Article Text

Abstract
Background and purpose Dyslipidaemia is a major risk factor for ischaemic stroke and transient ischaemic attack (TIA). This study aimed to investigate the association between baseline low-density lipoprotein cholesterol (LDL-C) level, lipid-lowering treatment and short-term risk of new stroke in patients with a minor ischaemic stroke or TIA.
Methods We derived data from the Clopidogrel in High-risk patients with Acute Non-disabling Cerebrovascular Events trial. Patients with a minor stroke or TIA were categorised by LDL-C level at baseline (<2.6 or ≥2.6 mmol/L (100 mg/dL)) and with or without lipid-lowering treatment after symptom onset. The primary outcome was a new ischaemic stroke at 3 months. The association of baseline LDL-C level, lowering treatment and outcomes were assessed.
Results Among 3027 patients, 2154 (71.2%) patients had an initial LDL-C ≥2.6 mmol/L, of which 1267 (41.9%) received lipid-lowering treatment. Elevated LDL-C level was associated with a higher risk of new ischaemic stroke at 3 months in patients without lipid-lowering treatment (adj.HR=1.35, 95% CI: 1.19 to 1.53), but not in those with lipid-lowering treatment (adj.HR=0.99, 95% CI: 0.82 to 1.19) (p for interaction=0.007). Patients with LDL-C ≥2.6 mmol/L had a numerically higher risk of ischaemic stroke (11.8% vs 8.0%, adj.HR=1.37, 95% CI: 0.96 to 1.96) in those without lipid-lowering treatment. For patients with LDL-C ≥2.6 mmol/L, lipid-lowering treatment was associated with reduced risk of ischaemic stroke at 3 months (7.9% vs 11.8%; adj.HR=0.54, 95% CI: 0.39 to 0.75).
Conclusions Elevated untreated baseline LDL-C level was associated with an increased short-term risk of ischaemic stroke among patients presenting with minor ischaemic stroke or TIA. There was potential benefit of lipid-lowering treatment in minor stroke or TIA patients with LDL-C ≥2.6 mmol/L.
Trial registration number NCT00979589.
- stroke
- cerebrovascular disorders
Data availability statement
Data are available on reasonable request. Data are available to researchers on request for purposes of reproducing the results or replicating the procedure by directly contacting the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Dyslipidaemia is a major risk factor for atherosclerotic cardiovascular disease and reduction of low-density lipoprotein cholesterol (LDL-C) level is the major therapeutic target in clinical practice.1–3 Numerous previous epidemiological studies and randomised trials have established the association of elevated LDL-C level with risk of poor outcome in the setting of cardiovascular diseases.4–6 Whereas, previous studies on stroke mainly focused on the association of LDL-C and risk of ischaemic stroke in the primary prevention setting.7 8 In the secondary prevention setting, the previous SPARCL trial (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) and the recent TST trial (Treat Stroke to Target) demonstrated that lowering LDL-C level by statin treatment reduced long-term recurrent events in patients with ischaemic stroke.9 10 However, few studies described the pattern and magnitude of the association between LDL-C level, lipid-lowering treatment and the short-term prognosis of minor stroke and transient ischaemic attack (TIA) in real world clinical setting. Therefore, the pattern and magnitude of association between baseline LDL-C level, lipid-lowering treatment and short-term outcome of minor stroke and TIA should be further examined.
This study, thus, aimed to evaluate the pattern and magnitude of association between baseline LDL-C level, lipid-lowering treatment and short-term prognosis of patients with acute minor ischaemic stroke or TIA.
Methods
Study design and patients
Data were derived from the Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events (CHANCE) trial. Design and primary results of the CHANCE trial have been published elsewhere.11 12 Briefly, CHANCE was a prospective multicentre double-blind randomised placebo-controlled trial conducted at 114 centres in China between 1 October 2009 and 30 July 2012. The trial compared dual therapy of clopidogrel plus aspirin (a loading dose of 300 mg, followed by 75 mg/day clopidogrel for 90 days; plus 75 mg/day aspirin for the first 21 days) vs placebo plus aspirin (75 mg/day for 90 days) in 5170 patients within 24 hours after the onset of non-cardioembolic minor ischaemic stroke (defined as a score of ≤3 on the National Institutes of Health Stroke Scale (NIHSS)) or high-risk TIA (defined as a score of ≥4 on the ABCD,2 which assesses the risk of stroke according to age, blood pressure, clinical features, duration of TIA and presence or absence of diabetes). Clinical follow-up was obtained in the first 90 days from randomisation. All the participants or their legal proxies provided written informed consent prior to enrolment.
Among 144 clinical centres included in CHANCE, 73 centres voluntarily participated in the prespecified blood biomarker substudy. All the patients at these centres participated in this biomarker substudy. The biomarker substudy has been described elsewhere.13 Patients participating in the biomarker substudy provided a separate written informed consent form including consent for blood sample collection and further study of biomarkers.
Data collection and measurement of LDL-C level
Baseline characteristics on demographics, history of ischaemic stroke, TIA, myocardial infarction, angina, congestive heart disease, atrial fibrillation, valvular heart disease, hypertension, diabetes mellitus, hypercholesterolaemia, smoking status and medication use during hospitalisation and after discharge were collected through face-to-face interviews by trained interviewers (neurologists from participating centres). Patients with any record of antihypertensive, antidiabetic and antihyperlipidaemic therapy during hospitalisation and after discharge were considered along with corresponding treatment.
Venous blood samples were collected from fasting patients within 24 hours from admission. Serum specimens were extracted, aliquoted and transported through cold chain to the centre laboratory in XXX Hospital and stored at −80℃. LDL-C measurements were centrally and blindly assayed by enzymatic method on the Cobas 8000 analyzer c702 module (Roche Diagnostics, Mannheim, Germany). Due to low sample size in patients with LDL-C <1.8 mmol/L (70 mg/dL) and the fact that lipid-lowering treatment for patients who hd a stroke with LDL-C <2.6 mmol/L (100 mg/dL) was not recommended before 2016 in the Chinese guidelines for the prevention and treatment of adult dyslipidaemia,14 patients were categorised as four groups according to baseline LDL-C levels and lipid-lowering treatment during hospitalisation and after discharge: LDL-C <2.6 mmol/L without lipid-lowering treatment, LDL-C <2.6 mmol/L with lipid-lowering treatment, LDL-C ≥2.6 mmol/L without lipid-lowering treatment and LDL-C ≥2.6 mmol/L with lipid-lowering treatment.
Clinical outcomes
The primary efficacy outcome was a new ischaemic stroke within 3 months following randomisation. The secondary efficacy outcomes included a new stroke (ischaemic or haemorrhagic) and a new composite vascular event (stroke, myocardial infarction or vascular death) at 3 months. The primary safety outcome was any bleeding at 3 months. All the definitions of outcomes in this study were same as those in the parent trial.12 All reported efficacy and safety outcomes were verified by a central independent adjudication committee that was blinded to study treatment assignments and baseline LDL-C level.
Statistical analysis
Continuous variables of baseline characteristics were presented as medians with IQRs and categorical variables as frequencies and percentages. The baseline variables between patients included in and excluded from this analysis and among different LDL-C/lipid-lowering treatment groups were compared using the non-parametric Wilcoxon rank-sum test or Kruskal-Wallis test as appropriate for continuous variables, and chi-square test for categorical variables.
We presented the time to the first new ischaemic stroke using Kaplan-Meier curves (1—proportion free of event). Multivariable Cox proportional-hazards regression models with study centre as a random effect were used to evaluate the association of LDL-C level, different LDL-C/lipid-lowering treatment groups and the risk of new ischaemic stroke, composite vascular event, stroke, and any bleeding at 3 months. Adjusted HRs with their 95% CIs are reported. We adjusted for all other potential covariates listed in table 1 in the multivariable models. Interactions between antiplatelet treatment assignment and LDL-C level, between antiplatelet treatment assignment and lipid-lowering treatment and between LDL-C level and lipid-lowering treatment were tested by including terms of antiplatelet treatment, LDL-C level, lipid-lowering treatment, antiplatelet treatment-by-LDL-C level interaction, antiplatelet treatment-by-lipid-lowering treatment interaction and LDL-C level-by-lipid-lowering treatment interaction in the Cox models. The proportional-hazards assumption was assessed by testing a time-dependent covariate with a logarithmic function of survival time-by-LDL-C/lipid-lowering treatment interaction in the model.
Baseline characteristics of the patients included in and excluded from this analysis
The association of lipid-lowering treatment with the short-term prognosis of stroke is of great concern given the high prevalence of dyslipidaemia in patients who had a stroke. To further compare the outcomes of patients with and without lipid-lowering treatment when with LDL-C <2.6 mmol/L or LDL-C ≥2.6 mmol/L, a propensity score matching method was developed as a sensitivity analysis, respectively. A propensity score, indicating the predicted probability of receiving lipid-lowering treatment, was calculated using a non-parsimonious multivariable logistic regression model including all baseline variables. We performed a 1:1 matching based on the nearest-neighbour matching algorithm with a calliper width of 0.1 of the propensity score.15 We then compared the outcomes of patient with and without lipid-lowering treatment with Cox proportional-hazards regression models using the propensity score matching sample.
To evaluated the pattern and magnitude of associations between LDL-C level and risk of new ischaemic stroke, we used a multivariable Cox regression model with restricted cubic spline for LDL-C level. The LDL-C level of 2.6 mmol/L was treated as the reference and the 5th, 25th, 50th, 75th, 95th percentiles of LDL-C level was treated as the five knots for spline. Separate analyses were performed for patients with LDL-C <2.6 mmol/L, LDL-C ≥2.6 mmol/L without lipid-lowering treatment and LDL-C ≥2.6 mmol/L with lipid-lowering treatment.
Anonymised data are available to researchers for reproducing the results by contacting the corresponding author. Two-sided p<0.05 were considered to be statistically significant. All analyses were considered exploratory and adjustments were not made for multiplicity. All analyses were conducted with SAS software V.9.4 (SAS Institute).
Results
Study participants
A total of 3044 consecutive patients participated in the biomarker substudy. After excluding 17 patients with missing data of lipid-lowering treatment, a total of 3027 patients were included in the present analysis. Among those included, the median age was 62.3 years old, 66.6% were males, 2215 (73.2%) had an index event of minor stroke and 812 (26.8%) had a TIA. Table 1 shows the baseline characteristics of patients included in and excluded from this analysis. The patients included in and excluded from this analysis were well-balanced except for a slightly lower proportion of angina, diabetes mellitus, hypercholesterolaemia and qualifying TIA in patients enrolled, higher NIHSS score on admission and higher proportion of antihypertensive therapy during hospitalisation and after discharge in the included population.
Among the 3027 patients, there were 210 (6.9%), 663 (21.9%), 959 (31.7%), 630 (20.8%) and 565 (18.7%) patients with an LDL-C <1.8 mmol/L, LDL-C 1.8–2.5 mmol/L, LDL-C 2.6–3.3 mmol/L, LDL-C 3.4–4.0 mmol/L, LDL-C ≥4.1 mmol/L, respectively. There were 513 (16.9%), 360 (11.9%), 1247 (41.2%) and 907 (30.0%) patients had an LDL-C <2.6 mmol/L without lipid-lowering treatment, LDL-C <2.6 mmol/L with lipid-lowering treatment, LDL-C ≥2.6 mmol/L without lipid-lowering treatment and LDL-C ≥2.6 mmol/L with lipid-lowering treatment, respectively. The baseline characteristics of patients by LDL-C level and lipid-lowering treatment during hospitalisation and after discharge are showed in tables 2 and 3.
Baseline characteristics of the patients by LDL-C level and lipid-lowering treatment in the entire cohort
Baseline characteristics of the patients by LDL-C level and lipid-lowering treatment in the propensity score matching cohorts
Association of LDL-C level and lipid-lowering treatment with risk of stroke
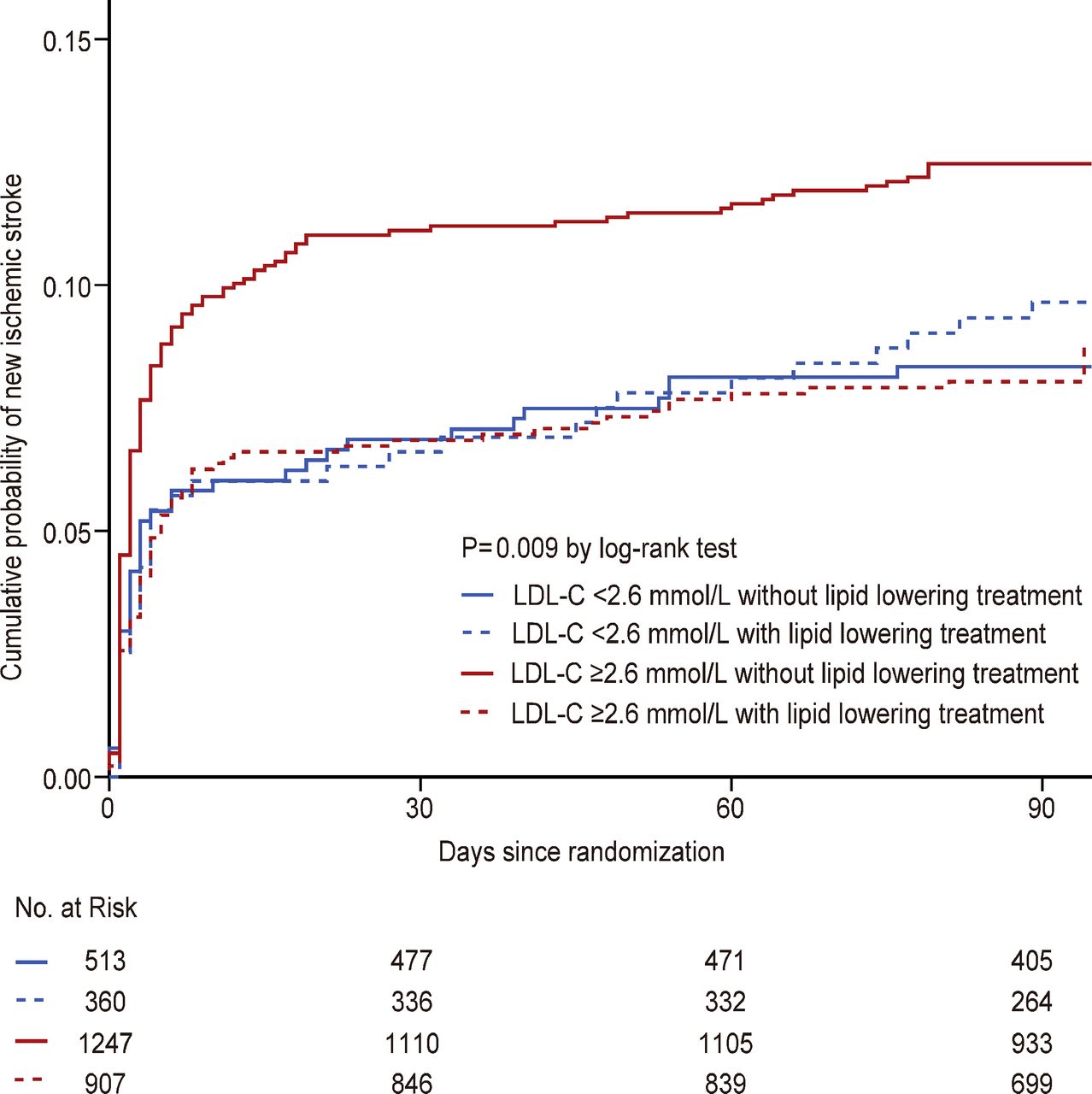
There were 299 (9.8%) new stroke occurrences at 3 months, of which 293 (98.0%) were ischaemic stroke and 6 (2.0%) were haemorrhagic stroke. No significant interactions were observed between antiplatelet treatment assignment and LDL-C level or lipid-lowering treatment (p for interaction=0.19 and 0.64 in the adjusted model). Higher baseline LDL-C level was associated with an increased risk of ischaemic stroke in patients without lipid-lowering treatment (adj.HR=1.35, 95% CI: 1.19 to 1.53, p<0.001), but not in those with lipid-lowering treatment (adj.HR=0.99, 95% CI: 0.82 to 1.19, p=0.91) (p for interaction=0.007 in the adjusted model). Compared with patients with LDL-C <2.6 mmol/L without lipid-lowering treatment, patients with LDL-C ≥2.6 mmol/L without lipid-lowering treatment had a numerically higher risk of ischaemic stroke at 3 months (11.8% vs 8.0%, adj.HR=1.37, 95% CI: 0.96 to 1.96, p=0.09) (table 4, figure 1); whereas, those with LDL-C ≥2.6 mmol/L with lipid-lowering treatment had similar risk of ischaemic stroke at 3 months as those with LDL-C <2.6 mmol/L without lipid-lowering treatment (7.9% vs 8.0%, p=0.16). The proportional hazard assumption was met (p=0.57). For patients with LDL-C ≥2.6 mmol/L, lipid-lowering treatment was associated with reduced risk of ischaemic stroke at 3 months both in multivariable model (7.9% vs 11.8%; adj.HR=0.54, 95% CI: 0.39 to 0.75, p<0.001) and in the propensity score matching model (7.7% vs 12.5%; adj.HR=0.60, 95% CI: 0.44 to 0.81, p=0.001); whereas, for patients with LDL-C <2.6 mmol/L, lipid-lowering treatment was not associated with reduced risk of ischaemic stroke at 3 months both in multivariable model (p=0.68) and in the propensity score matching model (p=0.81). Similar results were found for the outcome of stroke and composite vascular events (table 4). Compared with those without lipid-lowering treatment, lower risk of any bleeding was observed in patients with LDL-C ≥2.6 mmol/L with lipid-lowering treatment in multivariable adjustment model but not in propensity score matching model.
Risk of stroke at 3 months after a minor stroke or TIA according to LDL-C level and lipid-lowering treatment

Risk of ischaemic stroke for patients with different level of LDL-C and lipid-lowering treatment. LDL-C, low-density lipoprotein cholesterol.
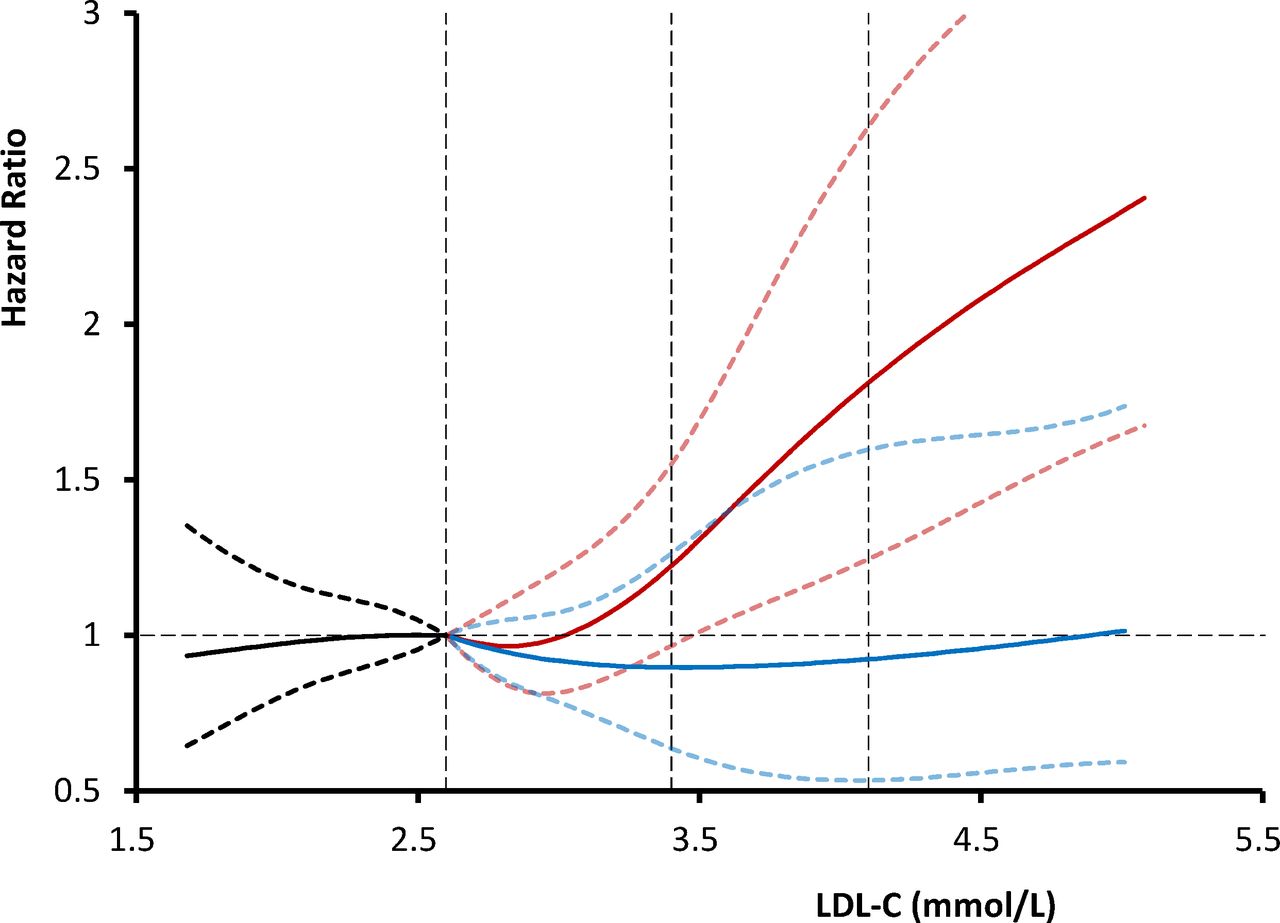
Using a Cox regression model with restricted cubic spline, we found the risk of new ischaemic stroke increased with the increase of LDL-C level for patients with LDL-C level ≥2.6 mmol/L but without lipid-lowering treatment (figure 2). However, this trend was not found for those with LDL-C level ≥2.6 mmol/L and lipid-lowering treatment, and the risk of new ischaemic stroke for these patients was similar as those with LDL-C level <2.6 mmol/L.

{kind=link}
{kind=link}
Adjusted HRs of recurrent ischaemic stroke according to LDL-C level and lipid-lowering treatment. the red line indicates estimated HR of recurrent ischaemic stroke in patients without lipid-lowering treatment when LDL-C level ≥2.6 mmol/L, whereas the blue line indicates those with lipid-lowering treatment when LDL-C level ≥2.6 mmol/L, and the dark line indicates those with LDL-C level <2.6 mmol/L. The solid line indicates the estimated HR and the dashed lines the 95% CI. Reference is LDL-C level of 2.6 mmol/L. Data were fitted using a multivariable Cox regression model with restricted cubic spline with five knots (the 5th, 25th, 50th, 75th, 95th percentiles) for LDL-C level. The lowest 5% and highest 5% of participants were not shown in the figures for small sample sizes. LDL-C, low-density lipoprotein cholesterol.
Discussion
In this post hoc analysis of the CHANCE trial, we found that elevated untreated baseline LDL-C level was associated with an increased risk of new ischaemic stroke at 3 months in patients presenting with a minor ischaemic stroke or TIA. lipid-lowering treatment was associated with reduced risk of new ischaemic stroke at 3 months for those with high baseline LDL-C level.
Numerous previous studies have established that an elevated level of LDL-C is a major contributor to atherosclerotic cardiovascular disease.4 Previous prospective cohort studies also showed linear relationships of higher level of LDL-C with an increased risk of incidence of ischaemic stroke,7 whereas Mendelian randomisation studies of LDL-C and ischaemic stroke have reported conflicting results.5 8 In contrast, there was a limited study that investigated the association between LDL-C level and the prognosis of stroke. The SPARCL trial demonstrated that lowering LDL-C level by statin treatment reduced recurrent stroke during a median of 4.9 years.9 The recent TST trial found that an intensive LDL-C lowering target of less than 1.8 mmol/L (70 mg/dL) further reduced risk of cardiovascular events by approximately 20% during a median follow-up of 3.5 years in patients with ischaemic stroke within 3 months or a TIA within 15 days, compared with the higher target of 2.3–2.8 mmol/L (90–110 mg/dL).10 Recent studies also demonstrated intensive LDL-C lowering treatment with statin may stabilise symptomatic intracranial atherosclerotic plaques and produce greater regression of carotid atherosclerosis.16 17
Our study adds to the evidence that higher levels of LDL-C are associated with increased risk of short-term new stroke in patients with a minor stroke and TIA. Although we failed to demonstrate the association of the level of LDL-C reduction with stroke outcome, we still observed that patients with elevated baseline LDL-C and lipid-lowering treatment after stroke had similar risk of recurrent stroke as those with normal baseline LDL-C but lower risk than those with elevated baseline LDL-C but without lipid-lowering treatment, indicating potential benefit of LDL-C lowering treatment in patients who had a stroke. Our study also showed approximately 93% of patients had LDL-C ≥1.8 mmol/L and approximately 70% patients had LDL-C ≥2.6 mmol/L. Therefore, it is of clinical significance to highlight early identification and control of high LDL-C level, and to further investigate on efficacy of intensive lipid-lowering therapy in patients who had a stroke. The approval of more intensive classes of pharmacological interventions designed to lower cholesterol such as proprotein convertase subtilisin-kexin type 9 inhibitors18 and further trials with these interventions may be warranted.
This study has several limitations. First, details of medication use, such as class, dose, duration and adherence of lipid-lowering agents, were not recorded in this trial; thus, the definition of lipid-lowering treatment was simply according to any record of lipid-lowering agents use during hospitalisation and after discharge. The proportion of lipid-lowering agents use (42%) was lower than recent studies,19 but comparable with contemporary register studies in China.20; 21 Second, statin use before admission was not recorded in the trial and may confound the results. However, proportion of lipid-lowering agents use was very low before index ischaemic event onset according another contemporary national registry studies in China (~2%).21 Third, the LDL-C level at the follow-up visit was not measured in this study; thus, we failed to investigated the association of LDL-C reduction by lipid-lowering treatment with prognosis of stroke. Fourth, immediate testing of cholesterol after ischaemic events may be inappropriately low as it is an inverse phase reactant. Fifth, this study included only minor stroke or high-risk TIA patients (ABCD2 scores ≥4), which may not be generalisable to moderate/major stroke or all TIA samples from population-based cohorts,22 resulted in high events rates. Sixth, the aetiological classification for qualifying events was not collected in the trial and we could not investigate the association between baseline LDL-C level and stroke outcome by stroke subtype. However, patients with a known cardioembolic source were excluded from enrolment in CHANCE. Finally, the sample size for patients with low LDL-C level (<1.8 mmol/L) and outcome of bleeding were small. Additionally, the trial was conducted exclusively in Chinese patients. The finding in this study needs to be further validated in studies with larger sample size and non-Asian populations.
Conclusions
Among patients with minor ischaemic stroke or TIA, elevated untreated baseline LDL-C level was associated with an increased short-term risk of new ischaemic stroke. In contrast, lipid-lowering treatment after stroke onset was associated with reduced risk of new ischaemic stroke for those with high baseline LDL-C level. It is of significance to identify and control the LDL-C level for patients with minor stroke and TIA in clinical practice.
Data availability statement
Data are available on reasonable request. Data are available to researchers on request for purposes of reproducing the results or replicating the procedure by directly contacting the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of Beijing Tiantan Hospital. The IRB approval is submitted together with the manuscript. There is no IRB number provided.
References
Footnotes
YP and RW contributed equally.
Contributors YW is responsible for the overall content as the guarantor, have full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: YP, RW and YW. Supplying participants: JieL, JinL and XM. Drafting of the manuscript: YP, RW and YW. Critical revision of the manuscript for important intellectual content: YX and DTL. Statistical analysis: YP, HL and AJ. Study supervision and organisation of the project: XM and YW.
Funding This study is supported by grants from National Key R&D Program of China (2018YFC1312903), grants from the National Natural Science Foundation of China (81971091, 81870905, U20A20358), Beijing Hospitals Authority Youth Programme (QML20190501), grants from Beijing Municipal Science and Technology Commission (D171100003017002, Z181100001818001).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.