Article Text

Statistics from Altmetric.com
Background
The advent of flow diverters (FDs) has changed the scope of endovascular treatment options for intracranial aneurysms (IAs). FDs can effectively treat complex aneurysms in which both microsurgical and conventional endovascular options are less than ideal.1 2 The Pipeline Flex Embolization Device (PED; Medtronic, Irvine, California, USA) has been available in the USA for several years demonstrating positive results. More recently, the PED Flex with enhanced delivery features has been introduced, and although decreased, thromboembolic complications are still a potential risk.3 In light of this, a new surface modification was applied to the PED Flex known as Shield Technology consisting of a phosphorylcholine layer covalently bound to its metal braids potentially reducing its thrombogenicity.4 Herein, we report our initial experience using the PED Flex with Shield Technology in the treatment of an unruptured fusiform aneurysm located in the middle cerebral artery (MCA) using dual-antiplatelet therapy.
Case presentation
A 32-year-old woman with history of sudden onset of headache and no other major relevant medical history presented for medical evaluation. Initial head CT and MRI showed no evidence of any haemorrhage, but MRI depicted a possible left MCA aneurysm. A CT angiography (CTA) revealed an unruptured fusiform aneurysm involving the inferior division of the left MCA. Treatment options consisting of observation, clip-wrapping, bypass or possible off-label use of PED were discussed with the patient. Decision was made to perform a cerebral angiogram and a three-dimensional reconstruction, with final therapeutic decision to be made based on bifurcation involvement. If both the superior and inferior divisions were involved, the treatment plan would consist of clip-wrapping but, if only the inferior division was diseased, then the plan was to use the PED. Cerebral angiogram demonstrated the complex morphology of the lesion exclusively compromising the inferior division of the MCA with two components measuring 3.9 mm × 3.0 mm and 3.7 mm × 3.3 mm (figure 1A–C). Due to the complex morphology and location, the final decision was to proceed with endovascular vessel reconstruction using the PED. In order to potentially reduce the risk of thromboembolic events and risk of thrombosis of small-size distal MCA, the use of PED Flex with Shield Technology was petitioned and approved as compassionate use by the Food and Drug Administration and our institutional review board.
{kind=link}
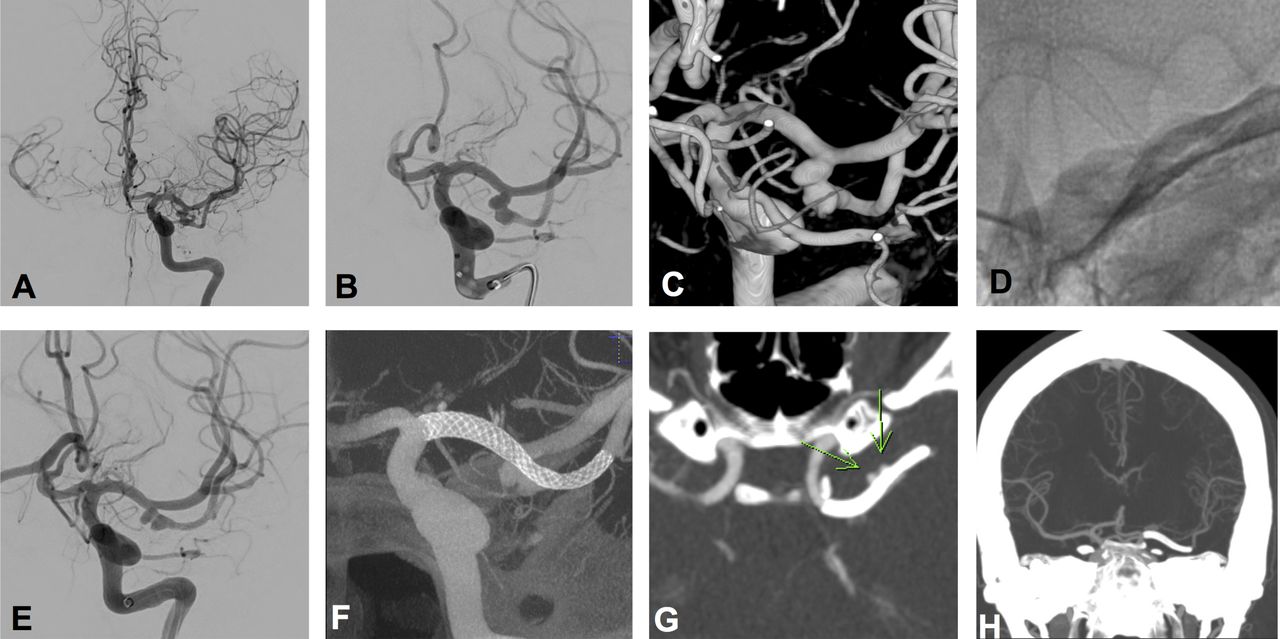
Diagnostic digital subtraction angiography demonstrating a fusiform irregular aneurysm on the inferior division of the left middle cerebral artery (MCA) in anteroposterior (A and B) views. (C) Three-dimensional reconstruction of the aneurysm depicting the complex morphology. The proximal diameter of the parent vessel was 2.6 mm, whereas the distal landing diameter was 1.7 mm. (D) Left MCA, anteroposterior view without contrast revealing the Pipeline Flex Embolization Device with Shield Technology (PED Shield) already deployed. (E) Anteroposterior view with PED Shield already deployed demonstrating patency of the left MCA. (F) Left MCA immediately after implantation of PED Shield, cone-beam CT demonstrating complete coverage of the aneurysm, good wall apposition and no vessel occlusion or stenosis. (G) Postoperative CT angiography (CTA) revealing good positioning of the PED Shield covering the aneurysm and no vessel occlusion or stenosis. (H) The 3-month follow-up CTA demonstrated complete aneurysm occlusion with patent M1 and M2 branches and a slight decrease in the vessel calibre of the superior MCA branch. The patient was neurologically intact at the 3-month follow-up.
Treatment
The final decision between treatment options, clipping-wrapping versus PED, was done after cerebral angiogram with treatment at the same sitting, and for that reason, the patient received a bolus of intravenous integrilin (half of cardiac dose) and was maintained on drip. A femoral approach was performed and a 6-French guide catheter was used to provide stability for deployment of the device, which was delivered through a standard 0.027-inch microcatheter. The proximal diameter of the parent vessel was 2.6 mm, whereas the distal landing diameter was 1.7 mm. The PED Flex with Shield Technology (3 mm × 16 mm) was uneventfully deployed crossing the affected segment from distal portion of the inferior branch of the left MCA to the M1 segment (figure 1D,E). Final angiographic runs and a cone-beam CT angiogram demonstrated good coverage of the aneurysm, good wall apposition and no vessel stenosis or occlusion (figure 1F,G). Following the procedure, the patient was given aspirin (81 mg/day) and ticagrelor (180 mg oral bolus followed by 90 mg two times daily) with intravenous integrilin discontinued 2 hours after ticagrelor bolus.
Outcome and follow-up
The patient’s hospitalisation was uneventful and she was discharged on postoperative day 2. On the day 5 postprocedure, the patient was tested for P2Y12 function resulting in 8 P2Y12 Reaction Units (PRU); therefore, the ticagrelor dosage was decreased in half (45 mg two times daily), whereas aspirin remained in standard dosage (81 mg/day). At the 3-month follow-up, the patient was neurologically intact with a Modified Rankin Scale of 0. CTA revealed no signs of any residual aneurysm with good patency of left MCA and branches (figure 1H).
Discussion
Our case represents the successful placement of the PED Flex with Shield Technology in the treatment of an unruptured MCA fusiform aneurysm. To our knowledge, this represents the first US case of PED Flex with Shield technology for unruptured IAs with the usual dual-antiplatelet therapy.
The rate of ischaemic complications using FDs without the phosphorylcholine layer in the MCA has been estimated in up to 16.3% (95% CI 10.1 to 22.6) regardless of size or morphology.5 In small case series, the rate has been reported as high as 43%.6 Despite the lack of a randomised clinical trial comparing 1:1 the PED Shield versus the PED Flex and the fact that results from in vitro and in vivo models cannot be fully extrapolated to human clinical use, the following benefits of this new technology have been demonstrated:
The PED Shield is less thrombogenic in vitro (lower peak thrombin and takes longer time to achieve peak thrombin; p<0.05) compared with the PED Flex and other FDs.7
The PED Shield had a lower platelet deposition in a non-human primate model compared with the PED Flex in the absence of antiplatelet therapy (p=0.016) and when using dual-antiplatelet therapy (p<0.001). In this study, there was no difference in platelet deposition when using aspirin monotherapy (p=0.084) between the PED Shield and PED Flex.8
The PED Shield has a trend of a faster neointimal development (earlier healing response) but similar percentage at 21 days in pig models based on optical coherence tomography (OCT) and histopathological findings compared with the PED Flex. The PED Shield had a concentric and homogenous neointimal pattern of growth. In addition, in pigs under aspirin monotherapy there were 6/6 PED Flex and 2/6 PED Shield thrombosed devices.9
The frequency of clots forming after angioplasty in rabbit models was lower in the PED Shield compared with the PED Classic based on OCT (p<0.0001). The reduction of microthrombi was also significant along the surface of the PED Shield covering the ostial of side branch arteries (OR 0.18; 95% CI 0.044 to 0.734); p=0.016). These findings did not change as a function of dual-antiplatelet therapy.4
The PED Shield induces less neointimal hyperplasia in rabbit models at 30 days compared with the PED Classic (5.7% vs 8.9%; p<0.0001) based on OCT and histopathological findings (r2=0.83; p<0.0001).10 The superior MCA branch in our patient was jailed and despite concerns for vessel occlusion, previous in vivo studies have demonstrated branches to remain patent despite a high surface tissue coverage11; therefore, treating the patient with PED Shield suggests an added benefit in this patient’s case.
The PED Shield is a new technology and the appropriate antiplatelet regimen remains uncertain. In the first case reported using the device, authors only used aspirin and a single intravenous loading dose of abciximab in a patient with a ruptured aneurysm in the posterior circulation.12 At the 7-week clinical follow-up, the patient was in rehabilitation and the construct remained patent. Recently, the preliminary results of the Pipeline Flex Embolization Device with Shield Technology (PFLEX) study in Europe demonstrated promising periprocedural outcomes.13 This study included 50 patients with IAs located in the internal carotid artery or in the intradural segment of the vertebral artery. The majority of devices (98.1%, 53/54) were successfully deployed in the target site, and there were no neurological complications within the 30-day postprocedure period. Although the majority of patients (88%, 44/50) were placed on single-antiplatelet or dual-antiplatelet therapy before the intervention, platelet reactivity testing was not mandatory and it was only performed in approximately half of them. In addition, there was no standardised regimen for antiplatelet therapy and several combinations of medications were used at the discretion of the neurointerventionalists. The fact that there were no periprocedural ischaemic complications, despite the variety of antiplatelet therapies or hyporesponse to aspirin or clopidogrel, suggests a reduced risk of thrombogenicity using the PED Flex with Shield Technology compared with previous generations of the device. Due to lack of strong data with this new technology, at present, dual-antiplatelet therapy should be recommended when using the PED Flex with Shield Technology. At the 1-year follow-up of the PFLEX study, no major neurological events occurred and the complete aneurysm occlusion rate was achieved in 83.9% of lesions.14 Attempts of PED Flex with Shield Technology using aspirin as monotherapy for ruptured lesions had less than ideal results.15
Our manuscript is limited by a single case study and results cannot be generalised to other centres. The safety and efficacy of the PED Flex with Shield Technology have been demonstrated in the PFLEX study for select cases, but further studies are required to determine the ideal antiplatelet regimen with this technology.
Conclusions
Fusiform aneurysms in the anterior circulation are rarely seen and remain difficult to treat by microsurgery. The introduction of FDs has expanded the treatment possibilities for these lesions and the increased experience with their use have made them a valid alternative. The PED Flex with Shield Technology is a promising alternative with a reduced thrombogenic profile.
Acknowledgments
RS is sponsored by the Interline Endowment Grant.
References
Footnotes
Contributors GJA and PA-S were responsible for study concept and design. GJA and RS contributed to acquisition of the data. All the authors were responsible for analysis and interpretation of the data. GJA, PA-S and RS contributed to drafting of the manuscript. ES and RAH contributed to critical revision of the manuscript for important intellectual content. All the authors were responsible for administrative, technical and material support. ES and RAH contributed to study supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Ricardo A. Hanel is a consultant for Medtronic, Stryker, Codman, and MicroVention. The remaining authors have nothing to disclose.
Patient consent Obtained.
Ethics approval Institutional Review Board of Baptist Health at Baptist Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.