Article Text

Abstract
Background and purpose Early neurological deterioration (END) is a common feature in patients with acute ischaemic stroke (AIS) receiving thrombolysis. This study aimed to investigate whether the presence of multiple hypointense vessels (MHVs) on susceptibility-weighted imaging (SWI) could predict END in patients with the anterior circulation AIS treated with recombinant tissue plasminogen activator (r-tPA).
Methods This was a retrospective study focusing on AIS patients suffering from symptomatic stenosis or occlusion of the middle cerebral artery or internal carotid artery with r-tPA treatment. We collected clinical variables and initial haematological and neuroimaging findings. MHVs were measured on SWI performed after intravenous thrombosis and were defined as the presence of a greater number of veins or veins of a larger diameter with greater signal loss on SWI than those of the contralesional haemisphere. The degree of hyperintensity of MHVs was classified into four grades: none, subtle, moderate and extensive. END was defined as an increase in the National Institutes of Health Stroke Scale score by 2 points during the first 48 hours after the onset of symptoms. Multivariate logistic regressions were conducted to investigate the predictors of END.
Results The study included 61 patients (51 males and 10 females) with a mean age of 62.4±12.6 years. Thirty-five (57.4%) patients presented with MHVs: 8 (13.1%) were graded as subtle MHVs, while 23 (37.7%) and 4 (6.6%) were graded as moderate or extensive MHVs, respectively. Twenty patients (32.8%) presented with END. Logistic regression analysis showed that compared with patients without MHVs, moderate MHVs (adjusted OR 5.446, 95% CI 1.360 to 21.800; p=0.017) and extensive MHVs (adjusted OR 15.240, 95% CI 1.200 to 193.544; p=0.036) were significantly associated with END.
Conclusions MHVs might be a useful predictor of END in AIS patients with symptomatic large artery stenosis or occlusion after r-tPA treatment.
- stroke
- MRI
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Early neurological deterioration (END) has been reported to be related to a poor outcome and occurs commonly in patients suffering from acute ischaemic stroke (AIS).1 According to the literature, the incidence of END in AIS patients varies from 16.3% to 37.5%.2–5 Some biomarkers of END are identified in recent years, including the fibrinogen level,3 hyperglycaemia,6 homocysteine,7 serum triglyceride8 and D-dimer levels.9 In addition, several imaging markers are associated with END, including computed tomographic signs of cerebral oedema,5 lacunar strokes10 and severe large artery stenosis and occlusion.2 Other studies have demonstrated that large vessel disease11 12 and a lack of recanalisation13 are good predictors for the occurrence of END after intravenous thrombolysis (IVT).
Susceptibility-weighted imaging (SWI) is a MRI sequence that is highly sensitive to paramagnetic materials, including deoxyhaemoglobin and haemosiderin.14 15 The cerebral veins can be seen more prominently on SWI as multiple hypointense vessels (MHVs) in acute ischaemic cerebral haemispheres.16 17 A previous study indicated that the presence of MHVs was a novel marker for predicting END in AIS patients.18 However, not all patients in this earlier study were suffering from severe intracranial large artery stenosis or occlusion (ILASO), which are factors highly correlated with both MHVs and END.19 Previous studies have found that the presence of MHVs was related to a poor outcome in AIS patients with ILASO, which suggested that MHVs might be predictive of outcomes in patients with ILASO.20 21 A growing body of evidence currently suggests that the perfusion status of ischaemic brain regions is also associated with END in AIS patients11 22 23; furthermore, SWI can detect the regional perfusion status in an efficient but indirect manner.16 Thus, we hypothesised that the presence of MHVs could also be a useful predictive marker for END in such patients.
However, to our knowledge, a few studies have investigated the specific relationship between the presence of MHVs and END in patients with anterior circulation AIS treated with IVT. Therefore, we aimed to evaluate the effects of MHVs on END in patients with AIS in the anterior circulation suffering from stenosis or occlusion of the symptomatic middle cerebral artery (MCA) or internal carotid artery (ICA) following IVT therapy.
Methods
Patients
We prospectively recruited AIS patients who received recombinant tissue plasminogen activator (r-tPA) IVT therapy in Dongguan People’s Hospital between 1 January 2016 and 31 October 2019. We then retrospectively analysed data from all subjects receiving thrombolysis. The inclusion criteria were as follows: (1) age >18 years, (2) treatment with r-tPA within 4.5 hours of onset of stroke symptoms, (3) prestroke modified Rankin Scale score ≤1 and (4) symptomatic severe ILAS or occlusion confirmed by MR angiography (MRA). Patients were excluded according to the following criteria: (1) MRI-confirmed AIS of the posterior circulation, (2) parenchymatous haemorrhage (PH) evident on CT following END, (3) lack of SWI data, (4) severe ILASO contralateral to the infarction and (5) direct thrombectomy or thrombectomy following IVT.
Because visual comparison of the severity of signal loss between haemispheres is essential during MHVs assessment, it follows that severely compromised contralateral haemodynamics could, in theory, render vessel signs less obvious. Therefore, we excluded subjects with severe contralateral ICA/MCA stenosis or occlusion. In addition, because it is difficult to assess MHVs on SWI in patients with haematoma within the infarction, we also excluded patients with PH transformation.
All subjects provided informed consent in accordance with the Declaration of Helsinki.
Clinical data collection
We acquired clinical data from each patient, including the National Institutes of Health Stroke Scale (NIHSS) score, onset to treatment time (OTT), demographic data including age, sex, history of hypertension, diabetes mellitus, smoking, atrial fibrillation, and previous stroke, and initial haematological findings including the homocysteine level, blood glucose (BG) level on admission and neutrophil to lymphocyte ratio.
Clinical outcomes
END was defined as an increase in the NIHSS score by 2 points24 during the first 48 hours after the onset of symptoms. A second CT scan was performed when END occurred to confirm whether PH was evident.
Imaging analysis
Brain MRI following IVT was performed within 72 hours of the onset of stroke for each patient, including T1-weighted imaging, T2-weighted imaging, fluid-attenuated inversion recovery, diffusion weighted imaging (DWI), SWI and three-dimensional time-of-flight MRA (3D-TOF-MRA). All scanning was carried out with a 3.0 T system (Skyra, Siemens Medical, Erlangen, Germany). The parameters for each sequence are shown in table 1.
The parameters for each sequence of MRI scan
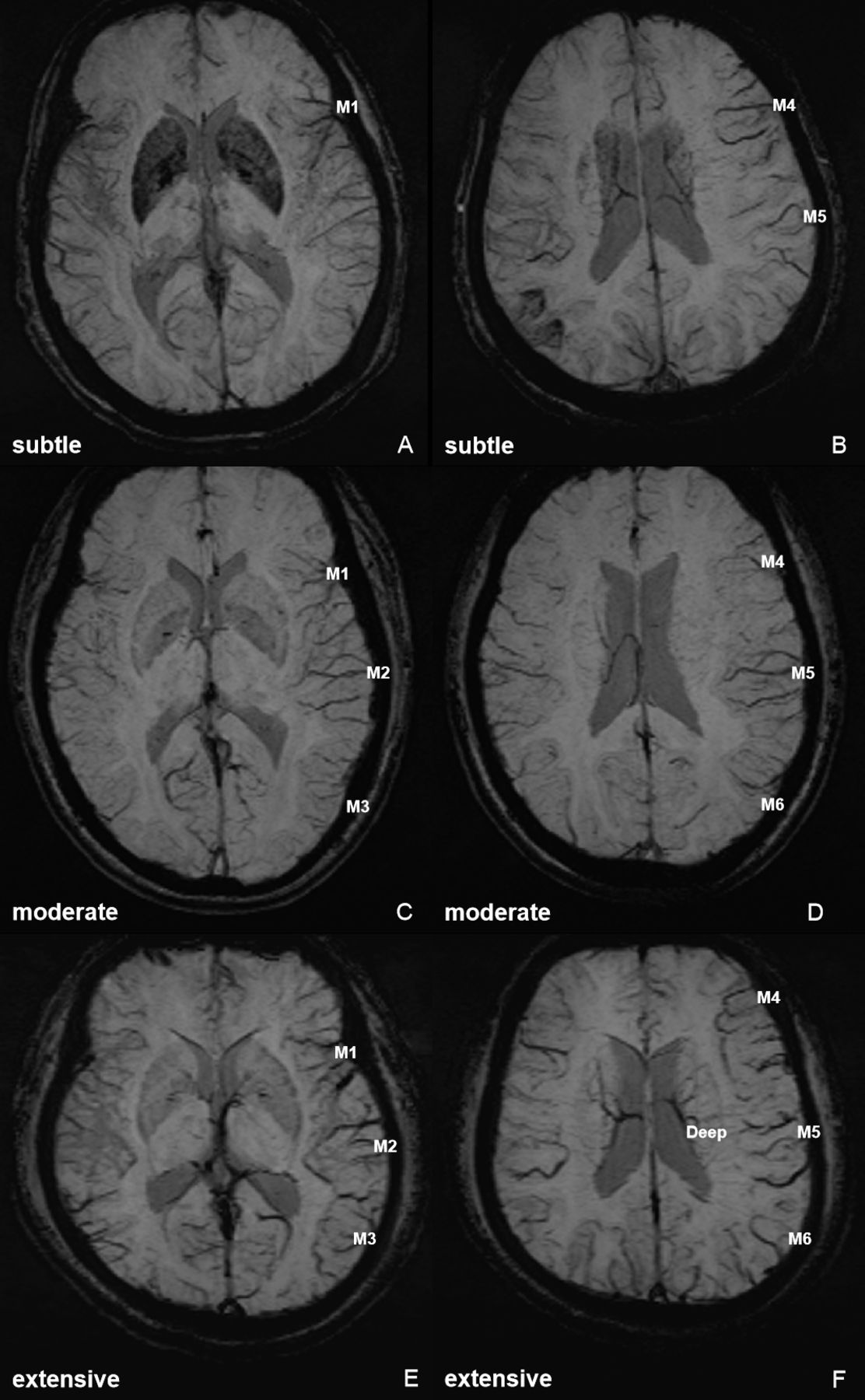
MHVs were measured on SWI scans performed following IVT and were defined as a greater number of veins or larger veins with greater signal loss on SWI than those of the contralesional haemisphere.25 According to a previous study,25 MHVs were classified into four grades, based on the number of defined areas occupied (according to the Alberta Stroke Programme Early CT (ASPECT) score.26 The defined areas were as follows: ‘Ins’, ‘M1’, ‘M2’, ‘M3’, ‘M4’, ‘M5’, ‘M6’ and ‘Deep’. The criteria used for the classification of the MHV grade were as follows: (1) ‘none’, no MHVs in any MCA territory; (2) ‘subtle’, MHVs in 1–3 defined areas of the MCA territory; (3) ‘moderate’, MHVs in 4–6 defined areas of the MCA territory; or (4) ‘extensive’, MHVs in 7–8 defined areas of the MCA territory. A figure demonstrating the assessment of MHV grades is included in the supplemental materials (online supplementary figure S1).
Supplemental material
ILASO was evaluated by 3D-TOF-MRA. Symptomatic severe ILAS was defined as cases involving the ICA or M1 segment of the MCA ipsilateral to the infarction with a diameter loss >70%. Symptomatic intracranial large artery occlusion (ILAO) was defined as signal loss of distal blood flow ipsilateral to the infarction. Intracranial stenosis or occlusion was assessed using the Warfarin Aspirin Symptomatic Intracranial Disease criteria.27 PH was assessed according to The European Cooperative Acute Stroke Study II criteria28 by repeated CT scans performed after END onset. The DWI-ASPECT score29 and small vessel disease (SVD) score30 (based on T2-weighted imaging and SWI) were also measured. CT angiography (CTA) or digital subtraction angiography (DSA) were not conducted regularly and were performed depending on the decision of the attending physician.
Two experienced neuroradiologists specialised in MRI (M-QL, an associate consultant with 15 years of experience in neuroradiology; FW, with 10 years of experience in neuroradiology), who were blinded to the clinical information of patients, independently evaluated the imaging findings for each subject, including PH, the DWI-ASPECT and SVD scores, and the severity of ILASO and MHVs. The two observers reviewed and discussed the cases for which agreement was not reached, and the final decisions were made by M-QL.
Statistical analysis
Statistical analyses were conducted using SPSS for Windows (V.20.0, IBM). Continuous variables with a normal distribution are reported as means (with SD), while non-normally distributed variables are reported as the median and IQR. Judgements of the inter-rater and intrarater agreements of measurement of MHVs were made based on Kappa test.
All subjects were divided into two groups with regard to END. Variables were compared between the groups using t-tests, Mann-Whitney U tests, Pearson χ2 tests or Fisher’s exact tests, as appropriate. Variables for which p≤0.1 in the univariate analysis were subsequently included in further binary multivariate logistic regressions. Statistical significance was defined as p<0.05 (two sided).
Results
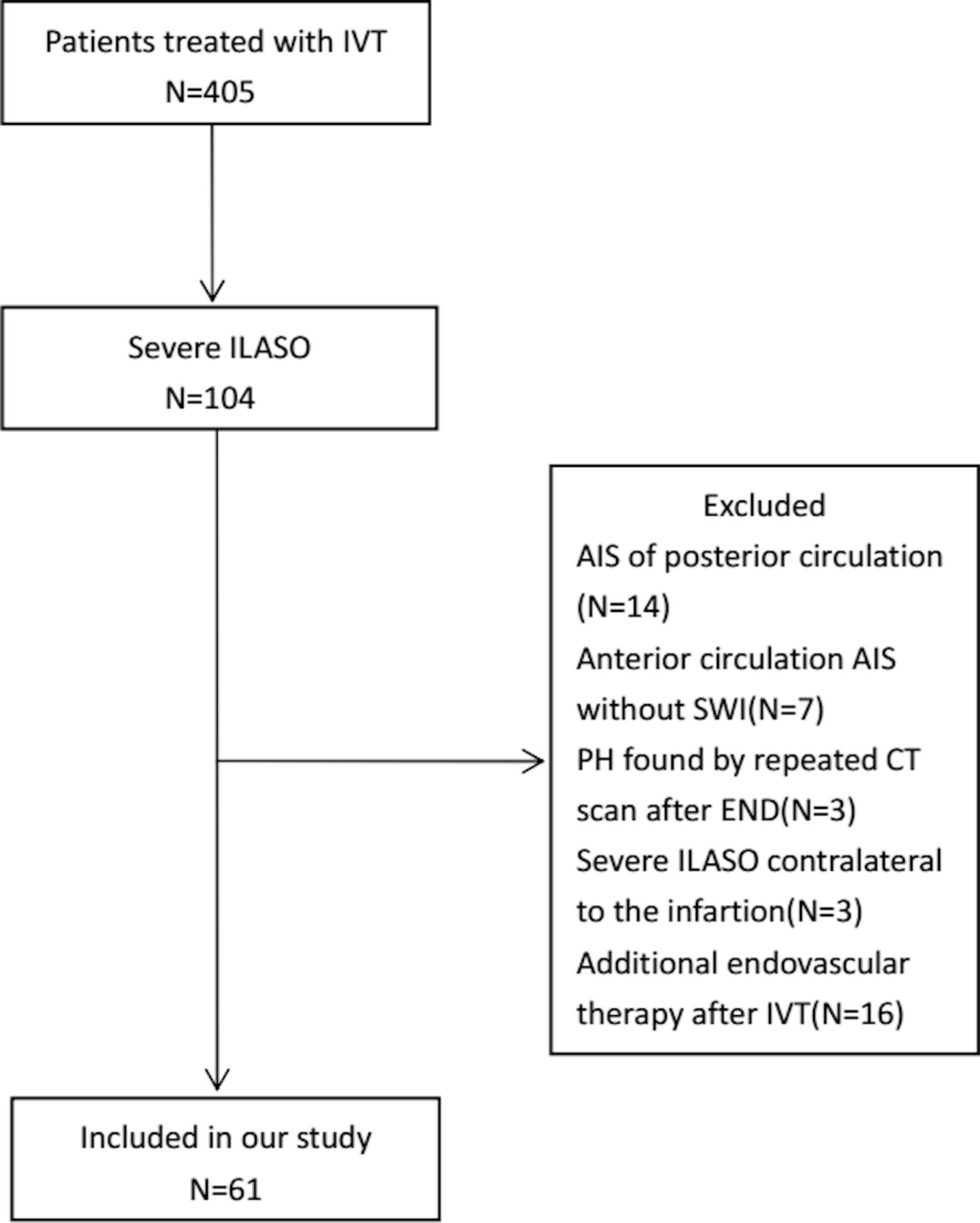
During the study period, 405 consecutive patients were treated with r-tPA IVT within 4.5 hours of the onset of stroke. Of these 405 patients, 104 were diagnosed with severe ILASO by MRA. Of these 104 patients, 43 were excluded because of AIS of the posterior circulation (n=14), AIS of the anterior circulation with no SWI data (n=7), detection of PH by repeat CT scanning following END (n=3), severe ILASO contralateral to the infarction (n=3) and additional endovascular therapy after IVT (n=16). Therefore, 61 patients with a mean age of 62.4±12.6 years were included in our final analysis. Twenty-three patients underwent CTA examinations, and two patients underwent DSA examinations. There were no significant differences between the included and excluded patients in terms of age (62.4±12.6 years vs 61.3±12.4 years, p=0.665), sex (male, 51 (83.6%) vs 31 (72.1%), p=0.157), NIHSS score on admission (median (25–75 IQR), 9 (5–14) vs 8 [6–13], p=0.979) or OTT (203.5±54.1 min vs 189.8±58.5 min, p=0.221).
A comparison between patients with ILAS and those with ILAO indicated no significant differences in terms of age (63.5±11.6 vs 60.9±14.0 years, p=0.433), sex (male, 28 (80.0%) vs 22 (84.6%), p=0.745), and NIHSS score on admission (median (25–75 IQR), 9.0 (5.0–15.0) vs 10.5 (5.8–17.3), p=0.971); patients with ILAO had more severe MHVs than those with ILAS (from none to extensive, 7 patients (26.9%), 4 patients (15.4%), 12 patients (46.2%) and three patients (11.5%), respectively, vs 19 patients (54.3%), 4 patients (11.4%), 11 patients (31.4%) and one patient (2.9%), p for trend=0.027); patients with ILAO were also more likely to have END (13 patients [50%] vs 7 patients (20%), p=0.014). During the study period, 24 patients with large artery occlusion were treated by direct thrombectomy; these patients had a mean age of 66.3±10.3 years and a median NIHSS score on admission of 13 (11–17.75); 16 of these patients (66.7%) were male. A flow chart of the selection process is shown in figure 1.
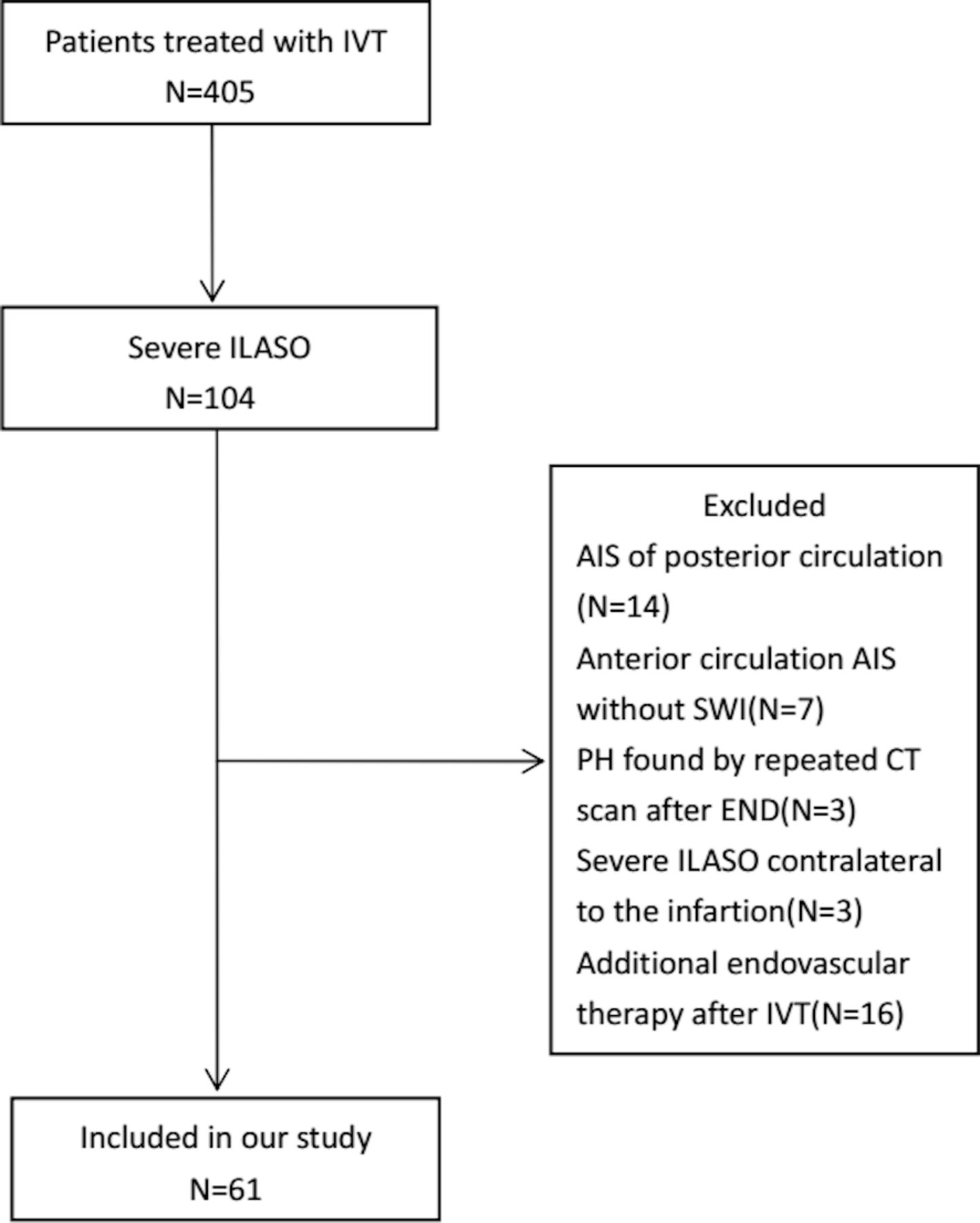
Flow chart of the process used to select subjects. AIS, acute ischaemic stroke; END, early neurological deterioration; ILASO, intracranial large artery stenosis or occlusion; IVT, intravenous thrombolysis; SWI, susceptibility-weighted imaging; PH, parenchymatous haemorrhage.
The median interval between stroke onset and MRI scanning was 42 hours (range, 13–65 hours). Thirty-five patients (57.4%) had severe ILAS (31 patients (50.8%) involving the MCA and 4 patients (6.5%) involving the ICA) and 26 patients (42.6%) had ILAO (17 (27.9%) involving the MCA and 9 (14.8%) involving the ICA). Thirty-five (57.4%) patients presented with MHVs (with grades classified as being ≥subtle) on SWI including 8 (13.1%) graded as subtle, 23 (37.7%) graded as moderate and 4 (6.6%) graded as extensive. The measurement agreement of MHVs was judged to be good (inter-rater kappa value: 0.81; intrarater kappa value: 0.85). Twenty (32.8%) patients presented with END. Three typical cases of MHVs, graded as subtle, moderate and extensive, are shown in figure 2. The demographic and clinical characteristics of this study sample are shown in table 2.
{kind=link}
{kind=link}
(1) The case of a 74-year-old woman who suffered from AIS for 2 hours. In the left haemisphere, MHVs in M1 (A), M4 and M5 (B) were evident on SWI, and defined as subtle MHVs. (2) The case of a 68-year-old woman who suffered from AIS for 3 hours. In the left haemisphere, MHVs in M1, M2, M3 (C) and M4, M5, M6 (D) were evident on SWI, and defined as moderate MHVs. (3) The case of a 42-year-old man who suffered from AIS for 2 hours. In the left haemisphere, MHVs in M1, M2, M3 (E) and M4, M5, M6, Deep (F) were evident on SWI, and defined as extensive MHVs. AIS, acute ischaemic stroke; Deep, deep white matter; MHVs, multiple hypointense vessels; M1, anterior MCA cortex; M2, MCA cortex lateral to the insular cortex; M3, posterior MCA cortex; M4, M5, M6, the anterior, lateral and posterior MCA territories immediately superior to M1, M2 and M3; MCA, middle cerebral artery; SWI, susceptibility-weighted imaging.
Demographic and clinical characteristics of the study cohort
Univariate analysis
Compared with those without END, patients who presented with END had significantly higher BG levels (7.3±2.7 vs 6.3±1.1, p=0.041, crude OR 0.759), a significantly longer OTT (221.6±46.8 vs 194.7±55.9, p=0.048, crude OR=1.010), and significantly more severe MHVs (moderate, 11 (55.0%) vs 12 (29.3%), crude OR=5.042; extensive, 3 (15.0%) vs 1 (2.4%), crude OR=16.500) (p=0.003) . The results derived from comparisons between patients with and without END are shown in table 3.
Risk factors of END determined by univariable analysis
Multivariate logistic regression
Variables identified to show significant differences between the two groups (p≤0.1) in the univariable analysis, including the OTT, NIHSS score on admission, BG level on admission and MHVs as well as age and sex were subsequently entered into logistic regression models. The analysis showed that compared with patients without MHVs, moderate MHVs (adjusted OR=5.446; 95% CI 1.360 to 21.800; p=0.017) and extensive MHVs (adjusted OR 15.240; 95% CI 1.200 to 193.544, p=0.036) were significantly associated with END, while subtle MHVs were not associated with END (p=0.468). The multivariate logistic regression analyses are shown in table 4.
The identification of predictors for END by multivariate logistic regression
Discussion
In the present study, we identified that the presence of MHVs was associated with END in patients with anterior circulation AIS receiving IVT therapy. Both moderate and extensive grades of MHVs were able to predict END (OR 5.446 and OR 15.240, respectively). As SWI is increasingly being applied for patients with AIS, this finding may help physicians to identify those at a relatively high risk of END.
MHVs have been hypothesised to be related to increased deoxyhaemoglobin15 31 because of the reduced oxygen saturation in hypointense vessels.32 An increased oxygen extraction fraction in ischaemic tissue with a large perfusion–diffusion mismatch (PDM) leads to an increased deoxyhaemoglobin–oxyhaemoglobin ratio, which results in more prominent MHVs on SWI.25 According to several previous studies, the presence of MHVs might also reflect poor perfusion within the infarction territory16 18 33 34; poor levels of perfusion have also been correlated with the occurrence of END in AIS patients.11 22 23 Consequently, there appears to be a correlation between the presence of MHVs and END. A larger PDM has been reported to be related to END,11 23 35 and more severe MHVs were associated with larger PDM.25 Therefore, this could explain why moderate and extensive MHVs were related to END while subtle MHVs were not associated with END. This finding indicated that the correlation between the presence of MHVs and END was non-linear, and a threshold might exist when using MHVs to predict END.
The presence of MHVs was highly correlated with prominent ILASO.19 However, in our study, 26 (42.6%) patients had prominent ILASO but lacked MHVs. We hypothesise that this phenomenon is related to the collateral circulation. Indeed, a previous study also reported that the presence of MHVs was related to poor collateral circulation.36 Therefore, the patients in our study who did not have MHVs might have had relatively good collateral circulation.
In our study, we evaluated intracranial arteries by 3D-TOF-MRA, which increased the difficulty of completely distinguishing ILAO from ILAS. Meanwhile, MHVs could present in patients with either ILAS or ILAO, and ILASO was examined as a whole in a previous study.20 Therefore, it would be reasonable to combine ILAS and ILAO into the category of ILASO.
There were several advantages to our study. First, this is one of only a few studies that have focused on the specific relationship between the presence of MHVs and END after IVT. In addition, we used a semiquantitative method of assessment to evaluate the predictive value of MHVs. However, there were also several limitations to our study that need to be considered. First, the sample size was relatively small, and only four patients (6.6%) in our study had extensive MHVs, which may lead to a limitation of the statistical power. Second, because MHVs were only assessed once, it was not possible to examine dynamic changes. Third, CTA or DSA was performed for only a few of our patients, potentially resulting in an overestimation of intracranial stenosis and uncertainty regarding recanalisation of the occluded vessels and the collateral circulation to the infarction. Finally, in our study, the median interval between stroke onset and MRI scanning was 42 hours (range, 13–65 hours), which meant that END may have occurred prior to MRI scanning in some cases. This might partially reduce the clinical application of MHV assessment. However, AIS patients who present with MHVs and without END would be more likely to experience END than those without MHVs. Monitoring the functional status and maintaining a stable level of cerebral perfusion would be a reasonable treatment.
Conclusion
The presence of MHVs might be useful in the prediction of END in AIS patients with symptomatic ILASO after r-tPA treatment.
Acknowledgments
We thank Lisa Kreiner, PhD, from Liwen Bianji, Edanz Editing China (www.liwenbianji.cn/ac), for editing the English text of a draft of this manuscript.
References
Footnotes
Contributors Y-LL: designed and conceptualised the study; analysed the data; data acquisition; drafted the manuscript for intellectual content. Y-KC: designed and conceptualised study; analysed the data; data acquisition; revised the manuscript for intellectual content. H-PY, D-HQ, J-FQ, H-HZ, Z-HL, FW, M-QL: analysed data; data acquisition.
Funding This study was supported by the Medical Scientific Research Foundation of Guangdong Province, China (Reference number: A2018322).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study was approved by the hospital ethics committee (approval number: KYKT2018-002).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.