Article Text

Abstract
Background White matter hyperintensity (WMH) on brain MRI is associated with developing dementia or mild cognitive impairment (MCI), but WMH progression over time has not been fully investigated as an independent risk factor.
Methods We performed a post hoc analysis of the Systolic Blood Pressure Intervention Trial - Memory and Cognition in Decreased Hypertension (SPRINT MIND) trial. The primary outcome was incident probable dementia or MCI (dementia/MCI) before the follow-up MRI at 48 months from enrolment. The primary predictor was WMH progression, defined as the Z score difference between the follow-up and baseline WMH volumes. The secondary predictor was a binary WMH progression threshold (≥1.4 mL vs <1.4 mL).
Results Among the 433 included patients, 33 (7.6%) developed dementia/MCI. There were 156 (36.0%) patients who met the WMH progression threshold of ≥1.4 mL, in whom the rate of dementia/MCI was 12.8% (20/156) vs 4.7% (13/277) of patients with <1.4 mL WMH progression (p=0.002). In multivariable logistic regression, the Z score of WMH progression was associated with dementia/MCI (OR 1.51, 95% CI 1.12 to 2.04, p=0.007) as was the WMH progression threshold of ≥1.4 mL (OR 2.89, 95% CI 1.23 to 6.81, p=0.015).
Conclusions In this post hoc analysis of SPRINT MIND, WMH progression over 48 months was associated with the development of probable dementia or MCI.
- Brain
- Cognitive Dysfunction
- Magnetic Resonance Imaging
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject
The burden of white matter hyperintensity (WMH) on brain MRI is associated with future risk of developing dementia or mild cognitive impairment (MCI).
In the SPRINT MIND and Action to Control Cardiovascular Risk in Diabetes Memory in Diabetes (ACCORD MIND) trials, intensive blood pressure reduction resulted in less WMH progression over time.
However, WMH progression over time, as opposed to static burden, has not been fully investigated as an independent risk factor for the development of dementia/MCI.
What are the new findings
We performed a post hoc analysis of the SPRINT MIND trial. Among the 433 included patients, 33 (7.6%) developed dementia/MCI during follow-up.
There were 156 (36.0%) patients who met the WMH progression threshold of ≥1.4 mL, in whom the rate of dementia/MCI was 12.8% (20/156) vs 4.7% (13/277) of patients with <1.4 mL WMH progression (p=0.002).
In multivariable logistic regression, the Z score of WMH progression was associated with dementia/MCI (OR 1.51, 95% CI 1.12 to 2.04, p=0.007) as was the WMH progression threshold of ≥1.4 mL (OR 2.89, 95% CI 1.23 to 6.81, p=0.015)
How might it impact on clinical practice in the foreseeable future?
In this post hoc analysis of SPRINT MIND, WMH progression over 48 months was associated with the development of probable dementia or MCI. Because intensive blood pressure control reduces the progression of WMH, additional research is needed to test interventions that reduce WMH progression.
Introduction
The burden of white matter hyperintensity (WMH) on brain MRI is associated with future risk of developing dementia or mild cognitive impairment (MCI).1 2 In the SPRINT MIND and ACCORD MIND trials, intensive blood pressure reduction resulted in less WMH progression over time.3 4 However, WMH progression over time, as opposed to static burden, has not been fully investigated as an independent risk factor for the development of dementia/MCI.5
Methods
To assess the hypothesis that increased WMH progression is associated with incident dementia/MCI, we evaluated patients enrolled in SPRINT MIND who had a baseline and 48-month follow-up MRI. We conformed to Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cohort studies.6 The primary outcome of our analysis was incident probable dementia or MCI (dementia/MCI) before the follow-up MRI. The rigorous adjudication of dementia/MCI in SPRINT MIND has previously been described.7 We excluded 14 patients who were lost to follow-up more than 90 days before the follow-up MRI. The primary predictor was WMH progression, defined as the difference in millilitres between the follow-up and baseline WMH volumes, which was transformed to a Z score for standardisation.3 The secondary predictor was a binary WMH progression threshold, which was a concordance probability derived cutpoint of WMH progression (≥1.4 mL vs <1.4 mL, area under the receiver operating curve=0.64). We fit logistic regression models to dementia/MCI, with the predictor of WMH progression standardised as a Z score and a priori adjusted for baseline WMH volume and total intracranial volume. With stepwise backwards selection set at a p value of <0.1, we selected additional covariates from table 1, including patient race, retirement status and randomisation arm. As a sensitivity analysis, we adjusted for baseline WMH volume, total intracranial volume, patient age, race, sex, education and randomisation arm.
Baseline demographics and MRI volumes, stratified by the WMH progression threshold of ≥1.4 mL vs <1.4 mL
Results
The baseline demographics and their association with WMH progression are shown in table 1.
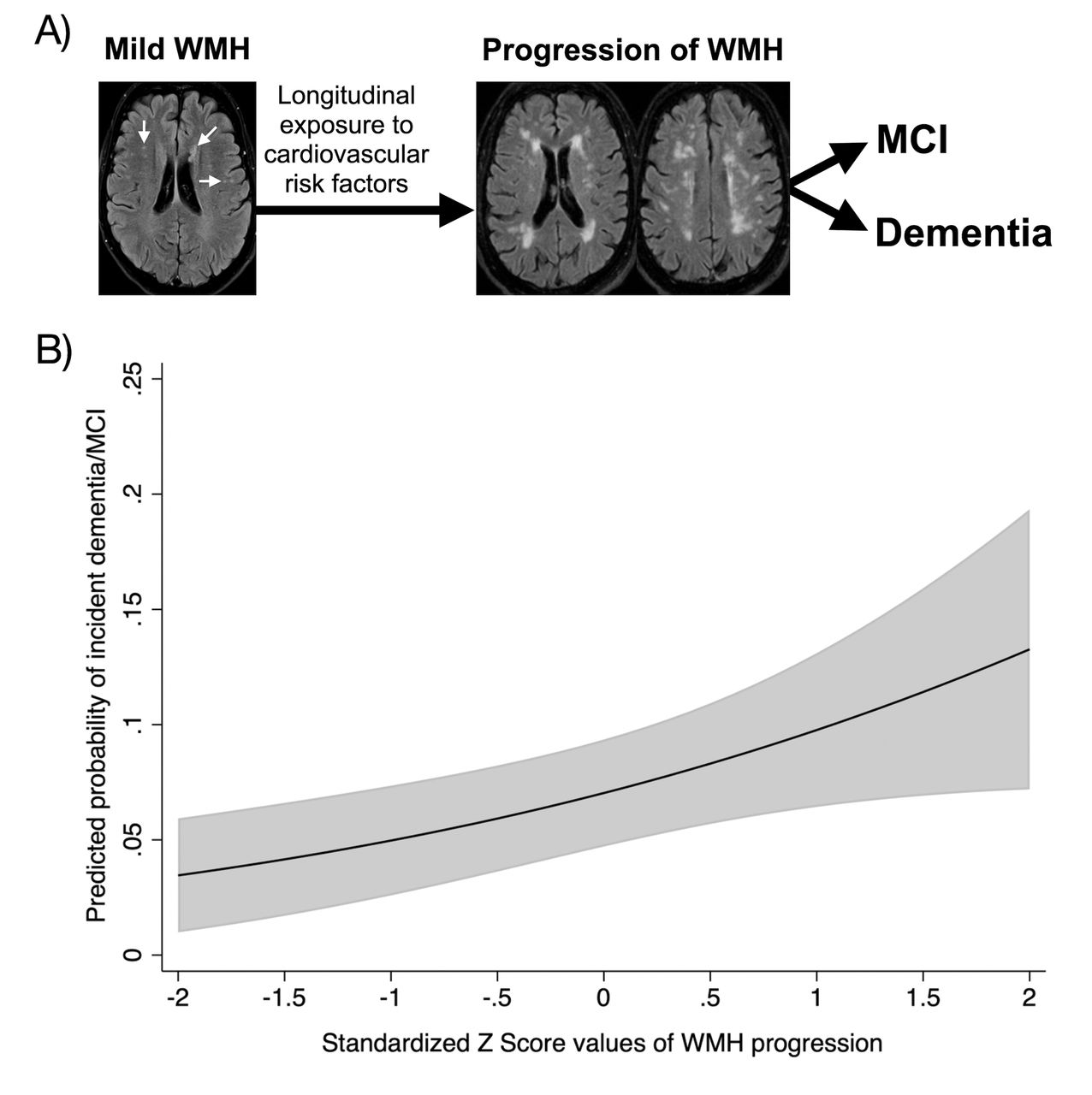
Among the 433 included patients, 33 (7.6%) developed dementia/MCI by the follow-up MRI. The mean WMH progression was 1.7±3.4 mL, and those in patients with dementia/MCI versus those without were 4.0±5.8 vs 1.5±3.0 mL (p<0.001). There were 156 (36.0%) patients who met the WMH progression threshold of ≥1.4 mL, in whom the rate of dementia/MCI was 12.8% (20/156) vs 4.7% (13/277) of patients with WMH progression of <1.4 mL (p=0.002). In the multivariable logistic regression model, the standardised Z score of WMH progression was associated with dementia/MCI (OR 1.51, 95% CI 1.12 to 2.04, p=0.007) as was the WMH progression threshold of ≥1.4 mL (OR 2.89, 95% CI 1.23 to 6.81, p=0.015). These associations remained significant in the sensitivity analyses (respective ORs 1.43 and 2.62, p=0.020 and 0.030). The predicted probability of incident dementia/MCI across ±2 Z scores of WMH progression is shown in figure 1.

{kind=link}
(A) An example of the pathway between WMH progression on MRI and dementia/MCI, (B) predicted probability* of incident dementia/MCI for ±2 Z scores of WMH progression. *Adjusted for baseline WMH volume, total intracranial volume, patient race, retirement status and randomisation arm. MCI, mild cognitive impairment; WMH, white matter hyperintensity.
Discussion
In this post hoc analysis of SPRINT MIND, the WMH progression over 48 months was associated with the development of probable dementia or MCI, independent of the baseline WMH volume. While these results are concordant with prior research showing that a high burden of baseline WMH volume is associated with worse cognitive function,5 the extension of that finding to WMH progression over time is important for two reasons. First, SPRINT MIND showed that intensive blood pressure reduction (target systolic <120 mm Hg) resulted in a 0.58 mL reduction in WMH progression,3 suggesting that the potentially harmful effects of WMH progression could be mitigated. A key limitation to our analysis is that we were not able to control for all potential confounders, such as the Apolipoprotein E (APOE) genotype. Unfortunately, the current subgroup analysis does not allow investigation of the interaction between intensive blood pressure reduction and WMH progression on the risk of dementia/MCI due to a high potential for subgroup selection bias. Second, besides blood pressure reduction, there are other interventions with plausible beneficial effect on WMH progression including lipid lowering, antiplatelet therapy and optimisation of other vascular risk factors.8 The findings in this analysis provide further support for the study of novel approaches to reduce WMH progression as a potential treatment to prevent dementia/MCI.
Ethics statements
Patient consent for publication
Ethics approval
Institutional review board approval was not required for the deidentified dataset, which is publicly available.
Footnotes
Contributors AdH, KNS, SDY, TNT and SP all made substantial contributions to the conception or design of the work, drafting the work or revising it critically for important intellectual content, gave the final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AdH has investigator-initiated research support from Regeneron, AMGEN and AMAG pharmaceuticals; KNS reports funding from Biogen, Novartis, Bard, Hyperfine, Astrocyte and Alva Health.
Provenance and peer review Not commissioned; externally peer reviewed.