were presented with haemorrhage, and the haemorrhage often leads to devastating neurological deficits.4–9 However, given the risk of severe postoperative complications for brainstem AVMs, the principal management has traditionally been conservative treatment.10 11 Recently, with the development of intervention technology and operative equipment, brainstem AVMs might have more opportunities to undergo more aggressive treatment regimens.4 5 12 13 The present study retrospectively reviewed 61 brainstem AVMs in our institution to specify the long-term outcomes after different management modalities.
Materials and methods
Study design and participants
We performed a retrospective review of all patients diagnosed with AVMs seen at our institution from September 2011 to October 2017. Written informed consent for collecting clinical information was obtained from each patient at admission. The inclusion criteria were: (1) the diagnosis of AVM confirmed with digital subtraction angiography and/or MRI; (2) patients diagnosed of brainstem AVMs and (3) follow-up more than 2 years. Exclusion criteria were: (1) patients’ concomitant diagnosis of hereditary haemorrhagic telangiectasia; (2) patients missing critical baseline information or those lost to follow-up and (3) patients who received intervention before admission.
Data collection and variable definition
Patient baseline demographic, clinical features and imaging data were collected. Haemorrhage presentation was defined as haemorrhage that could be ascribed to AVM rupture. The definition of eloquent area and deep venous drainage was consistent with the evaluation criteria in Spetzler-Martin (SM) Grading system.10 SM Grading system, Virginia Radiosurgery AVM Scale (VRAS) and Radiosurgery-Based AVM Score (RBAS) were used to predict the long-term neurofunctional outcomes.10 14 15 Associated aneurysms were divided into two categories: flow-related aneurysms and non-flow-related aneurysms.16 Diffuseness was determined from preoperative magnetic resonance angiograms with Time-Of-Flight (TOF) images used to identify intervening brain parenchyma within the nidus. Treatment modality was classified as: conservative management, microsurgery, embolisation, stereotactic radiosurgery (SRS) and embolisation+SRS. The rupture risk was represented by annualised haemorrhagic rate, and the clinical follow-up duration was calculated as the interval between diagnosis to last follow-up for conservative patients or as first treatment to last follow-up in intervention patients. The observational interval of natural history was defined as the first diagnosis of brainstem AVMs to the last follow-up in the conservative group and to the first intervention in the intervention group. Recurrent haemorrhage was defined as any haemorrhage attributable to AVM rupture during the follow-up period. The neurofunctional prognosis was evaluated by modified Rankin Scale (mRS).
Follow-up was conducted at the first 3–6 months and annually after surgery by clinical visit and telephone interview. The evaluation of mRS score was conducted by neurosurgeons who have at least 5 years’ experience of clinical practice and all the images were interpreted by at least two radiologists independently who are with at least 5 years of clinical experience in radiology centre of our institute. Researchers who performed follow-up assessments were blinded to treatment modalities.
Statistical analysis
The categorical variables are presented as counts (with percentages); the continuous variables are presented as the mean±SD. The Pearson χ² test, Fisher’s exact test, Mann-Whitney U test or Kruskal-Wallis test was used to compare categorical variables as appropriate. Two-tailed t-tests or one-way analysis of variance test were employed to compare continuous variables (normal distribution variable). Bonferroni correction was adopted in the adjusted posthoc analysis in order to avoid the occurrence of Type I errors (p<0.005). Wilcoxon rank sum test was applied to compare non-normal distribution continuous variables. A Poisson rate test was used to compare the differences of annualised rupture risk. Kaplan-Meier analysis (Log Rank, Mantel-Cox) was employed to compare the actuarial obliteration rates and haemorrhage-free survival rates between different interventional modalities. P<0.05 was considered to be statistically significant. Statistical analysis was performed using SPSS (V.25.0, IBM, New York, USA).
Results
Baseline characteristics
A total of 61 patients (2.8%) with brainstem AVMs were included from our institutional database of 2212 patients with AVM (figure 1). Forty-nine patients (80.3%) were presented with haemorrhage. Thirteen patients (21.3%) were conservative managed and 48 patients (78.7%) underwent intervention (including 6 cases of microsurgical resection, 12 cases of endovascular embolisation, 21 cases of SRS and 9 cases of embolisation+SRS) (table 1). The mean age was 29.5±14.0 years (range, 3.1–61.0 years), the average size of all brainstem AVMs was 2.4±1.4 cm (range, 0.6–7.0 cm) and the mean admission mRS score were 1.2±1.4. Most of the patients were classified as SM grade II (30 cases, 49.2%) and III (22 cases, 36.1%). The most common VRAS score noted was VRAS=2 (27 cases, 44.3%), followed by VRAS=4 (16 cases, 26.2%) and VRAS=3 (15 cases, 24.6%). The most common RBAS noted was RBAS=1–2 (31 cases, 50.8%), followed by RBAS <1 (19 cases, 31.1%). Of the 61 brainstem AVMs, 30 were located in midbrain (49.2%), 5 in midbrain-pons (8.2%), 10 in pons (16.4%), 3 in pons-medulla (4.9%), 6 in medulla (9.8%), 5 in middle cerebellar peduncle (8.2%) and 2 in other locations (3.3%). Twenty-six patients (42.6%) drained by deep venous and 10 patients (16.4%) were accompanied by flow-related aneurysms. 16.4% were evaluated as diffuse nidus based on TOF images. The majority of patients (45 cases, 73.8%) accompanied with deep perforating arteries. No patients in the SRS group received either planned dose-stage or volume-stage therapy.
Baseline characteristics of the included brainstem AVMs
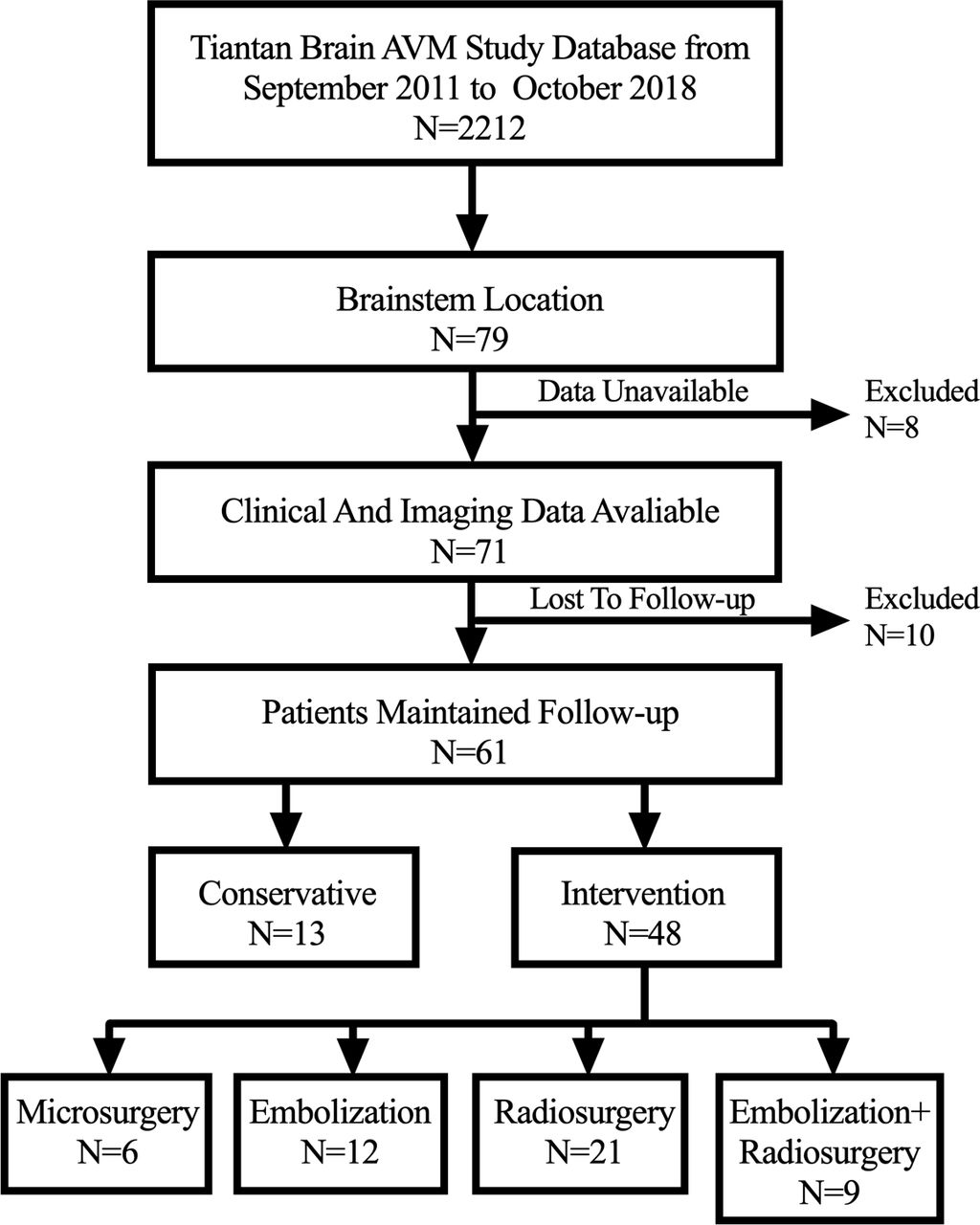
The flow diagram of patient screening. AVM, arteriovenous malformation.
Indication selection
In our institution, the three departments corresponding to the three intervention modalities (microsurgery, embolisation, SRS) are independent of each other, and they all complete the formulation of the patient’s treatment plan independently. Therefore, the selection of indications for each intervention modality may be different. Patients with nidus partial obliteration after embolisation would be recommended for SRS, but the patient compliance was not consistent.
In this study, diffuse nidus were often suggested conservative management because of the unclear boundaries (46.2% vs 8.3%, p=0.004, OR 9.429, 95% CI 2.113 to 42.069) and nidus involving the midbrain were more likely to be recommended for intervention (23.1% vs 56.3%, p=0.034, OR 0.233, 95% CI 0.057 to 0.956). In the adjusted posthoc Bonferroni correction analysis, the baseline characteristics were similar between these five management modalities (table 2).
Indication selection of different management strategies for brainstem AVMs
Annual rupture risk
All of 61 brainstem AVMs were continuously followed up clinically and angiographically with an average of 4.5±2.0 years. In the nature history analysis, seven patients in the ruptured cohorts and zero patients in occurred rupture event during the observational interval (one case in the conservation group experienced one rerupture event and six cases in the intervention group experienced seven rerupture events before clinical invasive intervention). The observational interval of nature history was 109.7 patient-years, indicating a natural annualised rupture rate of 7.3%. In the ruptured cohorts, the total follow-up time before the initial intervention was 89.7 patient-years, indicating an natural annualised rerupture rate of 8.9%. The overall follow-up duration of the conservation group was 65.5 patient-years, indicating an annualised subsequent rupture rate of 1.5%. Seven cases (14.6%, three in the embolisation, three in the SRS and one in the embolisation+SRS) in the intervention group experienced a total of eight subsequent haemorrhages during a follow-up period of 207.4 patient-years, indicating an annualised subsequent rupture rate of 3.9% in the intervention group (0.0% in the microsurgery, 9.7% in the embolisation, 3.5% in the SRS and 2.1% in the embolisation+SRS) (conservation versus intervention, 1.5% vs 3.9%, p=0.410, 95% CI −0.063 to 0.017). Interestingly, we found that partial obliteration has significant higher subsequent rupture risk than complete obliteration (10.6% vs 0.0%, p<0.001, 95% CI 0.032 to 0.179) and conservative management (10.6% vs 1.5%, p=0.036, 95% CI 0.011 to 0.170), and similar subsequent rupture risk with natural annualised rupture risk (10.6% vs 7.3%, p=0.465, 95% CI −0.056 to 0.122) (table 3).
Natural annualised rupture risk and annualised subsequent rupture risk under different treatment modalities in brainstem AVMs
Subgroup analysis
All of six AVMs were totally resected in the microsurgery group. Three patients (50.0%) were operated by posterior median suboccipital approach, and the other three patients (50.0%) were treated by Kawase approach. After the operation, three patients (50.0%) occurred persistent partial motor aphasia and one patient (16.7%) experience new-onset limb weakness. Five patients (41.7%) in the embolisation group achieved angiographic obliteration. However, three patients (25.0%) experienced long-term disability and four patients (33.3%) died (three died of recurrent haemorrhage, one died of medulla infarction) during follow-up. Radiosurgery was applied in 21 cases, and 13 of them (61.9%) achieved angiographic obliteration during a mean follow-up period of 4.0±1.8 years. Four patients (19.0%) underwent SRS procedures twice. The margin dose was 15.1±1.6 Gy (range, 12–18 Gy). New-onset neurofunctional deficit occurred in three patients (14.3%) because of recurrent haemorrhage during follow-up. In the embolisation+SRS group, four of them (44.4%) achieved obliteration. One patient (11.1%) experienced once subsequent haemorrhage after 5.6 years follow-up and finally died.
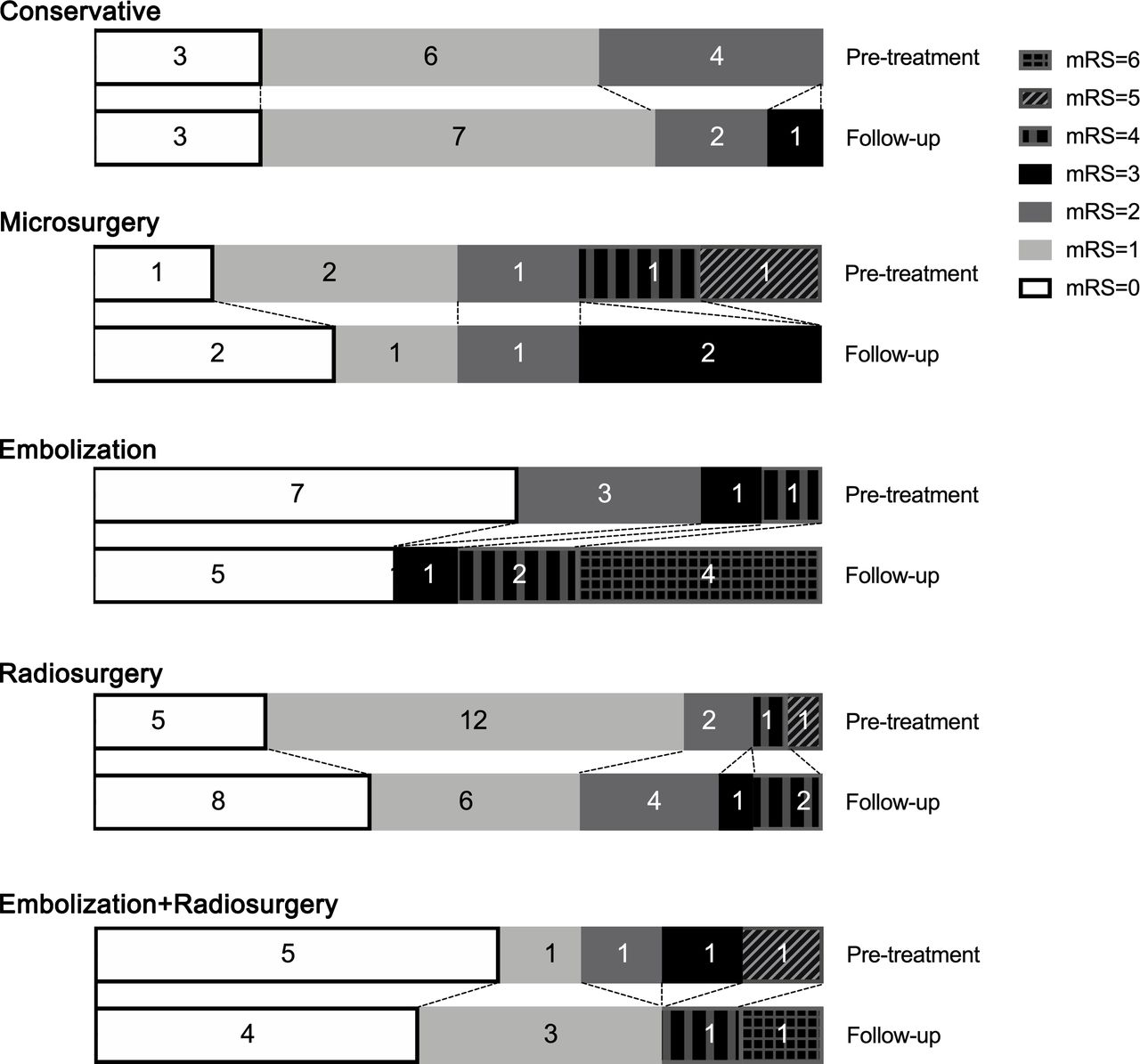
In the subgroup analysis of long-term outcomes in ruptured and unruptured brainstem AVMs, despite the long-term mRS were similar between different management modalities both in the rupture group (p=0.064) and unruptured group (p=0.391) (figure 2), there were differences in several prognostic indicators (table 4). In the ruptured cohort, the obliteration rate of different management modalities was not the same (p<0.001). The adjusted posthoc Bonferroni correction analysis indicated that both microsurgery and SRS could achieve statistical significant obliteration rate than conservative management (p<0.001, 95% CI NA; p=0.001, 95% CI 1.529 to 8.012, respectively). The new-onset neurofunctional deficit in the rupture cohort was not the same too (p=0.001). The adjusted posthoc Bonferroni correction analysis showed that SRS has a positive effect on avoiding new-onset neurofunctional deficit compared with microsurgery and embolisation (p=0.003, 95% CI 2.188 to 29.249; p=0.003, 95% CI 1.791 to 8.064, respectively). In addition, although there may be differences in the overall distribution of mortality between different management modalities in the rupture cohort (p=0.019), we found no significant differences in mortality between any two management modalities after adjusted Bonferroni correction analysis. In the unruptured cohort, we did not find any differences in all prognostic indicators. Kaplan-Meier analysis showed no significant difference in cumulative obliteration rate between SRS group and embolisation+SRS group (p=0.439) (figure 3), as well as in haemorrhage-free survival between different management modalities (p=0.145).
Subgroup analysis of ruptured versus unruptured brainstem AVMs underwent conservative versus different intervention management
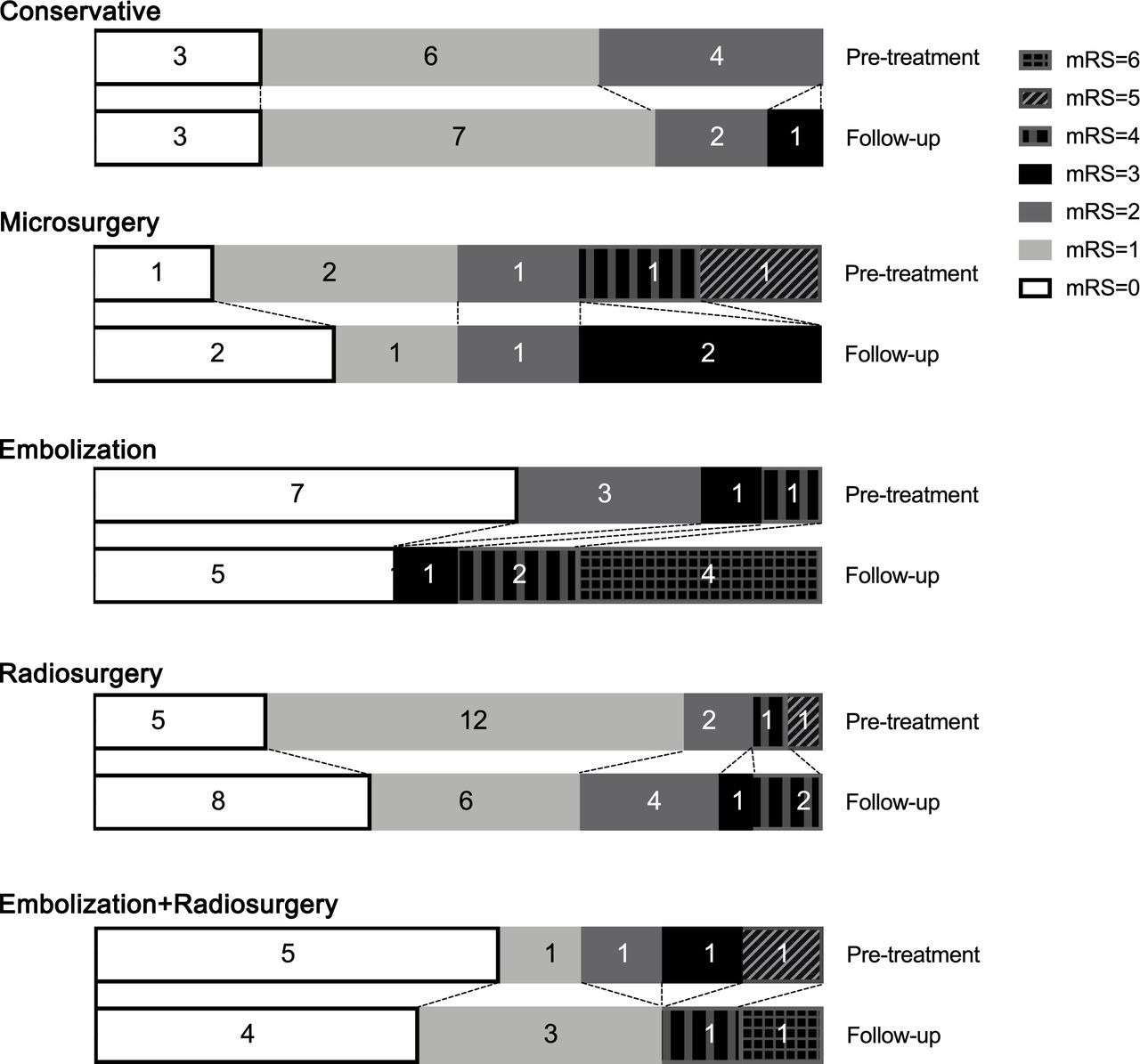
mRS scores of brainstem AVMs before and after conservation, microsurgery, embolisation, SRS and embolisation+SRS. AVM, arteriovenous malformation; mRS, modified Rankin Scale; SRS, stereotactic radiosurgery.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier plot. (A) Cumulative obliteration rates were similar between SRS group and embolisation+SRS group (p=0.439, log-rank test). (B) There was no significant difference in haemorrhage-free survival between different management modalities (p=0.145, log-rank test). SRS, stereotactic radiosurgery.
Discussion
Brainstem AVMs are a rare subset of vascular malformations that have been incompletely characterised and the most appropriate management remains unclear. This study is currently the largest sample size study of different management modalities in brainstem AVMs. In the present study, we included 61 brainstem AVMs (13 conservative cases and 48 intervention cases). Our results confirm that intervention has similar neurofunctional outcomes as conservative treatment in this brainstem AVMs cohorts. If intervention is adopted, partial obliteration should be avoided because of the high subsequent rupture risk. In the subgroup analysis, although the long-term mRS and haemorrhage-free survival were similar between different management modalities both in the rupture cohort and the unruptured cohort, microsurgery and SRS could significantly improve the obliteration rate compared with conservation in the rupture cohort, and SRS has a positive effect on avoiding new-onset neurofunctional deficit compared with microsurgery and embolisation in the rupture cohort.
General characteristics and natural history
The rate of brainstem AVMs in the whole cerebral AVMs cohort has been reported as 2.0%–6.0%.1–3 In the present study, the incidence was 3.6%. The majority of the brainstem AVMs were presented with haemorrhage (80.3%), which is slightly higher than previous literature (53.3%–79.0%).9 17 In addition to haemorrhage, the most common symptom is non-specific symptoms such as dizziness and headache. The mean ages in this study were 29.5±14.0 years, which is consistent with previous studies (30–54 years).4–8 The classification of brainstem AVM location was diverse in previous studies. Han et al 4 proposed a six classification schemes based on the lesion location (anterior midbrain, posterior midbrain, anterior pontine, lateral pontine, anterior medulla and lateral medulla), which could be applicable to different resection procedures and different outcomes.4 And many SRS studies applied the three-grading system (midbrain, pons, medulla).5 6 13 17–19 However, a significant proportion of patients have lesions at the junction or across multiple areas, which will lead to severe deviation in the location evaluation. In this study, we isolated the overlapping lesions and found that most of the nidus (49.2%) were located in midbrain and 24.6% were located in the junction area. The distribution of lesion location was consistent with most previous studies.5 6 13 17–19 Deep venous drainage was previously reported to be extremely common in brainstem AVMs (82.8%–89.8%).4 6 9 However, in this study, we found that some lesions had low filling of lesion contrast media and no obvious drainage veins in the pretreatment imaging examinations. Since slower blood flow velocity and transit time imply lower rupture risk,20 we adopt a conservative attitude in assessing the deep venous drainage of these patients. Finally, the percentage of deep venous drainage in this study was 42.6%. The natural annualised rupture risk of brainstem AVMs in this study was 7.3%, and the natural annualised reruptured risk in the ruptured cohort was 8.9%, which was consistent with previous brainstem AVM studies (4.8%–9.8%).9 17 21 22
Microsurgical resection
AVMs are under a significantly cumulative life-time risk of intracranial haemorrhage, and complete resection or obliteration should be the first-line treatment for AVMs. However, considering the important function and the complex anatomy of the brainstem, an aggressive and safe microsurgical resection can present at times an unrealistic challenge. Rare incidence and limited experience prevented the microsurgical exploration of brainstem AVMs.2 4 5 It was reported that 5%–12% of patients with brainstem AVM would experience poor outcomes after resection.1 3 4 8 10 Many previous studies promoted different categorisations for brainstem AVMs based on the lesion locations to predict the risk of postoperative complications and long-term outcomes.8 Nozaki et al suggested that acceptable surgical risk can be achieved from AVMs located in the dorsal midbrain and cerebellopontine angle after retrospectively reviewing 19 brainstem AVMs undergoing surgical resection.8 In contrast, Han et al proposed a six categorisation system and indicated that the most favourable lesions for resection are lateral pontine and lateral medullary AVMs because of preferable exposure and corridor of manoeuvre.4 In addition, they proposed a technique of ‘occlusion in situ’ for those AVMs that cannot be separated cleanly from the brainstem. In this study, two patients (33.3%) got worsened mRS and both of these two patients involved the medulla and operated by the posterior median suboccipital approach. Aphasia (50.0%) and limb weakness (50.0%) were the most common postoperative complications. We thought that although a higher risk of postoperative complications compared with other modalities, microsurgery remained an effective option for patients with emergent haematoma compression because of the immediate control of the haematoma and the high obliteration rate.9 However, individualised resection strategies based on lesion location and craniotomy approach are necessary in order to avoid severe postoperative complications.
Embolisation
Endovascular embolisation could occlude the rupture risk factors of AVMs to decrease the risk of haemorrhage, such as flow-related aneurysms and arteriovenous fistulas.23 Previous studies reported that targeted embolisation might be the most favourable strategy in the endovascular management for brainstem AVMs.7 24 In this study, no patients underwent target embolisation and five patients (41.7%) achieved completely obliteration. Unfortunately, three patients (25.0%) died of recurrent haemorrhage during follow-up and one (8.3%) patient died of postoperative medulla infarction. The postoperative mortality was higher than the other three interventional modalities. One previous study indicated that brainstem AVMs with incomplete nidus obliteration are at high risk of future rupture and feeding arterial or intranidal aneurysms might increase the risk of haemorrhage.25 In the present study, the annualised rupture risk of partial obliteration was 10.6%, similar with that of natural annualised rupture risk (7.3%), but significantly higher than complete obliteration (0.0%) and conservative management (1.5%). Four cases (33.3%) in the embolisation group were accompanied with flow-related aneurysms and all of them were embolised. However, the recurrent haemorrhagic events still occurred; the potential mechanism might be the increased haemodynamic stress in the nidus after incomplete obliteration.25 26
Radiosurgery and embolisation+SRS
Radiosurgery was increasingly recognised as a preferred treatment for brainstem AVMs,5 6 13 17–19 especially in small to moderate-sized and compact nidus.2 5 15 Cohen-Inbar et al investigated 134 brainstem AVMs in a multicentre study, and they calculated a 3-year actuarial obliteration rate of 62.3%, with 64.4% of all patients demonstrating favourable outcomes.6 In this study, 61.9% of the patients in the SRS group were proved obliterated and 66.7% of the patients got favourable outcomes after an average of 48.5-month follow-up. Most previous SRS series recommended a margin dose of 20–24 Gy (range 11.5–30 Gy) for brainstem AVMs,5 6 13 19 and obliteration occurred earlier in patients who got a higher prescribed margin dose and maximum dose.6 However, the latency period haemorrhage before obliteration and radiation-induced complications (RICs) might limit the application of higher margin dose SRS.15 In this study, the margin dose was 15.1±1.6 Gy (range, 12–18 Gy). No study has found differences in ethnic sensitivity to the radiation doses. Previous studies (21–24 Gy) reported that the annual postgamma knife latency period haemorrhage was 1.5%, and the rates of radiological and symptomatic RIC were 35.6% and 14.6%.6 In this study, the annualised rupture risk after SRS was 3.5% and the rate of symptomatic RIC was 4.8%. The symptomatic RIC was significantly lower than previous higher dose series. As such, an optimal dose balancing the obliteration rate and post-SRS RIC should be further explored in future study. Recently, pre-SRS embolisation has been proposed to decrease the intranidal flow and nidus volume.5 27 However, the pre-SRS embolisation remains controversial and it was previously demonstrated to have a negative impact on obliteration rate in many SRS series.15 28 29 In this study, nine patients underwent embolisation+SRS, and the obliteration rate and complication rate were consistent with single-modality strategy of SRS.
Several potential limitations of this study should be noted. First, the small sample size might reduce the power of our conclusions. Nevertheless, to the best of our knowledge, this is the largest study to investigate different management modalities in brainstem AVMs. The conclusion of this study plays an important role in guiding the selection of management modalities for brainstem AVMs. Second, rare incidence and limited experience may affect the neurofunctional outcomes after intervention. Third, the conservative group had a smaller proportion in the entire cohort, which may increase the error caused by individual bias. Future studies are required to organise multicentre trial to assess the optimal management strategy for brainstem AVMs.
Conclusion
Brainstem AVMs are dynamic and complex vascular malformations that require comprehensive consideration of the patients’ clinical presentations and angioarchitecture. We observed similar neurofunctional outcomes and annualised rupture risk between the conservative and different interventive modalities. Partial obliteration should be avoided because of the high subsequent rupture risk.
Acknowledgments
We thank the Multidisciplinary Team of Cerebrovascular Diseases in Beijing Tiantan Hospital.
References
Footnotes
Contributors YC and LM contributed to conception and design of the study. YC, RL, LM, XM and DY organised the database. YC and DY performed the statistical analysis. YC wrote the first draft of the manuscript. HW, XY, HJ, YL, DG, SS, AL, SW, XC and YZ critically revised the manuscript and approved the final manuscript as submitted. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was supported by Natural Science Foundation of China (81571110, 81771234 to YZ; 81500995 to XC; 81801140 to LM) and Bai Qian Wan Talent Plan (2017A07).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review boards at both institutions (Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China and Department of Neurosurgery, Peking Unversity International University, Peking University, Beijing, China) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Any subscribers who are interested in our database can send email requests to authors Yu Chen (chenyu_tiantan@126.com). Thanks.