Article Text

Abstract
Intracerebral haemorrhage (ICH) describes haemorrhage into the brain parenchyma that may result in a decline of the patient’s neurological function. ICH is a common cause of morbidity and mortality worldwide. Aggressive surgical treatment for ICH has remained controversial as clinical trials have failed to demonstrate substantial improvement in patient outcome and mortality. Recently, promising mechanical and pharmacological minimally invasive surgery (MIS) techniques for the treatment of ICH have been described. MIS was designed with the objective of reducing morbidity due to complications of surgical manipulation. Mechanical MIS includes the use of tubular retractors and small diameter instruments for ICH removal. Pharmacological methods consist of catheter placement inside the haematoma cavity for the passive drainage of the haematoma over the course of several days. One of the most favourable approaches for MIS is the use of natural corridors for reaching the lesion, such as the transsulcal parafascicular approach. This approach provides an anatomical dissection of the subjacent white matter tracts, causing the least amount of damage while evacuating the haematoma. A detailed description of the currently known MIS techniques and devices is presented in this review. Special attention is given to the transsulcal parafascicular approach, which has particular benefits to provide a less traumatic MIS with promising overall patient outcome.
- hemorrhage
- technique
- endoscopy
- brain
- device
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Intracerebral haemorrhage (ICH) refers to any bleeding located within the brain parenchyma. Spontaneous, or non-traumatic, ICH has an incidence of ~24.6 per 100 000 person-years and affects 40 000–67 000 people annually in the USA.1 2 This entity leads to significant disability or death, with a 1 month case fatality rate of 40% and 54% per year, with few patients achieving long-term independence.3 Despite advances in technology and multiple clinical trials, a significant change in the prognosis of these patients has not been observed.
Despite its prominence and high mortality, spontaneous ICH lacks a universally recognised and effective treatment.4 5 The heterogeneous nature of this condition and absence of data-driven recommendations has led to widespread variation in its clinical management. This has led to further investigate different surgical approaches. Given the lack of clear benefit from open surgery, increasing interest in minimally invasive techniques for the evacuation of ICH has emerged.4
Minimally invasive surgery (MIS) has become the focus of large-scale studies in recent years. In a meta-analysis of randomised controlled trials (RCTs) evaluating MIS techniques in the treatment of spontaneous ICH, Scaggiante et al found that selected patients with supratentorial ICH benefit from MIS over other treatments, regardless of the specific MIS technique or the evacuation timing.6 Ongoing trials are investigating MIS techniques, including the ENRICH (Early Minimally Invasive Removal of ICH) and Minimally Invasive Endoscopic Surgical Treatment with Apollo/Artemis in Patients with Brain Haemorrhage) (INVEST) trials.7 The preliminary results are promising and could shape how ICH will be managed in the future. The purpose of this review is to examine recent advances in MIS techniques for the evacuation of ICH, focusing on the advantages of minimally invasive parafascicular surgery (MIPS).
Pathophysiology
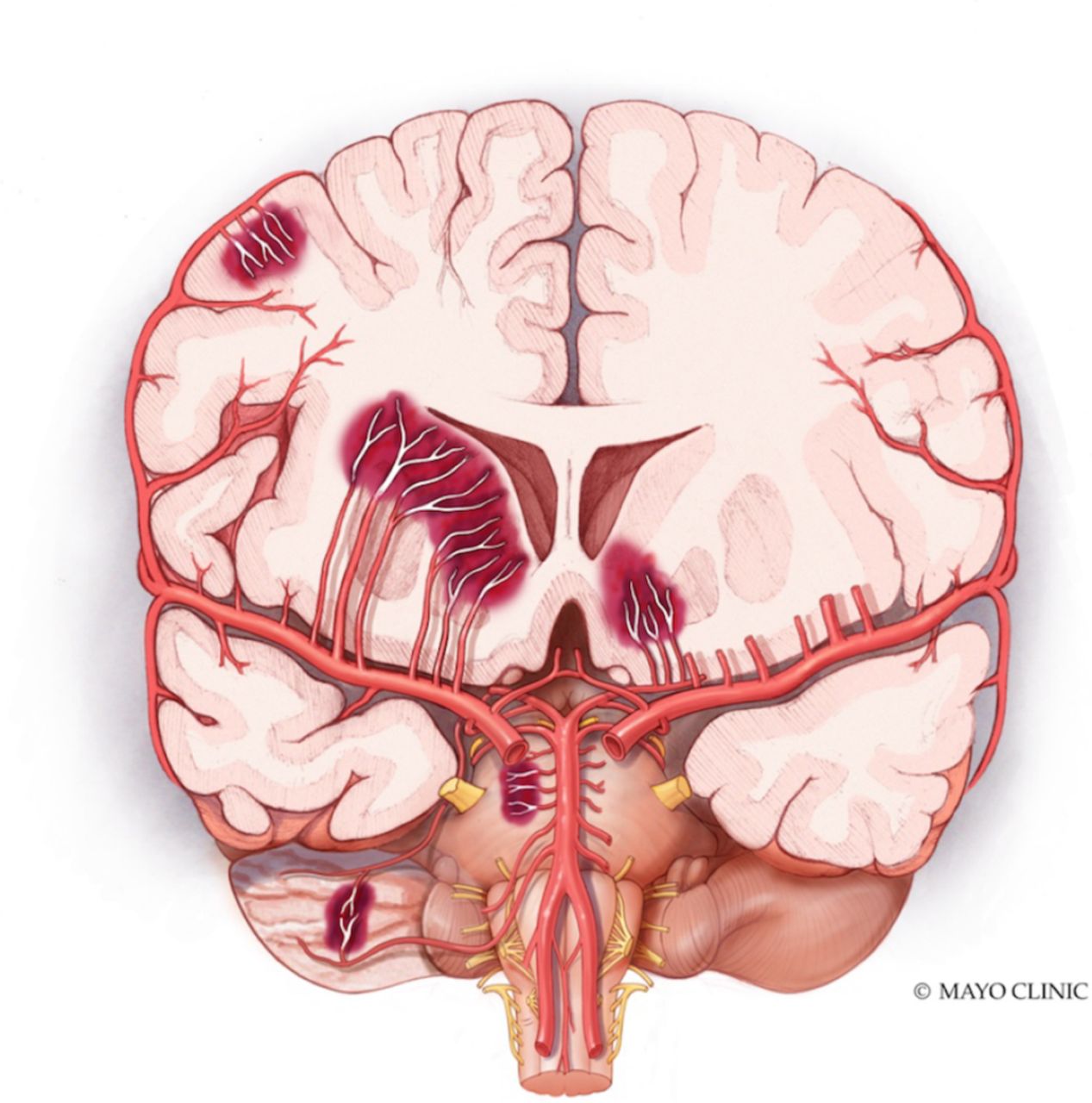
ICH can be divided into two main categories: traumatic and spontaneous.8 Spontaneous ICH is further subdivided into primary or secondary. Primary ICH is a manifestation of small vessel disease, while secondary ICH is due to a variety of pathologies including coagulopathy, vascular malformation, aneurysm rupture, cerebral venous thrombosis, haemorrhagic conversion in stroke or vasculitis.9 Primary ICH accounts for ~78% to 88% of cases of spontaneous ICH, where hypertension and cerebral amyloid angiopathy (CAA) represent the most common underlying causes. In general, the principal risk factor associated with ICH is chronic hypertension, which is identified as a precipitating factor in 80%–90% of patients with ICH. Chronic hypertension affects small to medium perforating arteries, resulting in haemorrhages in basal ganglia, thalamus, brain stem and cerebellum, among others1 10 11(figure 2). CAA is a vasculopathy characterised by the deposition of amyloid in vessels and presents as lobar haemorrhages in elderly individuals (figure 2). Secondary ICH is caused by preformed vascular abnormalities or a systemic disease leading to vascular changes in the central nervous system, such as the ones listed in figure 1.12

Coronal section illustrating the different locations of intracerebral haemorrhage, special attention to lobar and deep-seated haemorrhages. Mayo clinic foundation for medical illustration and Research.
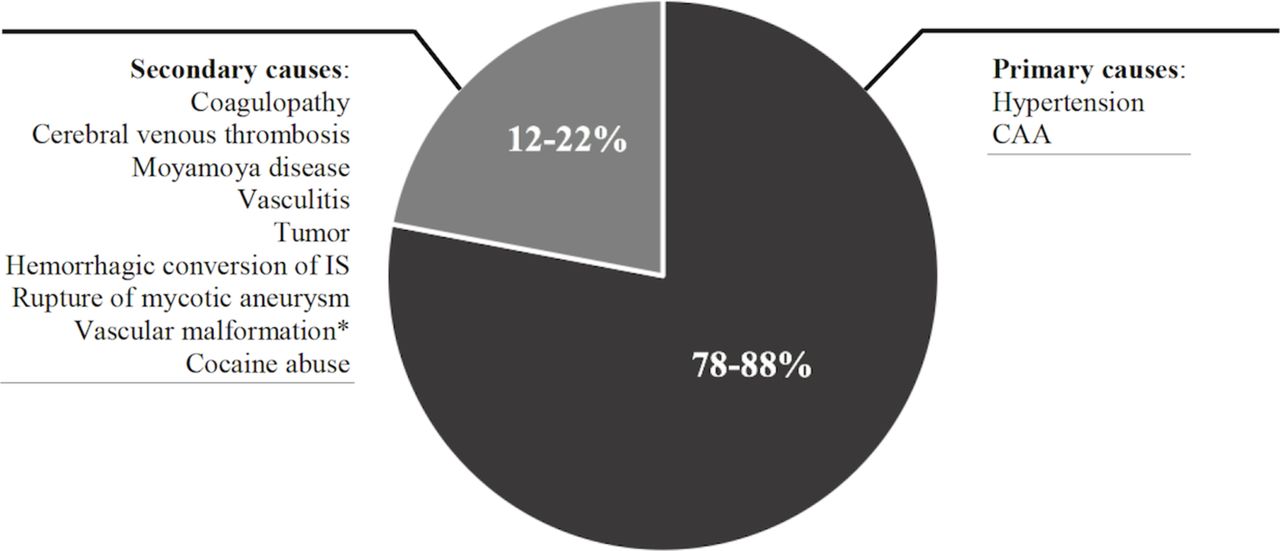
Summary of primary and secondary causes of ICH. *Vascular malformations: arteriovenous malformations, cavernous malformation, fistula. CAA, cerebral amyloid angiopathy; ICH, intracerebral haemorrhage.
Management
ICH is considered a medical emergency and treatment should be individualised to each patient. According to the guidelines by the American Heart Association (AHA) and the American Stroke Association (ASA) published in 2015, the first step in ICH management should be medical stabilisation and close monitoring of the patient.13 It is fundamental to establish a neurological status baseline using the NIH Stroke Scale/Score (NIHSS), Glasgow Coma Scale (GCS) or the Four Score assessment guides in order to have an appropriate baseline severity for further management.14 15
After establishing clinical stability, a neuroimaging study is necessary to integrate an accurate diagnosis and identify the characteristics of the ICH. The ‘gold standard’ imaging study is a non-contrast CT as it immediately provides sufficient information to determine the type of bleeding, location, volume, extension, involved neurological structures and the risk for haematoma expansion.16–18 If the patient is clinically stable, MRI study (gradient echo or T2 sequences) or other vascular imaging modalities such as CT angiography can be used to determine the underlying cause.16 19 Grading scales such as the ICH score and its derivatives, such as the functional outcome (FUNC) score that is based on ICH volume, location and presence of intraventricular haemorrhage (IVH), can be used to prognosticate neurological outcome and mortality.20 21
Early haematoma expansion represents one of the most important modifiable risk factors and, outcome predictor.22 For that reason, the AHA/ASA guidelines recommend strict blood pressure control and correction of any underlying coagulopathy immediately after diagnosis.13 According to results from the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial II (INTERACT II) and Anti-hypertensive Treatment of Acute Cerebral Hemorrhage II (ATACH II) trials, blood pressure has to be lowered gradually, by reaching a systolic blood pressure (SBP) of <140 mm Hg for ICH patients presenting with SBP between 150 and 220 mm Hg.13 23 24 On the other hand, any underlying coagulopathy should be corrected immediately by administering coagulation factors or platelet replacement.13 For oral anticoagulation reversal, administration of antidote has to be carried out immediately and monitored continuously.14 Additional control of seizures, temperature, blood glucose concentration, intracranial pressure and oedema can also help prevent complications.5 13
Indications for surgery
Surgical indications that are supported by class 1 recommendations in patients with ICH are those who are clinically deteriorating, those with cerebellar haemorrhages with brainstem compression, and/or those with haemorrhagic ventricular obstruction leading to hydrocephalus.13 The role of surgery in the management of patients with supratentorial ICH remains controversial.25–30 The rationale supporting surgery is based on the fact that it could reduce the volume of the haemorrhagic lesion, improving cerebral perfusion and avoiding the potential damage to neural tissue.31 32 Evidence suggests that the presence of an ICH could modify the pressure gradient between the tissue surrounding the lesion and distant tissue,33 which could reduce cerebral perfusion and put the viability of this surrounding parenchyma at risk. This potentially viable ischaemic area, or penumbra, has also been related to oedema and the presence of blood-derived cytotoxic metabolites.34–37
Two multicentre clinical trials have studied the role of surgery in ICH. The International Surgical Trial in Intracerebral Haemorrhage (STICH) aimed to compare early surgery versus initial conservative treatment in patients with spontaneous supratentorial ICH.38 This trial failed to show benefit from early surgical intervention, with 26% and 24% of favourable outcomes rates for the surgical and non-surgical arms, respectively; with no difference in mortality rates between groups. On the basis of a subgroup analysis, the authors suggested that patients with ICH within 1 cm of the cortical surface may benefit from surgery (OR: 0.69; 95% CI 0.47 to 1.01) and that surgery could decrease unfavourable outcome rates in comatose patients with a GCS<8. These potential benefits of surgery for lobar ICH led to a second trial with a more homogeneous population of patients, STICH II. This trial was designed to study if early surgery could improve outcomes in conscious patients in whom there is a superficial ICH of 10–100 mL and no evidence of IVH. However, the STICH II trial also failed in finding benefit from early surgical intervention, as 59% and 62% of patients from the surgical and non-surgical groups, respectively, had an adverse outcome.39 Nonetheless, a potential criticism of STICH II was the surgery could be done in any fashion including open craniotomy or minimally invasive. This left the door open to the possibility that advances in surgical techniques incorporating preoperative imaging, MIS and cortical mapping could theoretically lead to better outcomes for haemorrhagic lesions in difficult-to-approach locations.
MIS approaches
MIS for ICH evacuation can be classified into mechanical or stereotactic/pharmacological methods.40 Mechanical methods aim to reduce procedure-related morbidity by decreasing the damage to brain parenchyma caused by surgical manipulation. This category includes the use of endoports or tubular retractors, and small diameter instruments combined with conventional neuroendoscopy. Stereotactic/pharmacological methods involve placement of a catheter in the haematoma cavity and the administration of a thrombolytic agent. In contrast to pharmacological methods, a mechanical approach provides the evacuation of the haemorrhage in a single procedure rather than passive drainage of the haematoma over the course of several days.
Mechanical approaches of MIS
Auer et al were the first to examine the feasibility of ICH endoscopic removal. In a randomised pilot study of 100 patients with spontaneous supratentorial ICH, the authors compared endoscopic evacuation versus conventional medical management. The results showed a significantly lower 6-month mortality rate in the surgical cohort (48% vs 70%, p<0.05). Although there was a favourable increase in survival after surgical intervention, this benefit was limited to patients <60 years old and to subcortical haematomas. This study failed in finding improved functional outcomes in the surgical cohort.25 Since then, several retrospective and prospective randomised studies have compared minimally invasive aspiration to standard craniotomies and suggested benefit from MIS techniques.41 42
A recent meta-analysis conducted by Xia et al analysed 14 high-quality RCTs and prospective studies to compare MIS to craniotomy.43 Data from 2466 patients showed a lower mortality rate in patients undergoing MIS (OR: 0.76; 95% CI 0.60 to 0.97). It was also found that when compared with the medically treated group, the MIS cohort had a statistically significant reduction in rebleeding at the end of follow-up (OR: 0.42; 95% CI 0.19 to 0.95). Similar findings were reported in a subsequent meta-analysis conducted by Tan et al, examining 16 studies consisting of 1912 patients who compared MIS versus craniotomy or conservative treatment in patients with hypertensive ICH, and they reported lowered mortality rates and reduction of rebleeding in the MIS cohort.44
There have been recent surgical advances and techniques for haematoma evacuation—BrainPath/Myriad (NICO, Indianapolis, Indiana, USA) and the Apollo (first generation)/Artemis (second generation) Systems (Penumbra, Alameda, California, USA). The Nico BrainPath is a minimally invasive tubular retractor system which utilises naturally existing corridors to decrease iatrogenic insult and facilitate the drainage of the haemorrhage. The Apollo/Artemis is a non-clogging aspiration/irrigation wand which assists in the removal of haemorrhagic products in conjunction with neuroendoscopy (table 1).
Comparison of different innovative minimally invasive techniques for ICH
Innovative mechanical techniques in MIS
Tubular retractor devices
The BrainPath tubular retractor device was first approved by the United States Food and Drug Administration (FDA) for treatment of ICH in 2016. It consists of a clear sheath and an obturator. These provide circumferential retraction that symmetrically distributes the forces to the surrounding brain parenchyma. They are placed through a small craniotomy with a dural opening large enough to encompass the device (13 mm). The sheath is then advanced under neuronavigation guidance using a transsulcal parafascicular approach into the distal aspect of the clot, along the longest axis of the haematoma. Once the sheath is placed the obturator is removed, and the clot is evacuated with the assistance of exoscopic visualisation with conventional microsurgical techniques. If the clot is too dense then the Myriad handpiece; an automated no-heat device can be used for cutting, suction and blunt dissection to evacuate the clot. In addition, there are other tubular retractors with similar functions including the Vycor Viewsite, which is ovular in shape.45
Given the potential benefits of these minimally invasive technologies, several studies have aimed to assess the death rates, functional outcomes and extent of haematoma evacuation in ICH patients surgically intervened with endoport systems. A retrospective review conducted by Prybylowski et al aimed to assess the risk to benefit profile of patients undergoing ICH evacuation using tubular retractors.41 This retrospective case series demonstrated a median reduction in ICH volume of 87%, with a 36% functional independence at 90 days and 36% of procedure-related mortality.
Bauer et al conducted an initial case series looking at the feasibility of tubular retractors in the evacuation of ICH. The authors analysed data from 18 patients with spontaneous deep-seated and lobar haemorrhages evacuated using the BrainPath.42 Outcome measures included 30-day mortality, mean baseline modified Ranking score, GSC and ICH score. Data showed a significant decrease in mean volume reduction of 95.7% (±5.8%; p<0.001) after the intervention, with no reports of complications during follow-up and a low 30-day mortality rate (5.6%) within the cohort. Regarding neurological outcomes, they reported an increase in the mean GCS of 5±2.3 but no improvement on the median NIHSS scale postoperatively.
A larger multicentric study looking at the outcomes of patients who had undergone tubular retractor-assisted evacuation of ICH was recently performed by Labib et al. Here, investigators examined a total of 39 patients with symptomatic, supratentorial ICH with minimal or no intraventricular bleeding.46 These patients had a median ICH volume of 36 mL (IQR, 27–65 mL) with a median depth of 1.4 cm (IQR, 0.3-2.9) from the cortical surface. All the included patients underwent evacuation using the BrainPath through a minimally invasive, transsulcal parafasicular approach. After the surgery, the majority of patients (72%) achieved a clot reduction between 50% and 89% of preoperative haemorrhage volume and developed a statistically significant improvement of the median GCS, with a median postoperative GCS of 14 (range: 8–15; IQR, 11–15). At follow-up (30–365 days), there was a 0% mortality rate and 52% of patients achieved an MRS score ≤2 indicating a relatively high achievement of functional independence.
Apollo/Artemis system
The Penumbra Apollo and Artemis Systems were first approved by the FDA in 2014.43 This device consists of a non-clogging aspiration and irrigation wand that houses a vibrational element to eliminate clot buildup. This system fits through the channels of commercially available endoscopes, allowing drainage under continuous endoscopic visualisation. The haematoma is accessed through a burr whole or a minicraniotomy, with a small dural incision that is only sufficiently large to accommodate the endoscope sheath. Under navigation guidance, the sheath is advanced along the longest axis of the haematoma. Once the endoscope sheath reaches the distal portion of the haematoma, the inner obturator is removed and the neuroendoscope is inserted with the Apollo/Artemis device inside its working channels.
Fiorella et al conducted a case series of three patients undergoing evacuation with the device,47 where they reported a significant reduction in the volume of the intraparenchymal haemorrhage from 93.4 to 11.2 mL and from 15.6 to 0.9 mL for the first and second patient, respectively, and a complete evacuation of the parenchymal component in the third patient which had a mixed intraparenchymal/IVH. Tan et al reported their early single centre experience using the Apollo device, where a total of eight patients were examined and investigators found a significant reduction in volume after its implementation and resulted in a decrease in mean Graeb Score (GS) and median mGS.48
Goyal et al looked at a larger series of 224 patients and compared a subset of patients who were matched for confounding variables, where 18 patients who were evacuated with the Apollo device were compared with 54 patients undergoing standard medical treatment.49 These investigators matched the arms using median ICH volume, median ICH score and median admission ICH score. They found that median residual ICH volume was lower in the interventional group versus the medically treated group (15 vs 40 cm3; p<0.001). There was a significant reduction in the in-hospital mortality for patients who underwent surgical intervention versus medically treated patients (28% vs 56%; p=0.041); however, the data failed to show reduced morbidity or any differences in other prespecified outcome measures. One of the main limitations is that these outcomes were assessed after a short time period of 3 months, instead of waiting until the 6-month or 12-month mark for assessments.
Spiotta et al conducted a multicentric analysis of the 29 patients who underwent ICH evacuation with the Apollo system, where 6 had intraventricular extension.50 After the evacuation procedure, they reported a mean decrease in haemorrhage volume of 54.1%±39.1% reduction p<0.001. Although they reported a low mortality rate of 13.8%, only 2 patients were discharged home, with the remaining 12 patients in an acute rehabilitation centre and 2 patients in long-term care facilities. There were no differences in mortality in patients with lobar versus basal ganglia haemorrhages.
In an effort to optimise haemostasis and evacuation efficiency of ICH, Kellner et al described the Stereotactic Intracerebral Haemorrhage Underwater Blood Aspiration technique (SCUBA).51 The authors combined conventional methods for evacuating ICH with a wet field strategy. This process is divided into two phases. Phase I includes evacuation of the ICH with neuroendoscopic guidance using the Apollo device, and phase II involves the SCUBA technique where the cavity is infused with saline permitting fluid filled exploration. This allows for the assessment of active bleeding which are addressed by continuous irrigation, pressure using the endoscope, or cauterisation using an endoscopic bipolar electrode. The authors evaluated a series of 47 patients who underwent haematoma evacuation via the SCUBA technique. Using this technique, investigators observed a significant decrease in mean ICH volume from a mean preoperative ICH volume of 42.66 cm3 (SD: 29.7 cm3) to a mean postoperative ICH volume of 4.2 cm3 (SD: 6.6 cm3), resulting in an average evacuation of 88.2% of the initial volume (SD: 20.8%). Postoperative outcome measures such as morbidity or mortality were not assessed.
A direct comparison between patients treated with the Apollo system and BrainPath was conducted by Griessennaure et al. 52 This small size, retrospective matched cohort of five cases per group showed no overall differences in volume evacuation between the two methods but did reveal poor functional outcomes and increased mortality in both. However, these findings are subjected to bias due to its retrospective nature and reduced sample size, as well as delayed time to intervention (median: 2 (1–4) days). More robust studies are in need to come to an accurate conclusion.
Minimally invasive parafascicular approach
Depending on haemorrhage location and surgeon’s preference there are two approaches for open ICH drainage: trans-sulcal or trans-gyral. A trans-gyral approach provides direct access to the lesion and can be considered in the setting of a subcortical ICH located in non-eloquent regions. In the case of deep-seated haemorrhage underneath eloquent cortex, the trans-sulcal approach offers a substantial advantage. A trans-sulcal route minimises transgressed cortex, engages subcortical U-fibres, and can be applied to eloquent cortical and white matter tracts, while trans-gyral approaches can be technically easier and avoid sulcal arteries and veins. Minimally invasive subcortical parafascicular transsulcal access for clot evacuation (Mi SPACE) is an innovative technique that uses existing anatomical corridors to cause the least amount of damage to the subjacent white matter tracts.46 53 This technique is performed with the assistance of tubular retractors that are introduced assisted by neuronavigation systems, designed to preserve the integrity of implicated cortex and fibre tracts by moving parallel with white matter tracts.54
Preoperative imaging and planning are crucial steps in order to minimise potential damage to eloquent cortical and subcortical tracts. In addition to standard imaging techniques including a non-contrast CT and a CT-angiography, some authors mention the use of diffusion tensor imaging (DTI) with tractography as complementary imaging, however; due to the urgency of ICH and to distortion of the imaging due to clot, it is rarely performed.
All cases are performed under general anaesthesia. The position of the patient will be determined during the presurgical planning, and this can be supine, lateral or park bench. The accuracy of the navigation system is crucial to the surgery. When accessing the haematoma, the surgeon must ensure that the sagittal, coronal and axial planes are on target. Once this is performed, the entry point is marked on the scalp and confirmed by the navigation tool. The sulcus overlying the lesion and one that engages the least number of critical white matter tracts is typically chosen. A small incision of ~1.5–2 inches in length is made on the scalp, and the scalp is retracted with blunt scalp hooks or fixed skin retractors. For this approach, a small craniotomy of 2–3 cm in diameter is performed. The dura is then opened in a cruciate fashion to a diameter slightly larger to that of the tubular retractor (13 mm). Ultrasound can be used as a tool to verify the location of the haematoma. The dural flaps are tacked up with suture, and the sulcus that will serve as the point of entry is identified through the image guidance probe. The arachnoid covering the sulcus is incised as widely as possible under exoscopic or microscopic visualisation. The tubular retractor is then inserted into the sulcus and advanced to the preplanned depth under image guidance. The lesion is typically entered two-thirds to its depth. Evacuation is performed with the aid of exoscopic visualisation. The clot is removed through a combination of aspiration and bipolar cautery. If the clot is too dense, a side-cutting tissue device (Nico Myriad) can be used for cutting, suction and blunt dissection. The cavity is searched for potential sources of active bleeding. If arterial bleeds are found, they are coagulated with bipolar cautery, venous bleeding can be managed by placement of haemostatic materials such as Gelfoam or surgicel with gentle pressure. Once haemostasis is achieved, the sheath is carefully withdrawn in small increments. A small piece of Gelfoam is placed over the brain and the dura is sutured. The bone flap is placed and secured into place, the scalp is closed and a dressing is applied. The patient is typically extubated, and a postoperative head CT is done.
Advantages of mechanical clot evacuation are immediate clot removal, address site of bleeding, reduce mass effect and potentially decrease hospital stay. The following cases illustrate the technique, complementary DTI is provided for educational purposes to depict relevant anatomy in relation to the approach (figure 2).
Illustrative cases
Patient 1
An elderly patient with a history of hypertension presented to the emergency department after being found unresponsive. On physical examination, the patient was aphasic and not following commands had left gaze deviation, right facial droop and right haemiparesis with spasticity, and a NIHSS score of 26 and a GCS of 10. A non-contrast CT showed an acute ICH located to the left basal ganglia and temporal lobe (figure 3). A diagnostic cerebral angiogram did not show any abnormalities. Surgical treatment was performed in an effort to relieve the mass effect. The patient underwent MIS with the BrainPath retractor using a transsulcal parafascicular approach accessing the haematoma through an anterior approach medial to superior longitudinal and arcuate fasciculi. Visualisation was assisted with the use of an exoscope. A postoperative CT was performed which showed complete clot evacuation and expected postsurgical changes. Extubation occurred after the surgery and was transferred to the intensive care unit with a 3-day stay, transfer to the floor and discharge on day 7 to rehabilitation with some neurological deficits including aphasia and right-sided weakness unchanged from preoperatively. Four months post-op, the patient has shown significant improvement, with a GCS of 15, improved speech with some minor paraphasic errors and subtle right-sided weakness in the right upper extremity (4/5).
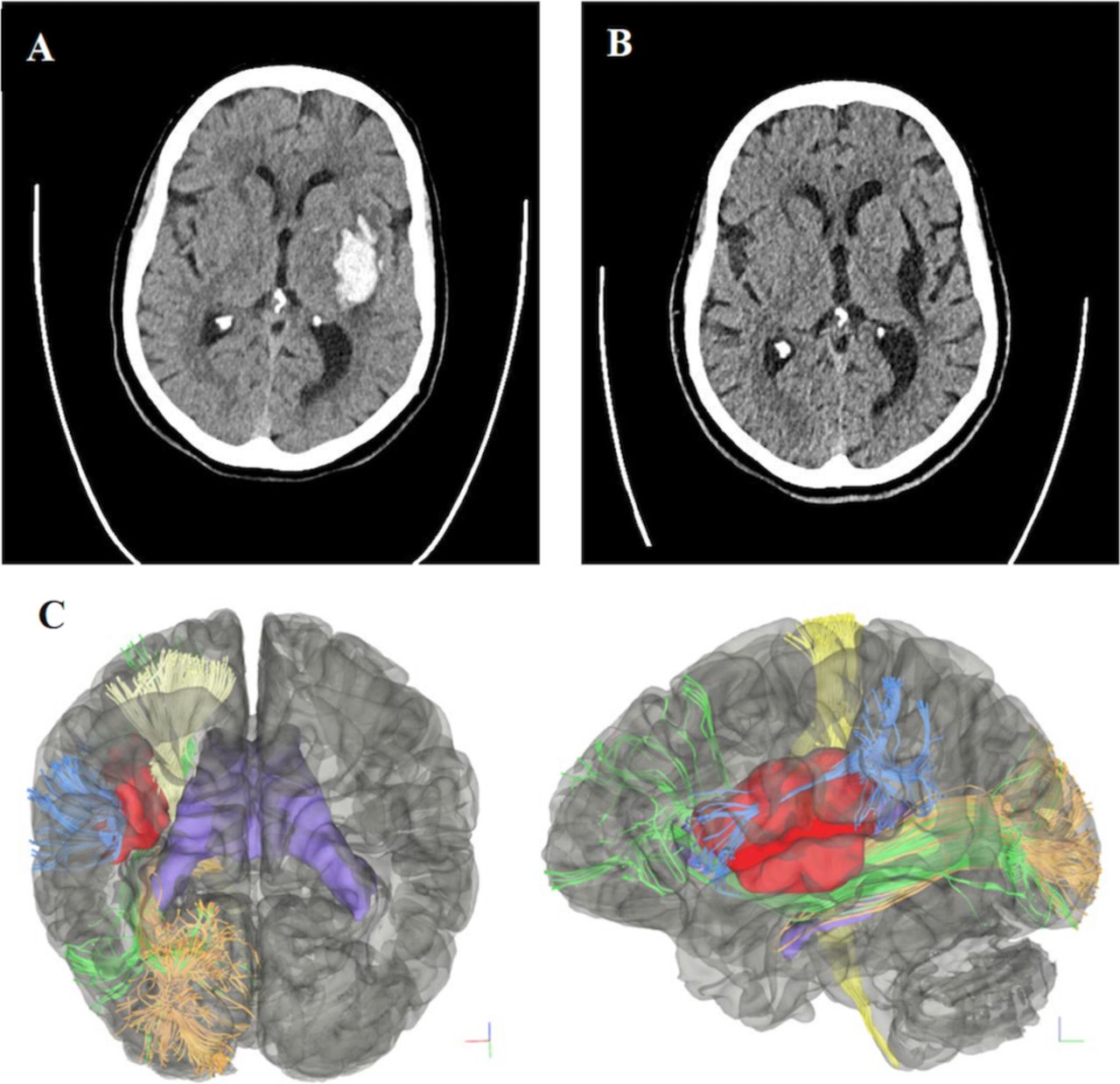
Patient 1. ICH in the left basal ganglia and left temporal lobe. (A) Preoperative non-contrast CT showing left-sided intraparenchymal haemorrhage within the insular region without midline shift. (B) Non-contrast CT 3 months post-op showing a stable residual cystic cavity from haematoma evacuation. (C) Coronal (left) and sagittal (right) DTI-generated preoperative simulated 3D tractography of patient 1. The location of the clot (red) is shown relative to the corticospinal tract (light yellow), inferior fronto-occipital fasciculus (green), optic radiations (orange) and lateral portion of the superior longitudinal fasciculus (SLF 3) (sky blue). Lateral ventricles (purple) are showed as reference. DTI, diffusion tensor imaging; ICH, intracerebral haemorrhage.
Patient 2
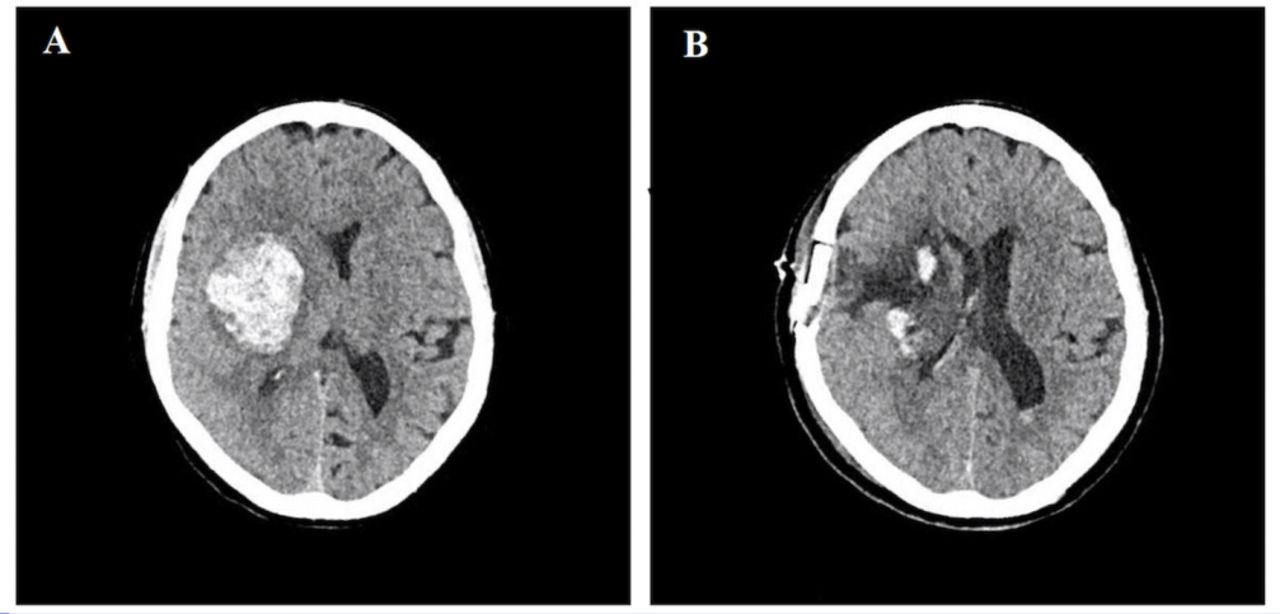
An elderly patient was brought to the emergency department after being found unresponsive. The patient presented in a state of coma and acute respiratory failure, with a blood pressure of 174/136 mm Hg and a GCS of 8. A non-contrast CT performed showed a large acute right basal ganglia haemorrhage with midline shift and uncal herniation which occurred secondary to a hypertensive crisis (figure 4 ). The haemorrhage was evacuated using the BrainPath retractor under navigation guidance and exoscopic visualisation. The patient was extubated after surgery, head CT showed 95% clot evacuation, and was transferred to the ICU. The patient stayed in the ICU for 2 days and was discharged to rehabilitation on postoperative day seven with a GCS 15, left-sided weakness (3/5) and intact speech.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient 2, with right basal ganglia deep brain parenchymal haematoma. (A) Initial non-contrast head CT showing a right haemispheric parenchymal haematoma centred in the basal ganglia with extension into the frontal lobe/insular region and effacement of the right lateral ventricle. (B) Postoperative CT without contrast on day 2 after haematoma evacuation showing good clot evacuation without rebleeding.
Catheter-based pharmacological MIS
The use of thrombolytics as an adjunct therapy to MIS was investigated by Wang et al in a randomised clinical trial involving 377 patients, where 182 patients were allocated to conservative management and 195 to CT-guided craniopuncture with aspiration followed by the administration of a urokinase solution over 3–5 days.55 Data revealed a trend towards favourable functional outcomes and decreased dependence in the interventional group at 90-day follow-up (40.9% vs 64%; p<0.01). However, there was no statistically significant difference in 90-day mortality rates between cohorts. A similar RCT conducted by Sun et al compared craniopuncture plus urokinase infusion against craniotomy in 304 patients with deep-seated haemorrhages.56 In spite of finding increased favourable outcomes in the craniopuncture and urokinase group, there were no statistically significant differences on neurological function, activities of daily living or mortality rates between groups on follow-up.
The minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE) trial was a multicentric, open-label, phase II RCT evaluating the safety and efficacy of alteplase combined with MIS for treatment of supratentorial, spontaneous ICH. Authors analysed a total of 96 patients randomised to either the best standard of care or MIS plus alteplase.57 A statistically significant reduction of ICH volume was observed in the alteplase group when compared with the medically managed cohort (57% vs 5% reduction; p<0.0001). Investigators assessed for safety and observed no difference in 7-day to 30-day mortality between the two cohorts but did note an increased risk of asymptomatic haemorrhages at 72 hours after the procedure. Its successor, the MISTIE III trial, a multicentric phase III RCT mainly set out to analyse the impact that this technique had on morbidity and mortality. Here, a larger cohort of 506 subjects with spontaneous ICH underwent randomisation into the previously mentioned groups.58 The individuals included for analysis presented with a median ICH volume of 21.8 mL, median GCS score of 10 and NIHSS score of 19. A more in-depth analysis of the data showed the extent of the evacuation of the clot was directly linked to improved functional outcomes; when the technical goal of a residual haemorrhage volume of <15 mL was reached, a significant increase in favourable functional outcomes was observed. After a 365-day period, subjects who had undergone alteplase+MIS showed a decreased estimated all-cause mortality, with a difference of 6%–8% between groups (p≤0.037). However, for patients with moderate to large supratentorial spontaneous ICH (median clot volume of 41.8 mL; IQR: 30.8–54.5), MIS+thrombolysis failed to increase the percentage of improved functional outcomes after a 1 year period. Therefore, the MISTIE III trial concluded that it could not be recommended as an intervention to improve functional outcome until the desired reduction in haematoma size was uniformly achieved.
In the setting of IVH, the Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage III (CLEAR III) trial demonstrated the safety and effacy of intrathecal tissue plasminogen activator (tPA) .59 Here, the authors randomised participants with ICH (≤30 cm3) with associated IVH into receiving placebo intrathecal recombinant tPA (r-tPA) (1 mg) every 8 hours through an external ventricular drain (EVD). Authors found a significant reduction in mortality at 180 days in the tPA group and in a subgroup analysis, patients with IVH volumes >20 cm3 presented better functional outcomes (mRS score 0–3).
Discussion
ICH is a debilitating disease, with only 20% of survivors expected to have full functional recovery after 6 months.1 After the inciting event, the haemorrhage continues to elicit damage to the surrounding brain parenchyma by the activation of the coagulation cascade and haemoglobin breakdown.34 60 Considering this, surgery results as an appealing approach to reduce secondary clot burden and diminish poor outcomes. In spite of the theoretical advantage, evidence from the STICH I and STICH II trials have failed to show clinical benefit to an open surgical approach. These results could potentially be attributed to iatrogenic injury from the surgical manipulation.
New MIS techniques tried to improve the setbacks of conventional surgery by developing safer and more cost-effective methods for haematoma evacuation. Although the MISTIE II trials first proved the technical safety and feasibility of a minimally invasive catheter-based pharmacological therapy of ICH,57 its successor, MISTIE III study failed to show improvement of functional outcome compared with the medically treated arm.58 In contrast to catheter-based thrombolytic therapy, mechanical methods offer the drainage of the haemorrhage in a single procedure and prove a safe and effective way of reducing clot volume and mortality.40 61 Although tubular retractors have been used for decades,62 the recent development of circular retractors has facilitated a transsulcal access, providing a method to safely access the haematoma through naturally existing corridors; minimising the risk of surgical related damage to cortical and subcortical structures. The Mi SPACE approach integrates five core elements: (1) mapping, (2. Navigation, 3 Atraumatic access 4. Optics, and 5. Atraumatic Resection; this allowed improved visualisation and a bimanual technique to facilitate a more complete evacuation than previous MIS designs.46 Preoperative mapping allows the precise identification of the least traumatic trajectory while the tubular retractors used are specifically designed to minimise strain forces on the brain parenchyma. Paired with the use of Video Telescopic Assisted Microscopy, the optimised visualisation provides the benefit of increased haematoma volume drainage which has been reported to be associated with greater functional outcome.46 58
Although many studies show a significant improvement in overall mortality, the benefit of this technique on functional outcomes is not clear. However, these results are limited to small multicentre series, and large series or RCTs are required to draw a more informed conclusion (table 1). Currently, three ongoing trials, the Early Minimally invasive Removal of Intracerebral Haemorrhage trial (ENRICH trial), the INVEST trial (table 1) and the MIND trial aim to answer these questions. INVEST is a single arm feasibility study comparing evacuation with the Apollo system and medical management in moderate to large supratentorial spontaneous haemorrhages (30–80 cm3), which is expected to be completed in 2021. The ENRICH trial is a phase II multicentric RCT comparing the use of early haematoma evacuation using MIPS with a predicted completion rate for 2019. The MIND trial is a larger, multicentre RCT of 500 participants evaluating minimally invasive haematoma evacuation with the Artemis neuroevacuation device. These studies will provide valuable data on the potential benefit of mechanical MIS on improving neurological outcomes.
References
Footnotes
Twitter @EMiddlebrooksMD
Contributors Lina Marenco-Hillembrand: Played a role in manuscript preparation, manuscript revision, figure edits, critical evaluation. Paola Suarez-Meade, Henry Ruiz Garcia, Ricardo Murguia-Fuentes, Erik. H Middlebrooks, Lindsey Kangas: a role in manuscript preparation, manuscript revision, literature search, figure preparation. Kaisorn L. Chaichana and W.David Freeman: played a role in manuscript preparation, final approval, supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.