Article Text

Abstract
Background Intracerebral haemorrhage (ICH) is the most devastating form of stroke causing high morbidity and mortality. We aimed to develop a novel clinical score incorporating multisystem markers to predict functional dependence at 90 days after ICH.
Methods We analysed data from Chinese Cerebral Hemorrhage: Mechanism and Intervention study. Multivariable logistic regression analysis was used to identify the factors associated with 90-day functional dependency (the modified Rankin Scale ≥3) after ICH and develop the ADVISING scoring system. To test the scoring system, a total of 2111 patients from Hubei province were included as the training cohort, and 733 patients from other three provinces in China were included as an external validation cohort.
Results We found nine variables to be significantly associated with functional dependency and included in the ADVISING score system: age, deep location of haematoma, volume of haematoma, National Institutes of Health Stroke Scale, aspartate transaminase, international normalised ratio, neutrophil-lymphocyte ratio, fasting blood glucose and glomerular filtration rate. Individuals were divided into 12 different categories by using these nine potential predictors. The proportion of patients who were functionally dependent increased with higher ADVISING scores, which showed good discrimination and calibration in both the training cohort (C-statistic, 0.866; p value of Hosmer-Lemeshow test, 0.195) and validation cohort (C-statistic, 0.884; p value of Hosmer-Lemeshow test, 0.853). The ADVISING score also showed better discriminative performance compared with the other five existing ICH scores (p<0.001).
Conclusions ADVISING score is a reliable tool to predict functional dependency at 90 days after ICH.
- Cerebrovascular Disorders
- Stroke
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Intracerebral haemorrhage (ICH) is the second most common stroke subtype and accounts for 15%–30% of stroke cases worldwide. ICH is associated with 50% of stroke-related mortality (approximately 2.8 million deaths per year) and is twice as fatal as ischaemic stroke.1–3 Many ICH scoring systems have been developed to predict the patient’s outcome. These scoring systems assess the prognosis of ICH at different stages. For in-hospital or 30 days after ICH, there are ICH score4 and simplified ICH score.5 For intermediate-term predictive models (3 months after ICH), there are ICH Grading Scale (ICH-GS),6 ICH Outcomes Project (ICHOP) score,7 the functional outcome (FUNC) score8 and Essen-ICH score.9 For long-term outcome (6 months or 1 year after ICH), there are modified ICH (MICH) score,10 max ICH score11 and ICH Functional Outcome Score (ICH-FOS).12 Efforts were made to improve the model discrimination and calibration, and predictors of models were optimised by adding single or several laboratory indicators to the clinical characteristics.
Limitations of prior studies include small sample size from single centre or not sufficiently validated, using Glasgow Outcome Score or Barthel Index but not modified Rankin Scale (mRS) to measure outcome. Most scoring systems include only indicators of adverse effects of haematoma, but not the indicators of multiple system injuries and responses after ICH, including organs such as liver13 and kidney,14 inflammation,15 coagulation16 and metabolic disorders,17 which may worsen the prognosis in patients with ICH. Thus, integration of important clinical predictors of ICH reflecting multisystem responses into the prognostic model may improve the assessment of poor outcomes after ICH (online supplemental file 2, graphical abstract).
Supplemental material
In this study, we aimed to develop a novel tool incorporating multisystem markers to predict 90-day poor outcome in Chinese patients with ICH based on a multicentre cohort study. Its performance was also compared with other five recognised scoring systems, including the ICH score, ICH-FOS, ICH-GS, ICHOP score and MICH score.
Methods
Study population
We developed the model using data from the Chinese Cerebral Hemorrhage: Mechanism and Intervention (CHEERY) cohort study, which is a multicentre Chinese programme that included consecutive patients with spontaneous ICH admitted to 31 stroke centres from December 2018 to June 2021. Patients were included if they were older than 18 years and diagnosed with a spontaneous ICH on CT. Patients were excluded if they had: (1) brain haemorrhage deriving from trauma, primary subarachnoid haemorrhage, haemorrhagic conversion from ischaemic stroke and thrombolysis; (2) onset to admission more than 7 days; (3) baseline clinical and imaging information unavailable; and (4) lost to follow-up at 90 days. A total of 4248 patients had an ICH event and 2844 patients were included in this final analysis. Of those, 2111 eligible participants from 19 centres in Hubei province were designated as the training cohort, and the remaining 733 participants from five centres of other three provinces were designated as the validation cohort. Informed consent was obtained from all participants prior to the enrolment.
Clinical and imaging data collection
Demographic and clinical characteristics collected on admission include age, sex, medical history (ischaemic stroke, ischaemic heart disease, hypertension, diabetes, hyperlipidaemia), prestroke mRS, systolic blood pressure (SBP), National Institutes of Health Stroke Scale (NIHSS), imaging information (haematoma location, haematoma volume and intraventricular haemorrhage (IVH)) and laboratory tests (white cell count, haemoglobin (Hb), platelet (PLT), neutrophil-lymphocyte ratio (NLR), alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine, uric acid (UA), fasting blood glucose (FBG), international normalised ratio (INR); glomerular filtration rate (GFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation).18 The laboratory variables on admission from all 31 stroke centres were uniformly converted before statistical analysis. Initial CT scans were analysed by experienced neurologists and the ABC/2 formula was used to calculate haematoma volume. The ICH location was considered as deep if the origin of the haemorrhage appeared to be in thalamus, basal ganglia, internal capsule, deep periventricular white matter, brainstem and cerebellum. Haemorrhages originating in both deep and lobar were also considered as deep location.
Outcome
The mRS score at 90 days was obtained by telephone calls or messages from patients or their relatives. We determined the 90-day functional dependence (mRS, 3–6) as the outcome of this study.
Statistical analysis
Continuous and ordinal variables (age, SBP, NIHSS, haematoma volume, Hb, PLT, NLR, ALT, AST, GFR, FBG, UA, INR) were categorised based on clinical significance. All variables were presented as frequency with percentage and were analysed using χ2 test. Variables that reached p<0.05 in the univariate analysis were considered for multivariable analysis.
A scoring system predicting functional dependence was developed from the multiple logistic regression model. Significant variables associated with 90-day functional dependence in multivariate model were included in the ADVISING score and were weighted to assign scoring points based on the strength of association with β coefficients. Specifically, we used β coefficients of haematoma volume (30–60 mL) as a specified parameter (B), and the assigned scores for each item were calculated using the formula of βi/B and the point was rounded to the closest integer (the parameter <1 was assigned a score of 1). Hosmer-Lemeshow test was performed to assess calibration, while C-statistic was calculated to measure discrimination in both training and validation cohorts.
Furthermore, we compared the discrimination of the ADVISING score and prior ICH scores for 90-day functional dependence (mRS ≥3) after ICH in the validation cohort. Five existing ICH scores (MICH score, ICHOP score, original ICH score, ICH-GS and ICH-FOS) were selected since their components were available in our database. Pairwise areas under the curve (AUCs) between ADVISING score and other ICH scores were compared using Delong’s method to evaluate the strengths of model discrimination. We also conducted the other two ways, net reclassification index (NRI) and integrated discrimination improvement (IDI), to further assess the superiority of our score compared with others.
All tests were two tailed and p<0.05 was considered significant. Statistical analyses were performed using SPSS software (V.26.0) and R software (V.4.1.2).
Results
Patient characteristics
From 1 December 2018 to 30 June 2021, a total of 4248 patients experienced an ICH event in the CHEERY study. Of those, 1404 patients were excluded (25 patients for non-spontaneous ICH, 87 patients for the onset to admission time >7 days, 532 patients for lack of imaging data, 701 patients for lack of clinical data and 59 patients for lack of information on 90-day mRS), and the remaining 2844 patients were included in the final analysis (online supplemental figure S1). Online supplemental table S1 shows comparisons of baseline characteristics between the excluded and the included data sets. Compared with excluded samples, the analysed data set had a lower rate of IVH occurrence and better 90-day outcomes. After exclusion of patients with IVH extension accompanied with unavailable haematoma volume (which was not calculated for irregular shapes), these differences were eliminated. A total of 2111 (74.2%) eligible patients from 19 stroke centres of Hubei province were included in the training cohort, while 733 (25.8%) patients from five stroke centres of other three provinces were included in the validation cohort. The median age of the included patients was 62 (IQR 53–70) years, and 67.5% of them were male. A total of 1439 (50.6%) were functionally dependent (mRS ≥3) at 90 days after ICH. Patients in the training cohort were older, had a lower rate of ischaemic stroke and a lower baseline NIHSS, and less proportion of 90-day functional dependence. Patient characteristics and outcomes of the training, validation and total cohorts were listed in table 1.
Supplemental material
Baseline characteristics and outcomes of the study
Univariate analysis of associations with 90-day functional dependence after ICH
Table 2 showed the univariate analysis of variables associated with 90-day functional dependence (mRS ≥3) in the training cohort. For clinical applicability, continuous and ordinal variables were categorised and the cut-off values were chosen based on clinical implications. Patients who suffered from functional dependence were more likely ≥60 years of age, had SBP ≥180 mm Hg and a baseline NIHSS ≥6. Their ICHs had a deeper location and IVH, and haematoma volume was ≥30 mL. Abnormal clinical laboratory values included white cell count >10×109/L, Hb <120 g/L, NLR >10, AST >40 U/L, GFR <90 mL/min/1.73 m2, FBG ≥7.0 mmol/L and INR ≥1.2.
Univariate analysis comparing patients with and without functional dependence in training cohort
Predictors of 90-day functional dependence after ICH
Multivariable logistic regression model was built to identify independent predictors of functional dependence at 90 days after ICH. After adjusting for confounding factors, nine variables were identified as independent predictors of functional dependence, including age ≥60 years, NIHSS score, deep location, haematoma volume, NLR >10, AST >40 U/L, GFR <90 mL/min/1.73 m2, FBG ≥7.0 mmol/L and INR ≥1.2. No statistical significance was observed at the associations with SBP (≥180 vs <180 mm Hg, OR 1.1; 95% CI 0.9 to 1.4; p=0.412), IVH (OR 1.1; 95% CI 0.8 to 1.7; p=0.560) or Hb (<120 vs ≥120 g/L, OR 1.3; 95% CI 1.0 to 1.7; p=0.081) (table 3).
Multivariate analysis for factors associated with functional dependence in training cohort
The ADVISING score
The ADVISING (age, deep location, volume of haematoma, NIHSS score, AST, INR, NLR, GFR, FBG) score was thus developed based on the multivariate logistic analysis result in the training cohort. Each of the nine predictors in the scoring system was weighted and points assigned based on the strength of association with β coefficients. The range of ADVISING scores was between 0 and 12, with a score ≥9 indicating a hundred per cent of functional dependence (mRS ≥3) (table 4). In fact, the proportion of patients who suffered from functional dependence at 90 days increased with higher scores both in training cohort and validation cohort, as shown in table 5 and figure 1. In order to promote the clinical practice of ADVISING score, we dichotomised the score to 0–4 for low risk and 5–12 for high risk of functional dependence, and determined. The cut-off value was based on the optimal performance of receiver operating characteristic (ROC) curve analysis. Among them, 742 (77.2%) patients in the training cohort and 293 (81.2%) in the validation cohort had a score ≥5, which predicted 71.6% and 72.9% sensitivity, and 79.6% and 79.5% specificity in the training and validation cohorts, respectively. The detailed information dichotomised test characteristics were shown in table 5.
Determinants of the ADVISING score
Proportion of patients with functional dependence stratified by ADVISING score

The proportion of patients suffering from functional dependence at 90 days in training and validation cohorts.
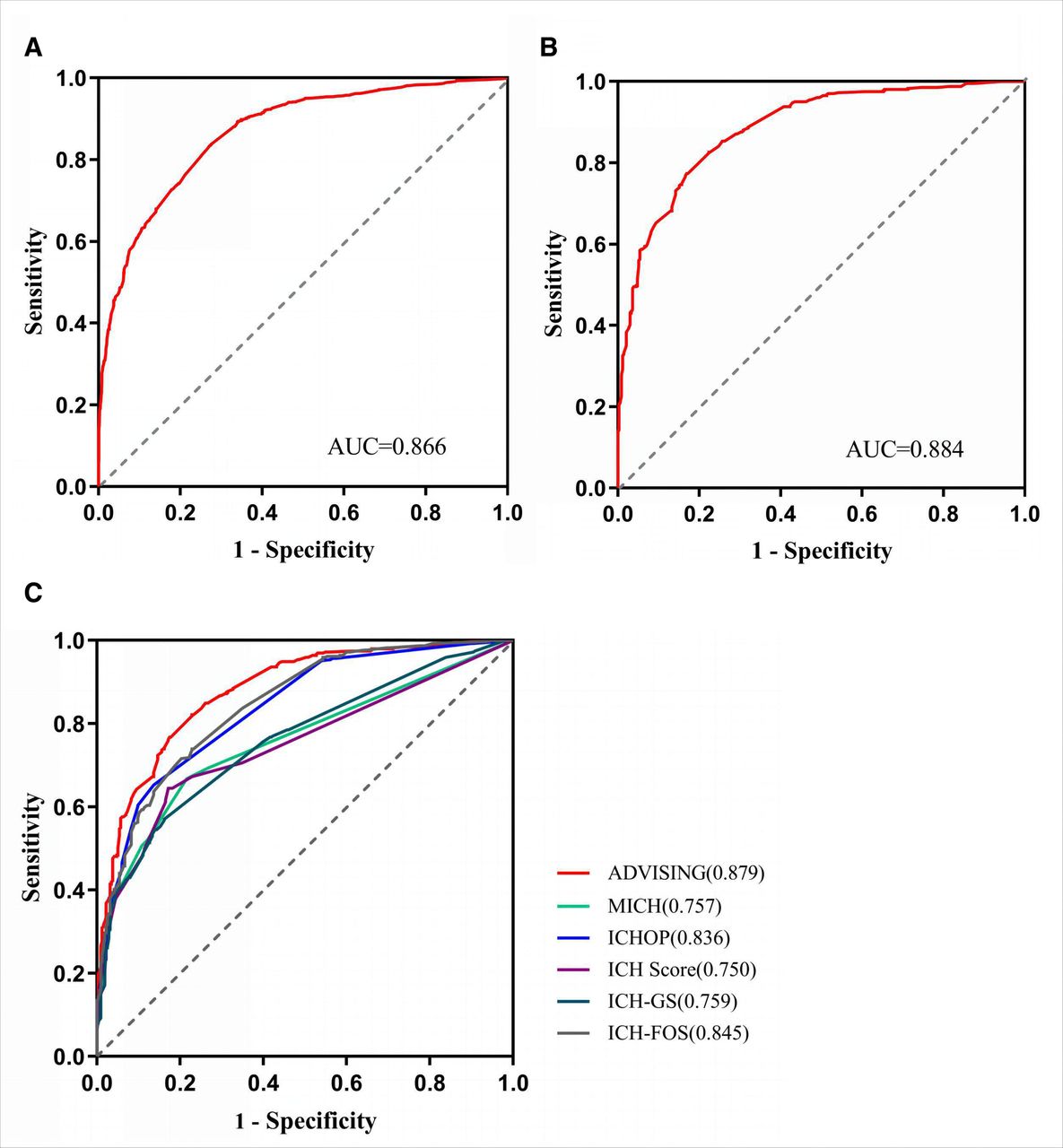
The ADVISING score demonstrated good discrimination and calibration in training cohort (C-statistic, 0.866; p value of Hosmer-Lemeshow test, 0.195) and validation cohort (C-statistic, 0.884; p value of Hosmer-Lemeshow test, 0.853). Figure 2A,B shows the ROC of the model.

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve for 90-day functional dependence (modified Rankin Scale (mRS) ≥3). (A) ROC curve of ADVISING score in training cohort. (B) ROC curve of ADVISING score in validation cohort. (C) ROCs of ADVISING score and the other five intracerebral haemorrhage (ICH) scores in validation cohort. The values in parenthesis in (B) and (C) are areas under the curve (AUCs). ICH-FOS, ICH Functional Outcome Score; ICH-GS, ICH Grading Scale; ICHOP, ICH Outcomes Project; MICH, modified ICH.
Comparing the ADVISING score with five other existing ICH scores
We compared the discriminative performance of the ADVISING score with five existing ICH scores including MICH score, ICHOP score, original ICH score, ICH-GS and ICH-FOS in the validation cohort (n=733). Among them, 27 patients were excluded for missing information on elements of other scores. The comparison of screening characteristics and scores between the ADVISING score and the previous risk scores was shown in online supplemental table S2. For functional dependence at 90 days after ICH, AUCs ranged from 0.750 to 0.879 (ICH score, 0.750; MICH score, 0.757; ICH-GS, 0.759; ICHOP score, 0.836; ICH-FOS, 0.845; ADVISING score, 0.879). The ADVISING score had the highest AUC. The pairwise difference in AUCs between the ADVISING and other scores showed statistical significance (all p<0.001) (online supplemental table S3). Figure 2C showed the ROCs of the mentioned scores with regard to functional dependence (mRS ≥3) at 90 days. To better evaluate the performance of predicting scores, we further calculated NRI and IDI in validation cohort (n=706). Reclassifications for patients with and without functional dependence were summarised in online supplemental table S4. The cut-off of 50% for risk categories was chosen based on the actual 90-day dependence rate reported in previous literature.19 Both NRI and IDI were estimated to be greater than zero (p<0.001) in pairwise comparison, with the greatest net gain in the reclassified 18.4% proportion and the highest improved ability in discrimination of 19.6%, suggesting that the ADVISING score had a significant improvement in performance compared with the other five existing ICH scores.
Discussion
We developed a novel prognostic scoring system for patients with spontaneous ICH from the nationwide multicentre samples in the CHEERY study. ADVISING score exhibited excellent discriminative ability, and was well calibrated and validated in the external cohort. Compared with other ICH scoring models, ADVISING score was developed including well-recognised predictors for prognosis, and selecting multisystem indicators to reflect the damage of other organs after ICH, which is expected to provide the new train of thoughts for screen, diagnosis, prophylaxis and treatment of ICH.
Growing evidence suggests that stroke is a systemic disease affecting many organ systems beyond the brain. Injuries after ICH consist of two main parts: one is the primary injury, including clot removal, haematoma expansion and ischaemia; the secondary injury included thrombin formation, inflammation, complement interaction, Hb fluctuation, iron deposition, free radical formation, glutamate release, cell death pathway apoptosis, etc.20 Stroke-related systemic responses and inflammatory/immune dysregulations may play important roles in brain injury, recovery and outcome.21
Multiple organ injuries after ICH include liver, kidney and coagulation system, mainly caused by circulating inflammatory factors and oxidative stress products.15 16 22–24 Above all, liver injury usually leads to further haemostatic disorders. Population-based studies have found that patients with ICH have an increased rate of liver dysfunction, including fibrosis and cirrhosis, with significant impairment of PLT aggregation and reduction of α2 antifibrinolytic activity, which in turn increase risks of ICH.25 26 As a sensitive marker of liver function, AST was associated with worsening of clinical outcomes in ICH.13 Second, renal function impairment, characterised by endothelial dysfunction and lipohyalinosis, is also a common complication after ICH.27–29 Patients with ICH with chronic renal insufficiency have more white matter changes, haematoma growth and perihaematoma oedema,30 31 possibly due to renal insufficiency inhibiting coagulation system and PLT function through microparticles and microRNA.32 GFR, as a common indicator reflecting renal function, was identified as an independent predictor of in-hospital mortality after ICH in a previous study.14 In addition, reactive hyperglycaemia, mediated by cortisol and norepinephrine, induces the opening of the blood–brain barrier and causes vasogenic cerebral oedema by directly inducing neuronal apoptosis, increasing inflammatory cytokines such as tumour necrosis factor alpha and interleukin-1 and promoting the production of oxygen-free radicals after ICH.33 34 Finally, our study found that higher baseline INR was associated with a 3-month poor outcome, which was in line with the previous study.16 In our study, we combined the above multisystem injury markers with traditional prognostic predictors and generated a novel prognostic system for patients with ICH.
Elevated blood leucocyte count was associated with higher disease severity, larger ICH volume and worse outcomes.35 Lower lymphocyte count was associated with larger haematoma volume and an independent predictor of risk of infection and 3-month mortality in ICH.36 Previous studies showed that NLR may be a useful biomarker for stroke severity and outcome, and higher NLR is associated with larger baseline haematoma volume and higher initial NIHSS.37 38 In our study, NLR was also included in the ADVISING score, which reflected the inflammatory and immune dimension of stroke-related systemic injuries and responses.
The robustness of this study is driven by large-sample, nationwide multicentre data. However, this study also had several limitations. First, this study only included data on Chinese people. Second, outcome data at 3 months were analyzed only, long outcomes like 1 year or 3 years of follow-up need further studies. In the mean time, the outcome was assessed by telephone interview and text, which are not as accurate as a face-to-face interview. Third, the laboratory variables were only drawn once on admission and we could not observe the dynamic changes of these indicators. Fourth, continuous and ordinal variables were transformed into categorical variables in the scale, with cut-off values determined according to the frequently used clinical implications rather than ROC analysis, which may be not statistically rigorous. Fifth, some patients with IVH were excluded for lacking of haematoma volume (which was not calculated for irregular shapes), leading to lower IVH occurrence rate and better outcomes of the analysed data set compared with excluded samples. Furthermore, we chose logistic regression model for creating this scoring system in order to compare this one with previous established models. Advanced methods including machine learning may be used in our future work to overcome the shortcomings of logistic regression. In addition, to better understand the mechanisms and interactions of multisystem injury after ICH, animal studies on biochemical mechanisms were expected in the future work.
In conclusion, we developed and independently validated a novel clinical prediction score for patients with ICH for their clinical outcomes, which features good calibration and discrimination.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Research Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China (approval number: 2018-S485). Participants gave informed consent to participate in the study before taking part.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YW, HG, SC and JC are joint first authors.
QH and BH contributed equally.
YW, HG, SC and JC contributed equally.
Contributors YW, HG and SC are joint first authors. BH was responsible for the concept and design of the study, and responsible for the overall content as the guarantor. QH and YW did the literature search and wrote the manuscript. HG and SC analysed the data and completed the tables and figures. DW revised the manuscript. JC and KS did the administrative, technical or statistical support. Other authors helped with data collection and interpretation. All authors contributed to the article and approved the submitted version.
Funding This study was funded by the Research and Development Program of China (2018YFC1312200) and the National Natural Science Foundation of China (81820108010, 81901214, 82071335).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.