Article Text

Abstract
Background/objective This study compares the global disability status of patients who had a mild ischaemic stroke at 30 and 90 days poststroke, as measured by the modified Rankin Scale (mRS), and identifies predictors of change in disability status between 30 and 90 days.
Methods The study population included 1339 patients who had a ischaemic stroke enrolled in the Mild and Rapidly Improving Stroke Study with National Institutes of Health (NIH) stroke score 0–5 and mRS measurements at 30 and 90 days. Outcomes were (1) Improvement defined as having mRS >1 at 30 days and mRS 0–1 at 90 days OR mRS >2 at 30 days and mRS 0–2 at 90 days and (2) Worsening defined as an increase of ≥2 points or a worsening from mRS of 1 at 30 days to 2 at 90 days. Demographic and clinical characteristics at hospital arrival were abstracted from medical records, and regression models were used to identify predictors of functional improvement and decline from 30 to 90 days post-stroke. Significant predictors were mutually adjusted in multivariable models that also included age and stroke severity.
Results Fifty-seven per cent of study participants had no change in mRS value from 30 to 90 days. Overall, there was moderate agreement in mRS between the two time points (weighted kappa=0.59 (95% CI 0.56 to 0.62)). However, worsening on the mRS was observed in 7.54% of the study population from 30 to 90 days, and 17.33% improved. Participants of older age (per year OR 1.02, 95% CI 1.00 to 1.03), greater stroke severity (per NIH Stroke Scale (NIHSS) point at admission OR 1.17, 95% CI 1.03 to 1.34), and those with no alteplase treatment (OR 1.72, 95% CI 1.11 to 2.69) were more likely to show functional decline after mutual adjustment.
Discussion A quarter of all mild ischaemic stroke participants exhibited functional changes between 30 and 90 days, suggesting that the 30-day outcome may insufficiently represent long-term recovery in mild stroke and longer follow-up may be clinically necessary.
Trial registration number NCT02072681.
- Risk Factors
- Stroke
Data availability statement
Data may be obtained from a third party and are not publicly available. The authors are not authorised to make the data publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Functional status at 30 days poststroke has been shown to be a reliable predictor of functional status at 90 days, but whether this applies to survivors of mild strokes is not known, and can have important clinical and research implications.
What this study adds
Using a conservative definition of change in Modified Rankin Scale, we found that a quarter of all mild stroke survivors exhibited functional changes between 30 and 90 days poststroke, with 8% declining and 17% improving.
How this study might affect research, practice or policy
Although the use of a 30-day functional outcome assessment would improve clinical study participant attrition and expedience of results, possibly decrease costs, and provide an earlier indicator of long-term functional prognosis, the results indicate that a 90-day outcome measure should remain the standard practice in clinical studies of patients who had a mild stroke.
Introduction
The final disability status after an ischaemic stroke has typically been assessed at 90 days in clinical trials. However, it has been shown that the functional status at 30 days poststroke, measured by the modified Rankin Scale (mRS),1 is a reliable predictor of functional status at 90 days.2 In fact, the 30-day mRS alone explained 65.6% of the variance in the 90-day mRS. Whether this is true specifically among the survivors of mild strokes is not known, as they have been understudied. If poststroke functional status in mild stroke could be reliably assessed at 30 days rather than 90 days, it could potentially benefit patients, clinicians and researchers by allowing assessment at an earlier time after stroke, reducing lost to follow-up and accelerating planning for reintegration into the patient’s usual activities, including work. Clinical trials of acute treatments for mild ischaemic stroke could be done with a shorter follow-up period, reducing the time to complete the trials and thereby realising cost savings. Therefore, the goal of this study is to compare the global disability status of patients who had a mild ischaemic stroke at 30 and 90 days poststroke and identify predictors of change in disability status between 30 and 90 days, including alteplase treatment.
Methods
The design and methodology of the Mild and Rapidly Improving Stroke Study (MaRISS) has been described previously.3 The primary objectives of MaRISS were to identify the long-term outcomes of patients with mild and rapidly improving strokes as well as the predictors of long-term outcomes, with a particular focus on alteplase treatment. MaRISS is a prospective observational study of patients arriving to the hospital within 4.5 hours of a mild (NIH Stroke Scale (NIHSS) 0–5) or rapidly improving stroke. The patients were treated at 100 MaRISS hospitals (online supplemental table 1), selected among those participating in the American Heart Association’s (AHA) Get With The Guidelines (GWTG) Stroke quality improvement programme, with >300 annual stroke discharges, and identified to represent the overall geographical and academic/non-academic status of the overall GWTG-Stroke hospital distribution. All MaRISS sites completed an online training module that focused on the mRS. We excluded all patients with an mRS >2 prior to their stroke and those with complete resolution of symptoms at arrival. Recruitment into the study was ascertained after the decision to administer thrombolytic agents was made. The current analysis was restricted to study participants with NIHSS 0–5 at baseline and a final diagnosis of an ischaemic stroke. IQVIA (Parsippany, New Jersey) serves as the data collection and coordination centre.
Supplemental material
Demographic and clinical characteristics at hospital arrival were abstracted from medical records by trained hospital personnel as part of GWTG-Stroke. The mRS-9Q version4 was used to limit inter-rater variability; it was obtained at 30 days and again at 90 days through a structured telephone interview performed by trained and certified site study personnel. A good outcome was defined as mRS 0–1. Improvement from 30 to 90 days was defined as having mRS>1 at 30 days and mRS 0–1 at 90 days OR mRS>2 at 30 days and mRS 0–2 at 90 days. Worsening from 30 to 90 days was defined as an increase of two or more points or a worsening from mRS of 1 at 30 days to 2 at 90 days. A weighted kappa statistic was calculated to represent agreement between the 30-day and 90-day mRS.
Univariate χ2 analyses were used to describe categorical patient and treatment characteristics in relation to mRS improvement (improvement vs no improvement) and mRS worsening (worsening vs no worsening). The potential predictors of interest included sex, race/ethnicity, insurance status, off hours arrival, stroke mechanism, altered consciousness, weakness, aphasia, hypertension, diabetes mellitus, hyperlipidaemia, tobacco use, prior stroke or transient ischemic attack (TIA), atrial fibrillation (AF), coronary artery disease (CAD)/prior myocardial infarction (MI), heart failure, carotid disease, peripheral vascular disease, anticoagulation use, antiplatelet use, alteplase treatment, haemorrhagic complication of alteplase treatment and endovascular therapy. The univariate relationships between age and mRS worsening and improvement were examined using t-tests, and the relationships between baseline NIHSS and mRS worsening and improvement were examined using the Wilcoxon rank sum test. Variables that were significantly associated with worsening or improvement in univariate analyses (p<0.05) were included in mutually adjusted multivariable logistic regression models using the complete case approach due to minimal missing data. In these models the dichotomous outcomes were mRS worsening and improvement, as described above, and all variables that reached statistical significance in univariate analyses were included simultaneously as independent variables in addition to age and NIHSS at admission (included a priori), and we accounted for clustering by hospital.
The authors are not authorised to make the data publicly available.
Results
The MaRISS study population included 1765 participants with a mild stroke (NIHSS 0–5) and an ischaemic stroke or TIA, of whom 1339 were included in the current analysis of patients who had a ischaemic stroke with NIHSS 0–5 and mRS at 30 and 90 days (177 with TIA and 249 with missing mRS were excluded). Participants who were missing one or two mRS assessments were not different in relation to stroke severity, but tended to be younger than participants who had both mRS documented (p<0.05). Out of 1461 participants with 30-day mRS, 122 were missing 90-day mRS. Among the patients with 30-day mRS, the 30-day mRS value was not a predictor of having the 90-day mRS missing (p=0.61) in logistic regression models adjusting for age and NIHSS at admission.
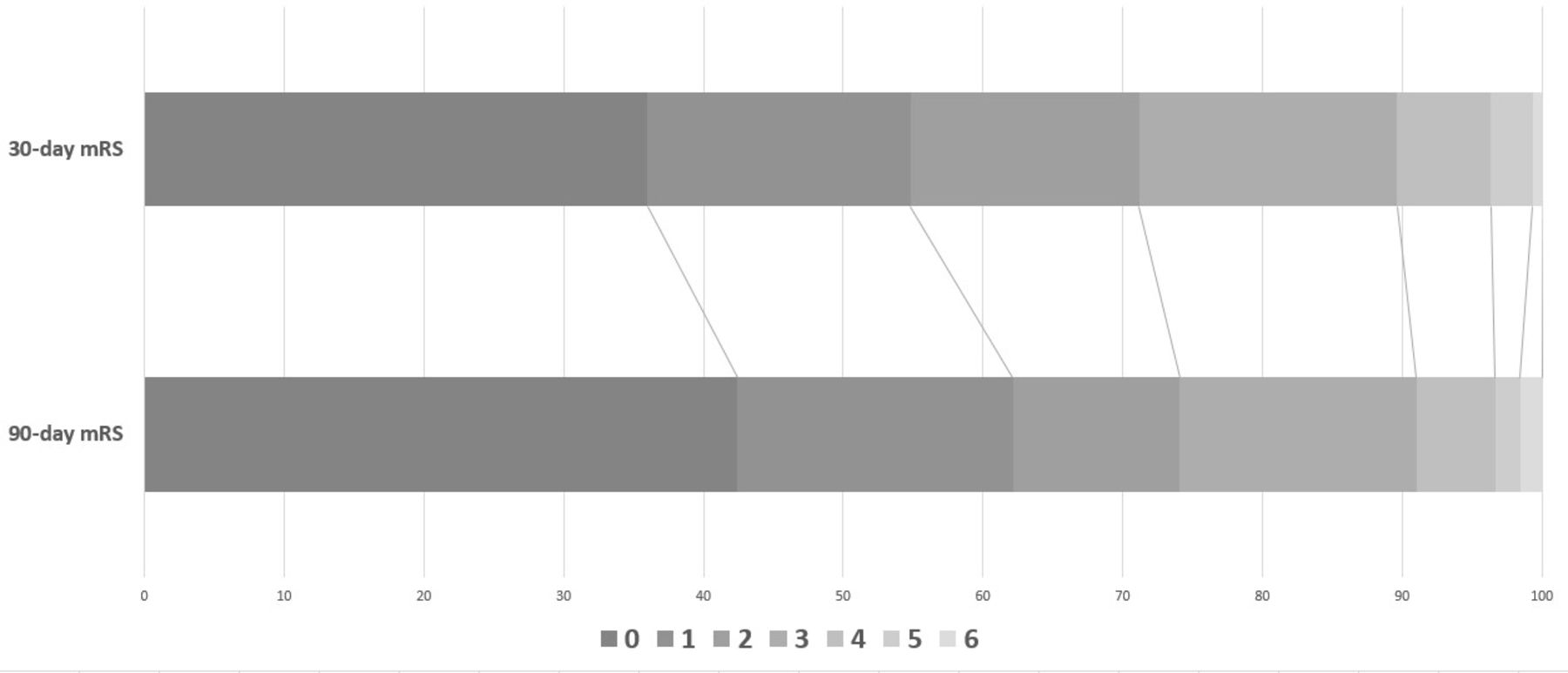
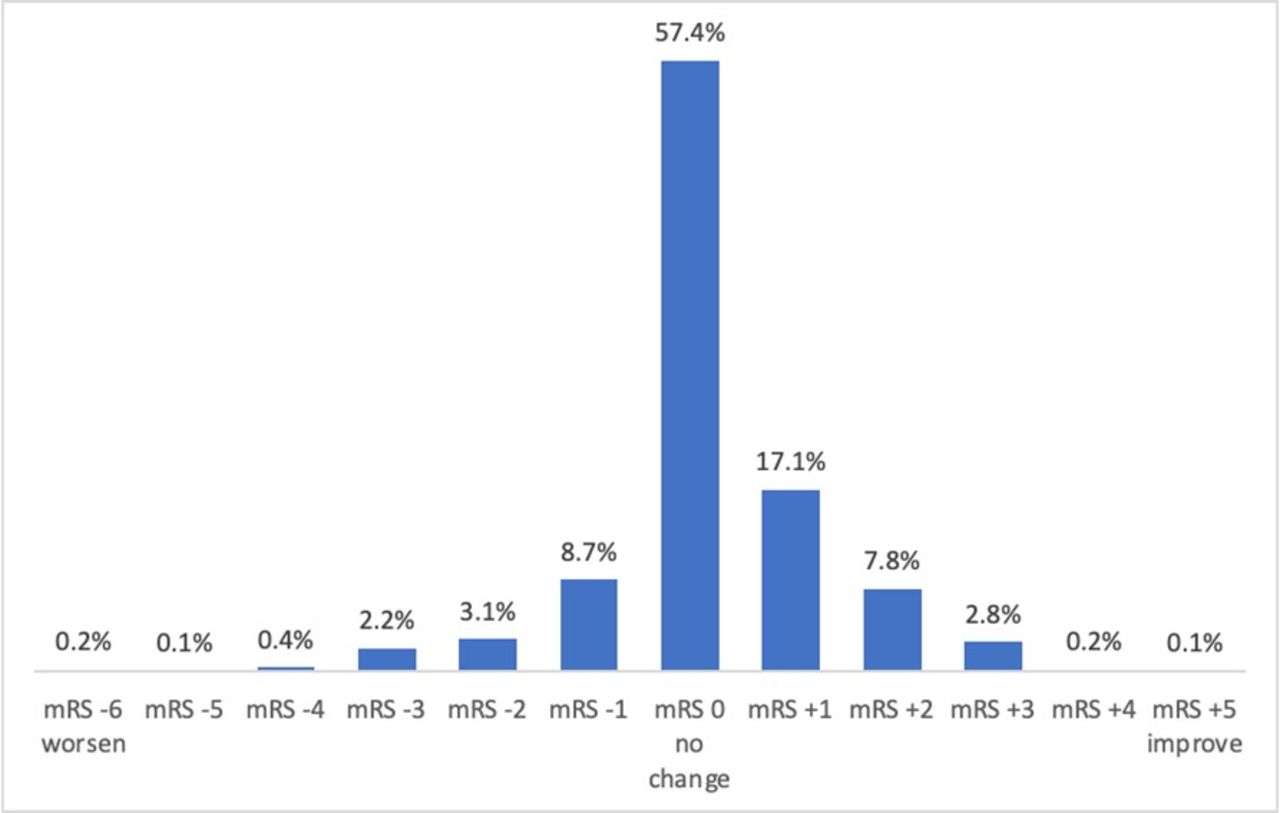
The distribution of the mRS at 30 days and 90 days, and the difference from 30 to 90 days is shown in figure 1 and online supplemental table 2. Fifty-seven per cent of study participants had the same mRS value at 30 and 90 days, while 17% improved by 1 point, and 9% declined by 1 point (1.6% starting at mRS=1). A weighted kappa of 0.59 (95% CI 0.56 to 0.62) suggested moderate agreement between the scores at the two time points. Figure 2 shows the distribution of mRS at 30 and 90 days.
Supplemental material
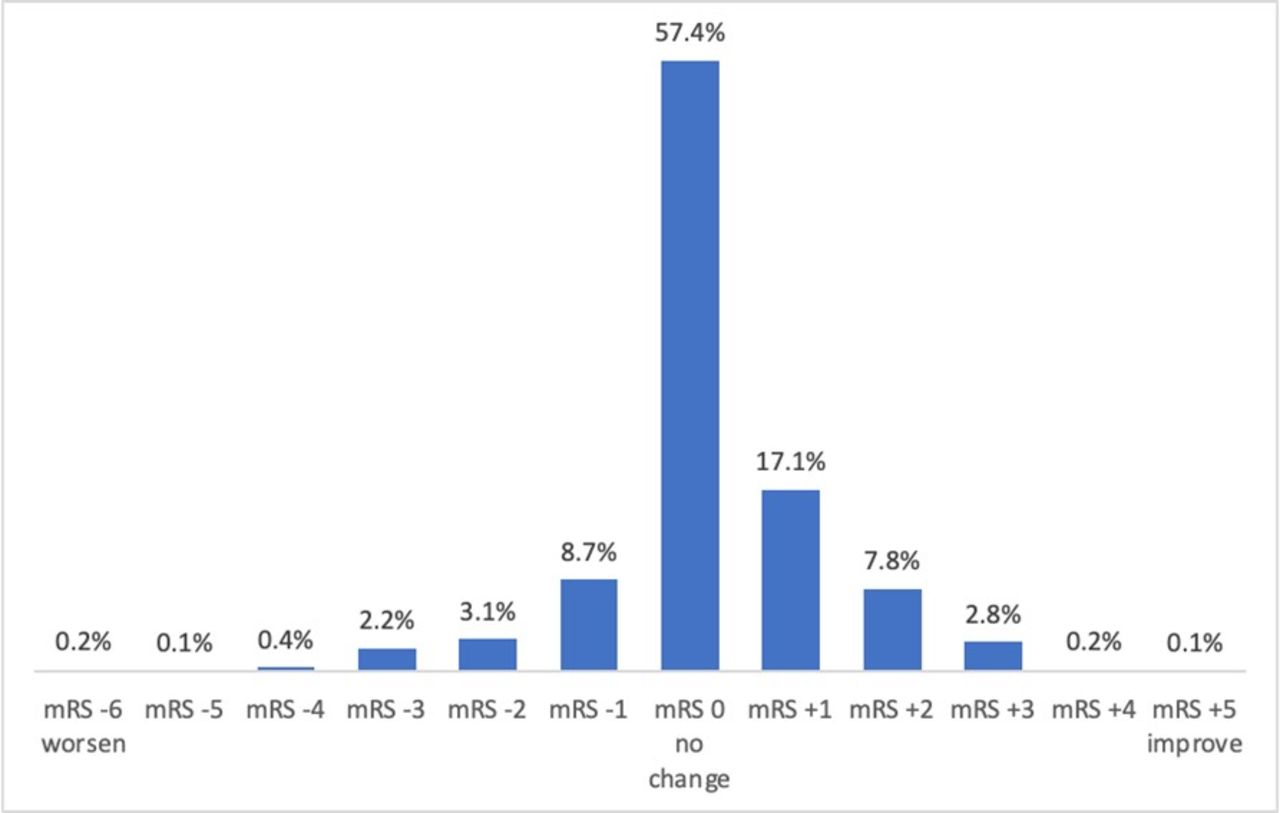
Change in modified Rankin Scale (mRS) between 30 and 90 days.
{kind=link}
{kind=link}
Distribution of modified Rankin Scale (mRS) at 30 and 90 days poststroke (%).
Employing the more parsimonious definitions of worsening and improvement between 30 and 90 days defined for this analysis (worsening: increase mRS >2 or change from 1 to 2; improvement: change from mRS >1 to 0–1 or change from mRS >2 to 0–2), we observed worsening in 7.54% (n=101) and improvement in 17.33% (n=232). As shown in online supplemental table 2, there were 10 additional participants who improved by more than 1 point but never achieved an mRS of 0–2 at 90 days. All of these participants improved from an mRS=5 to an mRS=3, which can also represent important clinical improvement, but was not included in the more parsimonious definition used in this study.
Table 1 shows the distribution of the patient and clinical characteristics in the full study population, and stratified by mRS worsening and improvement. In these analyses, patients with clinically insignificant worsening or improvement (ie, those that did not meet the definitions of worsening or improvement indicated above but did not have the exact same mRS at 30 and 90 days) were still included, as part of the ‘did not worsen’ or ‘did not improve’ categories, respectively.
Description of the study population by change in functional status
In univariate analyses the following variables were associated with mRS worsening from 30 to 90 days (p<0.05): older age, cardioembolic stroke mechanism, AF and no alteplase treatment. These variables remained significant after adjusting for age and NIHSS at hospital admission (table 2). After mutual adjustment in the final multivariable model, AF was no longer a significant predictor of decline, while increased stroke severity was associated with decline.
Predictors of decline between 30 and 90 days
In univariate analyses, the following variables were associated with mRS improvement from 30 to 90 days (p<0.05): private arrival mode, no hypertension, no dyslipidaemia, no previous CAD or MI. No hypertension, no dyslipidaemia and no previous CAD or MI all remained significant predictors after adjusted for age and NIHSS, but their associations were attenuated after mutual adjustment (table 3).
Predictors of improvement between 30 and 90 days
Discussion
In this study of patients who had a mild ischaemic stroke treated at select GWTG-Stroke hospitals across the USA, we examined whether an mRS assessment at 30 days may be an adequate representation of long-term disability at 90 days. It is widely accepted that an accurate prognosis of recovery after stroke can be made by 90 days from stroke onset,5 and an mRS assessment at 90 days is common in clinical trials. It has been previously suggested that the mRS at 30 days is similar to that at 90 days2; in that study the mRS at 30 days after discharge did not differ in approximately 50% of patients at 90 days, and those who showed functional change over time were more likely to worsen than improve. However, data on mild strokes are limited and the course of recovery may differ from more severe strokes. While mild stroke symptoms may improve faster, it is also possible that small insults allow surrounding brain tissue to engage in more vigorous neuroplasticity and recovery,6 underscoring the need to examine the functional trajectory from 30 to 90 days specifically in a large sample of mild strokes.
The results of the current study align with previous data suggesting consistency in function at 30 and 90 days poststroke from a statistical standpoint, but from a clinical perspective there was a high proportion of participants that had functional changes between 30 and 90 days. Specifically, with our conservative definition of mRS change, we found that a quarter of all study participants exhibited functional changes between 30 and 90 days, with 8% declining and 17% improving. For these patients the 30-day outcome was not representative of long-term recovery and a longer follow-up was clinically necessary. The potential causes of functional decline between 30 and 90 days in almost 8% of this population are many, such as stroke recurrence or other vascular events and depression. However, the MaRISS study did not collect the data needed to better understand interim clinical conditions that may have contributed to functional decline.
The 17% probability of significant improvement between 30 and 90 days in this mild stroke population supports the hypothesis that a mild stroke may result in greater opportunity for longer-term functional improvement compared with a major stroke that may be so debilitating that the prospect for improvement is diminished. The expected course of recovery for stroke, in general, depends on the severity of the initial stroke. Most patients who had a mild acute stroke are discharged home with none to mild neurological and functional disabilities after leaving the hospital, while most patients who had a severe stroke experience severe neurological and functional disability at discharge.7 Previous data suggest that approximately 80% of patients that suffered mild strokes reached their best neurological state within 2.5–6.5 weeks, while 80% of patients that suffered very severe strokes reached their best neurological state within 10–13 weeks.5 However, the current data supports the opportunity for continued improvement up to 90 days poststroke in low NIHSS stroke.
The results of this study also provided novel information about how to predict patients that might be more likely to improve or decline between 30 and 90 days, which can help investigators and medical professionals target specific patients for whom an additional 90-day assessment may be important. Patients with AF were more likely to decline between 30 and 90 days, even after accounting for age and stroke severity, while alteplase treatment was associated with a decreased risk of decline. AF is recognised as a strong predictor of recurrent stroke, and patients with AF not treated with anticoagulants have been shown to have a twofold increased risk of stroke recurrence.8 It is possible that patients with a recent stroke are not anticoagulated at discharge.9 However, the MaRISS study did not collect data on medication prescription and adherence at 90-days post-discharge. As expected, increasing age and stroke severity were also independent predictors of decline. In contrast the results suggested that patients with prior CAD or MI, hypertension and dyslipidaemia were less likely to improve between 30 and 90 days but none of these variables remained independent predictors after mutual adjustment.
We have previously shown in MaRISS that patients treated with alteplase were more likely to experience early improvement in the NIHSS, but we did not identify an association of alteplase with 90-day outcome between patients who were treated and untreated in this observational study, except for patients with NIHSS in the 3–5 range: those who received alteplase treatment performed better on the Stroke Impact Scale-16 at 90 days.10 The current study adds to the observations regarding potential modest benefits of alteplase treatment in patients with mild stroke, as treated participants were also less likely to decline on the mRS from 30 to 90 days, controlling for age and stroke severity. In MaRISS, a very small number had thrombectomy and therefore we could not assess its effect on outcomes. A recent multicentre study and meta-analysis did not find a clear benefit of thrombectomy over best medical management in patients with low NIHSS,11 but there are ongoing thrombectomy trials in this population.
Important strengths of the current study were the focus on mild strokes with a broad range of important clinical characteristics collected prospectively at the time of hospital admission, the collection of repeated mRS assessments by trained study personnel, the use of the mRS-9Q V.4 to reduce interobserver variability, and the minimal lost to follow-up. Potential selection bias in relation to alteplase treatment is important to note, as MaRISS included a very large proportion of alteplase treated patients (57%), higher than that reported in other large US-based studies of mild strokes.12 It is also important to note that excluded participants without mRS at both 30 and 90 days tended to be slightly younger and therefore possibly less likely to worsen. However, it was reassuring to observe that the 30-day mRS performance was unrelated to missingness of 90-day mRS. Finally, we did not collect information about access and intensity of rehabilitation after hospital discharge, medication adherence, lifestyle modifications, social support, nor stroke recurrence and readmission that could clarify the influential factors for deterioration or improvement after day 30. Future studies are needed to better understand and ultimately prevent the clinical circumstances associated with significant long-term decline after stroke in this mild patient population.
In conclusion, the use of a 30-day outcome assessment would improve clinical study participant attrition and expedience of results, possibly decrease costs and provide an earlier indicator of long-term functional prognosis. However, we found that the 30-day mRS is not a valid predictor of delayed outcomes for a quarter of the mild stroke population, indicating that a 90-day outcome measure should remain the standard practice in clinical studies of patients who had a mild stroke.
Data availability statement
Data may be obtained from a third party and are not publicly available. The authors are not authorised to make the data publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Miami IRB information:University of Miami IRB (FWA00002247)ePROST # 20120079 Initial UMIRB, approval issued on 16 March 2013.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @braindoc_mgh
Contributors HG: conception and design of the work, data analysis and interpretation, drafting the article, final approval of the version to be published. LAR: literature review, drafting the article, final approval of the version to be published. EES: data collection, data interpretation, critical revision of the article, final approval of the version to be published. IC-B: conception and design of the work, data collection, critical revision of the article, final approval of the version to be published. YK: data collection, critical revision of the article, final approval of the version to be published. ST: data collection, critical revision of the article, final approval of the version to be published. NR: data collection, critical revision of the article, final approval of the version to be published. RLS: critical revision of the article, final approval of the version to be published. PK: critical revision of the article, final approval of the version to be published. HMA: critical revision of the article, final approval of the version to be published. BMG: critical revision of the article, final approval of the version to be published. DG: critical revision of the article, final approval of the version to be published. NSS: critical revision of the article, final approval of the version to be published. KEO: critical revision of the article, final approval of the version to be published. CGB: critical revision of the article, final approval of the version to be published. AGK: critical revision of the article, final approval of the version to be published. SSB: critical revision of the article, final approval of the version to be published. ACK: critical revision of the article, final approval of the version to be published. LHS: data collection, data interpretation, critical revision of the article, Final approval of the version to be published. JGR: conception and design of the work, data analysis and interpretation, critical revision of the article, final approval of the version to be published. HG is responsible for the overall content as the guarantor.
Funding The study was supported by a grant from Genentech, Inc. (South San Francisco, CA; NCT 02072681); Genentech did not play a role in the design or data analysis. The study is registered in ClinicalTrials.gov (NCT 02072681). The Get With The Guidelines®–Stroke (GWTG-Stroke) programme is provided by the American Heart Association/American Stroke Association.
Competing interests JGR: grant from Genentech to U Miami to support role as PI of MaRISS; personal fees from Genentech for role as a member of the steering committee for the PRISMS trial and member of the independent data monitoring committee of the TIMELESS Trial. HG: grant from Genentech to U Miami to support role as MaRISS Study Epidemiologist EE Smith: none I Campo-Bustillo: grant from Genentech to U Miami to support role as MaRISS Study Manager. YK: none S Tai: none N Riley: none. HMA: none. BMG: none. DG: none. NSS: none. KEO: none. CGB: none. AGK: none. SSB: none. ACK: none. RLS: grants from NIH grants (NINDS, NIMHD, NCATS), from the Florida Department of Health for the support of the Florida Stroke Registry, and fees from American Heart Association for work as Editor-in-Chief of Stroke. PK: funds to her institution from Genentech (PRISMS Trial National PI, HAMLET Steering Committee member), Diamedica (Scientific Advisory Board), Lumosa (Consultant and DSMB Representative), Nervive (NIH SBIR Co-Investigator) and Cerenovus (Investigator-Initiated ENDOLOW Trial MPI); fees from Bayer (PACIFIC-Stroke Trial National Leader). HMA: none. LHS: scientific consultant and steering committee member, TIMELESS Trial (Genentech); consultant (LifeImage); consultant on stroke systems of care, Massachusetts Department of Public Health; DSMB member, MIND Study (Penumbra) and PHAST-TSC Study (Diffusion Pharmaceutical); National PI, Stroke AF Study (Medtronic); National Co-PI, MR WITNESS Study (NINDS) (alteplase provided free of charge to Massachusetts General Hospital, supplemental per-patient payments sites by Genentech); Site PI, New England Regional Coordinating Center, StrokeNet (NINDS).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.