Article Text

Abstract
Background and purpose Haemodynamics around the middle cerebral artery (MCA) and lenticulostriate arteries is believed to play important roles in the vascular rupture and local haemodynamics is subject to vascular geometry. Nonetheless, the relationship between the geometric features of MCA and spontaneous basal ganglia intracerebral haemorrhage (ICH) has not been investigated. To examine the relationship between the MCA geometric features and spontaneous basal ganglia ICH.
Methods This study was of retrospective and observational nature. The study recruited 158 consecutive hospitalised patients with consecutive CT-confirmed unilateral spontaneous basal ganglia ICH. Clinical data were extracted from electronic medical records, and imaging data were evaluated by two trained radiologists. The MCA-related geometric features were examined and their relationship with spontaneous basal ganglia ICH was analysed. Haemodynamic analyses under different MCA structural features were conducted.
Results Compared with the contralateral MCA, the ipsilateral MCA had greater M1 diameter ratio (proximal/distal) and a smaller M1/M2 angle and MCA bifurcation angle (p<0.01). Imaging study showed differences in the MCA shape in both sides on coronal plane (p<0.05). These MCA features were significantly correlated with the spontaneous ICH in basal ganglia. The greater M1 diameter ratio (proximal/distal), the inferior-oriented M1, the smaller M1/M2 angle and the superior-oriented M1 conditions increased the pressure, from high to low. The greater M1 diameter ratio (proximal/distal) and the inferior-oriented M1 increased the shear stress at the distal end of M1 segment.
Conclusions The geometric features of MCA were significantly related to the spontaneous ICH in basal ganglia. The risk of haemorrhage, from high to low, included the greater M1 diameter ratio (proximal/distal), the inferior-oriented M1 (distal end), the smaller M1/M2 angle and the superior-oriented M1. Mechanistically, these vascular structural features contribute to increased vascular wall pressure and shear stress, which eventually lead to haemorrhage.
- hemorrhage
Data availability statement
Data are available on reasonable request. All free text entered below will be published.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Although spontaneous intracerebral haemorrhage (ICH) accounts for less than 20% of cases of stroke, it represents the most serious type of the condition and has the highest mortality among all forms of stroke.1 Spontaneous ICH in the basal ganglia (the most common site) is caused by the rupture of lenticulostriate arteries (LSAs), the perforating branches of the ipsilateral middle cerebral artery (MCA).2 As we know it, this region is also a frequent site of ischaemic stroke. Haemorrhagic and ischaemic strokes had some risk factors in common, such as hypertension, diabetes, hyperlipaemia, smoking and alcohol use.3 In clinical practice, it is still difficult to identify populations who are at higher risk for haemorrhage. Haemodynamics around the MCA and LSAs is believed to play important roles in the vascular rupture and local haemodynamics can be impacted by vascular geometry.4–8 Previous histological evaluation found that, unlike ischaemic stroke, non-stenotic atherosclerotic MCAs were more common in ICH and it was hypothesised that arterial hypertension spread more easily to the small branches through the main vascular trunks without luminal narrowing, resulting in vascular rupture and haemorrhage.9 Therefore, we are led to speculate that some geometric features of MCA, which presumably affect both local haemodynamics and wall mechanics, might make the region more vulnerable to spontaneous basal ganglia ICH.
Studies have confirmed that the geometry of intracranial artery is an important factor in the development of atherosclerotic plaque.10–12 The arterial geometry, by haemodynamically working on the endothelia, can influence the growth of atherosclerotic plaques through the haemodynamic effect, leading to a consistency in geometry among different plaques.13 Moreover, the geometric properties of plaque can directly influence the risk of plaque rupture.14 15 In fact, the plaque features, including geometry, are found to be associated with the acute symptoms in MCA.16 Nonetheless, the haemodynamic mechanisms underlying the plaque formation have not been fully clarified.
In recent years, computational fluid mechanics has emerged as a powerful tool to more precisely explore the cause of cerebral haemorrhage, to probe the mechanism underlying the complex physical events in brain and to serve as a supplement to other medical equipment for higher precision.17–21 Researchers reportedly simulated the cerebral circulation to look into the pathogenesis of ICH.22 However, to our knowledge, the relationship between the MCA geometric features and spontaneous basal ganglia ICH have not been investigated, especially by using the computational fluid dynamic (CFD) technique. The objective of this study was, therefore, to examine the MCA geometric features and their effect on the development of spontaneous ICH in basal ganglia by means of CFD simulation. We tried to identify local geometric risk factors that could serve as indicators for identifying populations who are at high risk of spontaneous basal ganglia ICH.
Methods
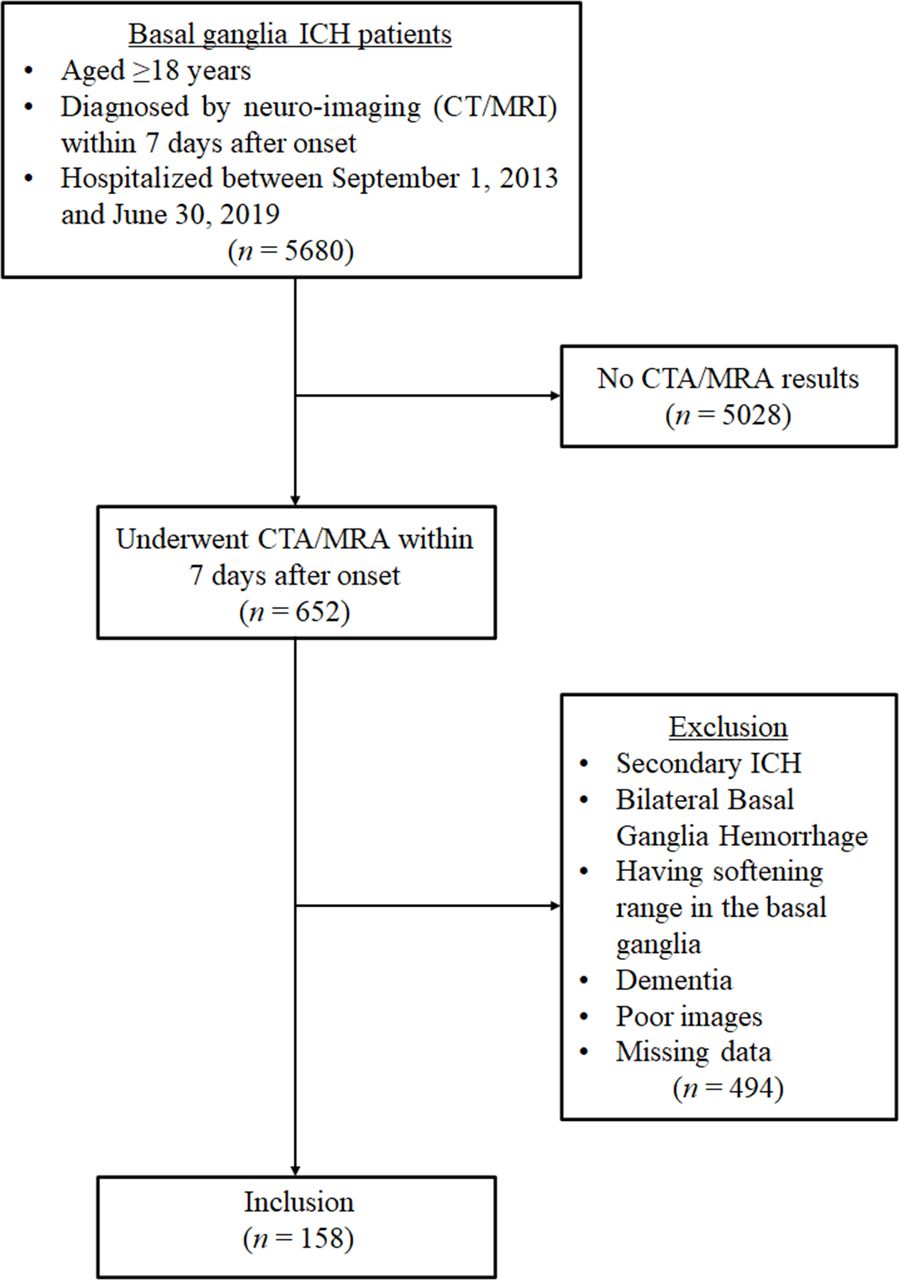
Enrolled into this study were the consecutive patients who had CT-confirmed unilateral spontaneous basal ganglia ICH (>18 years) and had received MR angiography (MRA)/CT angiography (CTA) (within 7 days of onset) in Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, between 1 September 2013 and 30 June 2019. The flow diagram for patient selection is shown in figure 1. The clinical data of the patients were collected from the institutional medical database. The parameters used in our study included the MCA-related variables and other items that might be related to spontaneous basal ganglia ICH (figure 2). The CFD analysis using the scFLOW module from MSC Cradle was performed to simulate the cerebral blood flow. Statistical analysis was performed by employing Statistical Product and Service Solutions V.12.0 for Windows. Details are given in online supplemental methods.
Supplemental material

Flow diagram of patient selection. CTA, CT angiography; MRA, MR angiography; ICH, intracerebral haemorrhage.
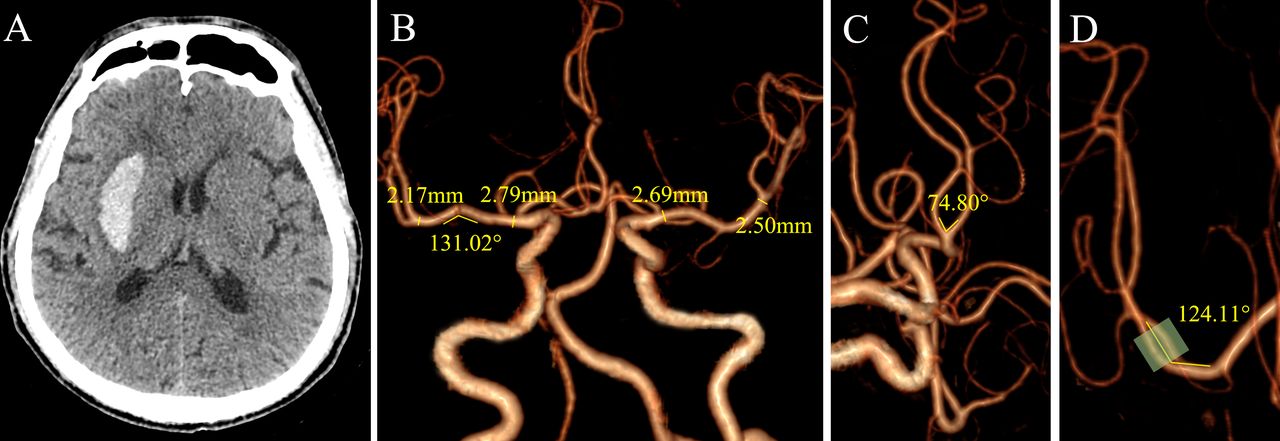
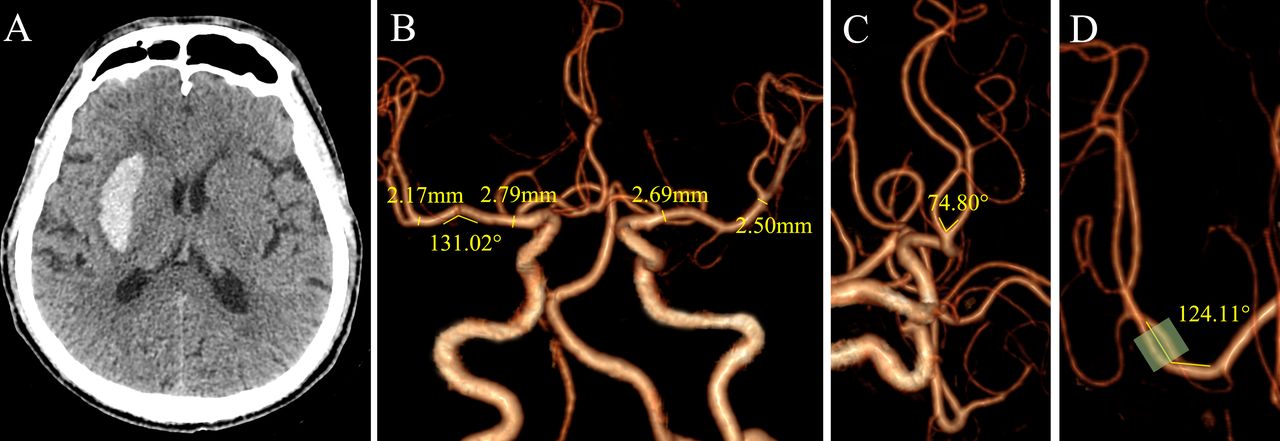
A right spontaneous basal ganglia ICH (A) and measurement of the M1 length (B), M1 proximal/distal diameter (B), M1 curve orientation (B), MCA bifurcation angle (C) and M1/M2 angle (D). ICH, intracerebral haemorrhage; MCA, middle cerebral artery.
Results
Basic data
Finally, 158 patients were included in the present analysis. The features of the study population are shown in table 1.
Clinical characteristics of patients with spontaneous basal ganglia ICH (N=158)
MCA Geometric Features of MCA
The MCA geometric features are summarised in table 2.
MCA geometric features (N=158)
Cerebral artery model
The model of human cerebral artery was based on the medical image of human brain CT scan and was generated by three-dimensional reconstruction by using Mimics commercial medical image processing software. The reconstructed model was measured (figure 3). The LSAs divided to branches of four levels (online supplemental figure 2). On the basis of clinical statistical data, models of 5 different lesion MCA geometric features were established (online supplemental figure 3), and then the vascular wall pressure, wall shear stress, and flow rate were observed by employing CFD technology.
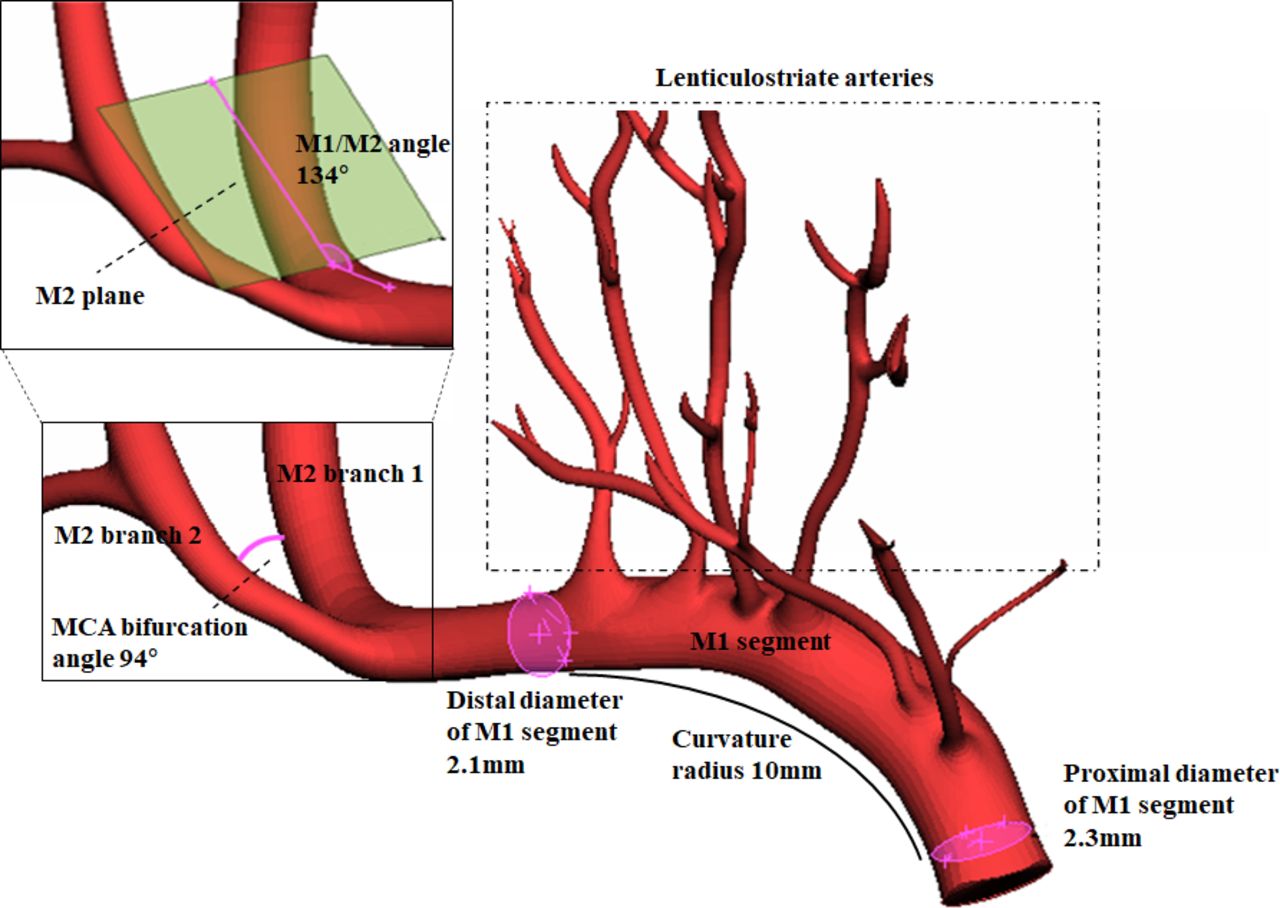
Primary cerebral artery model and measurement of the MCA-related geometric features. MCA, middle cerebral artery.
Arterial wall pressure distribution
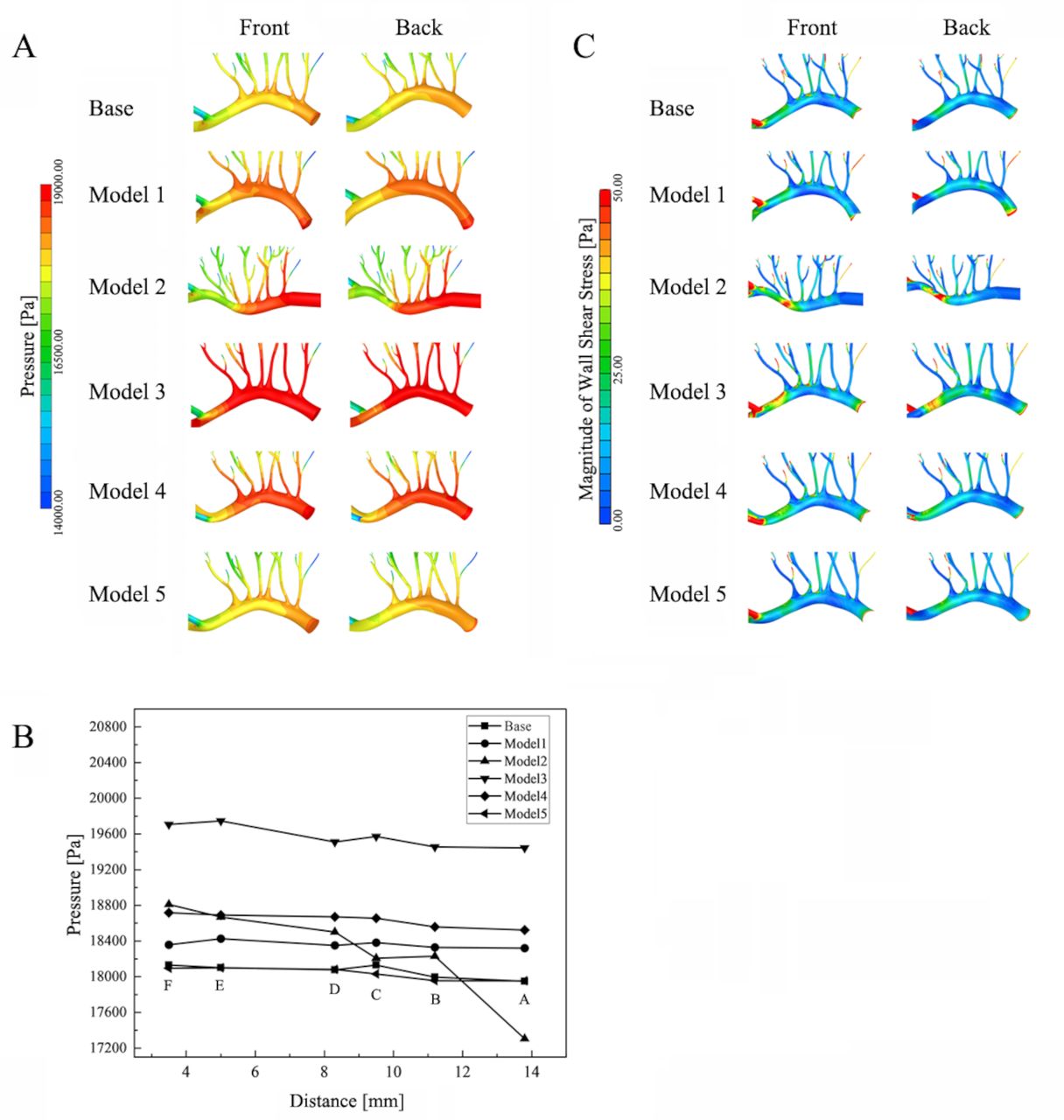
The cloud diagram of the arterial wall pressure distribution and pressure values on the axis of the arterial wall are shown in figure 4A,B. The pressure gradient generally decreased along the flow direction. The highest pressure was about 19.7 kPa at the blood inlet of the proximal end of M1. In the model 1, the wall pressures of M1 and all the level-1 branches of 6 LSAs were marginally higher than that of the basal condition. In the Model 2, the wall pressure at the proximal end of the M1 was relatively high while the distal wall pressure was relatively low. The pressures of the E and F branches (levels 1–3) and at openings of the B and D branches of the LSAs were also elevated. In the Model 3, the pressure, being the highest in all conditions, obviously increased in the M1 and all the level 1–3 branches of 6 LSAs, as compared with other conditions. In the Model 4, the wall pressure was high in the proximal end and dropped at the distant end. The pressure was elevated in all the level 1–2 branches of 6 LSAs and decreased along the flow direction. In the model 5, the working condition exerted little effect on the wall pressure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Haemodynamics analyses. (A) Arterial wall pressure distribution nephogram. (B) Arterial wall pressure distribution diagram. (C) Arterial wall shear stress distribution cloud chart.
Model 3 had the highest pressure, followed by model 2 (distal pattern), model 4 and model 1. The pressure gradients in the centre of base, model 1, model 4 and model 5 were relatively gentle. The pressure did not fluctuate significantly at the M1, but only decreased at the blood inlet and the distal end of M1 segment. The pressure dropped by 0.35–0.4 kPa. In the model 2, the pressure at the centre of the vessel fluctuated substantially. And there was a long low pressure area at the distal end of the M1 segment.
Arterial wall shear stress distribution
The distribution of the arterial wall shear stress under the six working conditions is shown in figure 4C. The distribution was more complicated, with the wall shear stress ranging from 1 to 50 Pa. There was a low shear stress area at the bottom of the level-1 branches of LSAs. The lower shear stress area at the upper arch of the M1 was larger in the model 1 than in the basal condition. In the model 2, there was a large shear stress (45–50 Pa) area at the distal end of M1 and the A and B branch opening of the LSAs also increased. In the model 3, the shear stress at the distal end of M1 increased and so did the B and C branch opening of the LSAs. In the model 4, the shear stress rose at the distal pattern of M1. Compared with the basal condition, the shear stress distribution of model 5 was essentially the same.
Discussion
In this study, a rationale was addressed on the association between the MCA geometric features and spontaneous basal ganglia ICH, by using numerical simulation. Our results showed that, the MCA geometric features, in terms of M1 diameter ratio (proximal/distal), M1 curve orientation on coronal image plane, and M1/M2 angle, were significantly related to the spontaneous ICH in basal ganglia. The factors that increase the risk of haemorrhage, from high to low, include the greater M1 diameter ratio (proximal/distal), the inferior-oriented M1 (distal end), the smaller M1/M2 angle, and the superior-oriented M1 segment. Our results suggested that these vascular structural features contribute to the increased arterial wall pressure and shear stress, which may pathologically underlie the development of haemorrhage.
Vascular geometry has been suggested as a factor that regulates haemodynamics and consequently influences the development of vascular diseases, such as atherosclerosis and cerebral aneurysmal disease, in which blood exerts excessive forces on the vascular wall.23 24 In reality, the vascular anatomy varies substantially. Some geometric features may be ‘geometric risk factors’ that bring about high haemodynamic shear stresses on the local vascular wall.25 Like the aforementioned diseases, spontaneous ICH is also presumed to be related to the geometry of intracranial vessels. Zhang et al 22 found that the angle between the MCA and the internal carotid artery and the distance between the beginning of the median artery and superior trunk were significantly related to ICH. Lee et al 7 also reported that putaminal ICH occurred more frequently on the side of the dominant anterior cerebral artery first segment. These might be ascribed to local haemodynamic changes caused by certain geometrical variations, but the assumption still awaits further confirmation.
Most spontaneous ICHs occurs in the basal ganglia, resulting from the rupture of the LSAs which bear more wall pressure or shear stress.26 27 LSAs are small branches of the MCA and the main perforators supplying basal ganglia.4 Therefore, the haemodynamics of LSAs is presumably affected by the MCA. Technically, direct measurement of the pressure or sheer stress of intracranial arteries remains a significant challenge in clinical practice. However, measuring the geometry of intracranial arteries is convenient, given the wide application of noninvasive vascular imaging, such as MRA and CTA. LSAs cannot be well visualised by MRA/CTA. Therefore, we focused on the MCA, with an attempt to find some geometric features that help predict the risk for ICH taking place in this deep brain area without obtaining local haemodynamic data.
In this study, a set of geometric features, presumed to impact the MCA haemodynamics, were then selected and measured. We found that, unlike ischaemic stroke, atherosclerotic plaque and stenosis at M1 segment were rare, which is consistent with the findings of an autopsy study.9 As with healthy population,28 curved MCAs were more prevalent than their straight counterparts. The dorsal and superior-oriented M1 segment curves were found to be the most common shape of MCAs in our study. This curve orientation is just opposite to that observed in a previous study on atherosclerotic MCAs,11 and this disparity might be attributed to the difference in subjects selection between the two studies. But the proportion of the curved M1 segment and inferior-oriented M1 segment curves were higher in the haemorrhage side. Further analysis showed that M1 diameter ratio (proximal/distal), M1 curve orientation on coronal image plane, M1/M2 angle and MCA bifurcation angle were independently associated with basal ganglia ICH. However, no correlations were found between these geometric features and haematoma volume (online supplemental table 1) or severity (online supplemental table 2), respectively.
A question presents itself: Whether these MCA structural features may raise local haemodynamic stresses and further result in haemorrhage? Further haemodynamic analyses revealed that the greater M1 diameter ratio (proximal/distal), the inferior-oriented M1 (distal end), the smaller M1/M2 angle and the superior-oriented M1, from high to low, could significantly increase M1 segment and LSAs wall pressure. The wall pressure gradient generally decreased along the flow direction under all these conditions. The elevated wall pressure of LSAs might lead to vascular rupture and haemorrhage in the condition that the brain pressure increases due to some unexpected stimulation. With greater M1 diameter ratio (proximal/distal), the wall pressure of all the level 1–3 branches of 6 LSAs were significantly elevated, rendering the areas prone to rupture. With smaller M1/M2 angle and superior-orientation of M1, the rupture-prone zones were at all the level-1 branches of six LSAs. Inconsistent with the aforementioned conditions, the inferior-orientation of M1 substantially increased the pressure of the proximal LSA branches. The rupture-prone zones were at the E and F branches (levels 1–3) and openings of the B and D branches. The role of the low pressure aera formed at the distal end of M1 warrants further study, and some unknown factors might contribute to the vascular rupture. Moreover, the wall shear stress under the four conditions ranged from 1 to 50 Pa. This might explain why M1 segment atherosclerotic plaques and segmental stenosis are rare in ICH patients since atherosclerotic plaques usually develop in areas where the wall shear stress is lower than 0.1 Pa.23 With greater M1 diameter ratio (proximal/distal) and the inferior-orientation of M1, the shear stress at the distal end of M1 segment was greatly increased, leading by a high blood velocity. The high wall shear stress has a greater scouring force on the inner wall of the vascular, causing damage to the endothelial cells of the vessels. This might increase the risk of distal LSAs rupture and haemorrhage. Furthermore, it is worth noting that curve orientation and curvature were two important factors that are associated with the risk of haemorrhage when M1 is curved. The inferior-oriented M1 segment is more susceptible to haemorrhage more than the superior-oriented one. We are led to conclude that the greater the positive curvature, the higher the pressure, and the smaller the distal shear stress. On the contrary, the smaller the negative curvature, the higher the pressure, and the greater the distal shear stress. Therefore, these four MCA structural features statistically suffice to cause basal ganglia ICH by increasing the arterial wall pressure and shear stress. The risk of haemorrhage, from high to low, included the greater M1 diameter ratio (proximal/distal), the inferior-oriented M1, the smaller M1/M2 angle and the superior-oriented M1 segment.
Our study had some limitations. First, the MCA geometric features selected in the study might not cover all parameters that affect local haemodynamics. Other geometric parameters, such as wall thickness, might also be important determinants, but these data are not available from the MRA/CTA images. Second, LSAs, which are subject to structural variation and sufficient to impact local haemodynamics, were not covered by this study since they could not be visualised by MRA/CTA. Third, this study was retrospective, single-centred and self-controlled nature. Further prospective multisetting studies in larger populations are needed.
Summary
In conclusion, our results are potentially of clinical importance. We confirmed that geometric risk factors were at work in the development of basal ganglia ICH. Some MCA geometric features, such as greater M1 diameter ratio (proximal/distal), curved M1 on coronal image plane, and smaller M1/M2 angle, were indicative of high risk of ICH in this deep brain area without support of local haemodynamic data. Identification of these risk features of the MCA might greatly facilitate the control and prevention of ICH in basal ganglia.
Supplemental material
Supplemental material
Data availability statement
Data are available on reasonable request. All free text entered below will be published.
Ethics statements
Patient consent for publication
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DL and GZ are joint first authors.
DL and GZ contributed equally.
Correction notice This article has been corrected since published online first. DL and GZ contributed equally and are joint first authors.
Contributors MW are responsible for the overall content as the guarantor. Concept and design: MW; acquisition, analysis or interpretation of data: MW, DL, GZ, YW, JL, PC, XY; drafting of the manuscript: MW, DL, GZ, YW, PC, XY, CZ; critical revision of the manuscript for important intellectual content: MW; statistical analysis: JL, PC, XY; obtained funding: MW; administrative, technical or material support: MW, DL, GZ, YW, JL, PC and XY; supervision: MW.
Funding This work was supported by grants from the Program of National Natural Science Foundation of China (81301001, 81301248, 81801181).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.