Article Text

Statistics from Altmetric.com
Introduction
Patients with an acute minor ischaemic stroke or high-risk transient ischaemic attack (TIA) had a higher risk of recurrent stroke within 3 months after onset. Dual antiplatelet therapy (DAPT) with clopidogrel and aspirin was more effective than aspirin alone for reducing subsequent events in this patient population in the Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events (CHANCE) and the Platelet-Oriented Inhibition in New TIA and Minor Ischaemic Stroke (POINT) trials. However, clopidogrel in CYP2C19 loss-of-function carriers were less effective in a CHANCE subgroup analysis.1 Ticagrelor, as the first of a new class of antiplatelet agents, is a non-competitive, direct-acting P2Y12-receptor antagonist.2 Unlike the thienopyridine compounds, ticagrelor does not require metabolism to become active. Clopidogrel is an irreversible inhibitor of the P2Y12 receptor, while ticagrelor reversibly inhibits receptor signalling and subsequent platelet activation. In pharmacodynamic studies and trials included patients with acute coronary syndrome, ticagrelor demonstrated faster onset and more potent inhibition of platelet aggregation than clopidogrel, which suggested ticagrelor may contribute to reduced rates of thrombotic events compared with clopidogrel.3 4
In the Acute Stroke or TIA Treated with Aspirin or Ticagrelor and Patient Outcomes (SOCRATES) trial, ticagrelor was not superior to aspirin in reducing the risk of the composite end point of stroke and myocardial infarction. However, ticagrelor plus aspirin showed higher efficacy to prevent recurrent stroke at 90 days in the Platelet Reactivity in Acute Stroke or Transient Ischaemic Attack (PRINCE) trial. In the Acute Stroke or TIA Treated with Ticagrelor and ASA for Prevention of Stroke and Death (THALES) trial, ticagrelor plus aspirin was shown with higher efficacy but also some safety concerns.5 Recently, Ticagrelor or Clopidogrel with Aspirin in High-Risk Patients with Acute Nondisabling Cerebrovascular Events II (CHANCE 2) trial published the results of comparing ticagrelor plus aspirin to clopidogrel plus aspirin for secondary prevention of stroke in CYP2C19 loss-of-function carriers. It showed that ticagrelor plus aspirin can modestly reduce the risk of stroke at 90 days in patients with minor ischaemic strokes or TIAs who were carriers of CYP2C19 loss-of-function alleles .6 These three trials all showed more number of haemorrhagic events although without a statistical difference. However, these three trials also raised the concern of the safety with ticagrelor plus aspirin. We performed this brief meta-analysis of aggregate data from the PRINCE, THALES and CHANCE 2 trials. Considering the difference of interventions between THALES and the other two trials, we made a subgroup analysis of PRINCE and CHANCE 2.
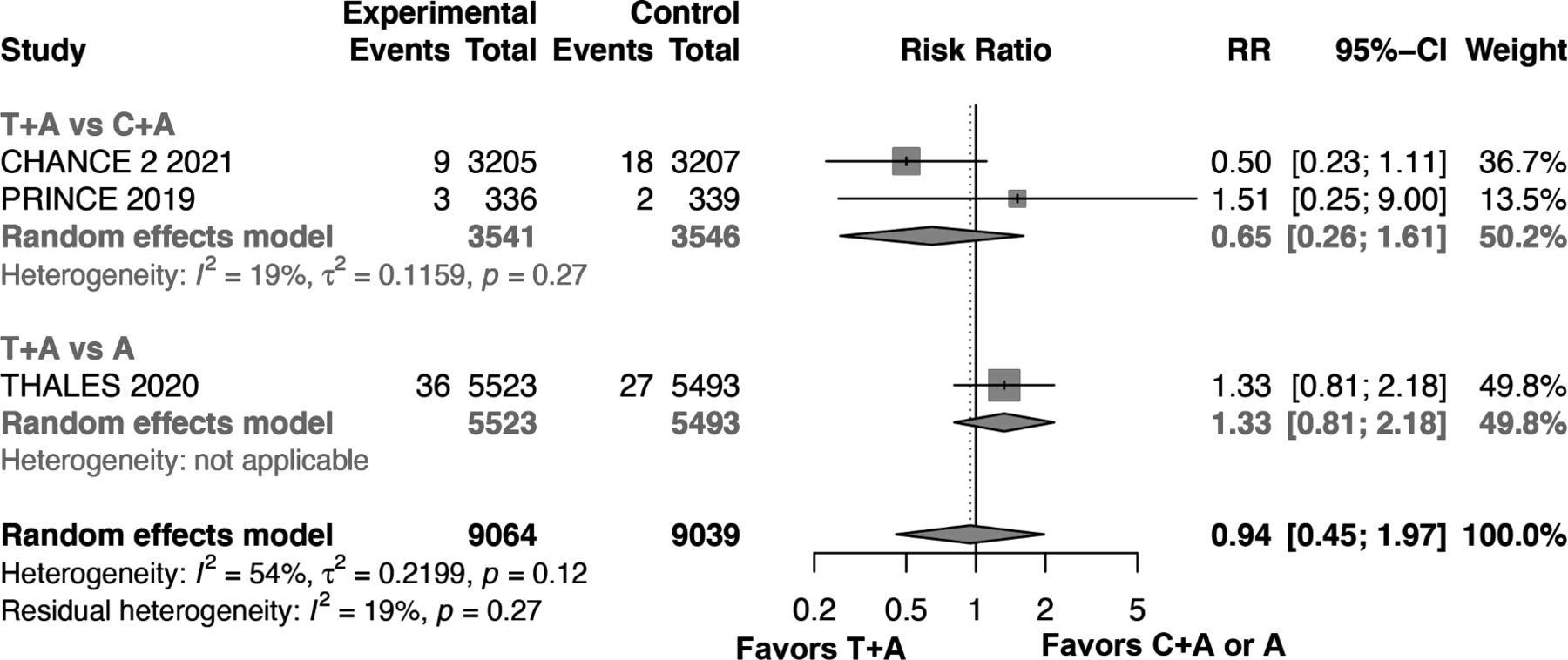
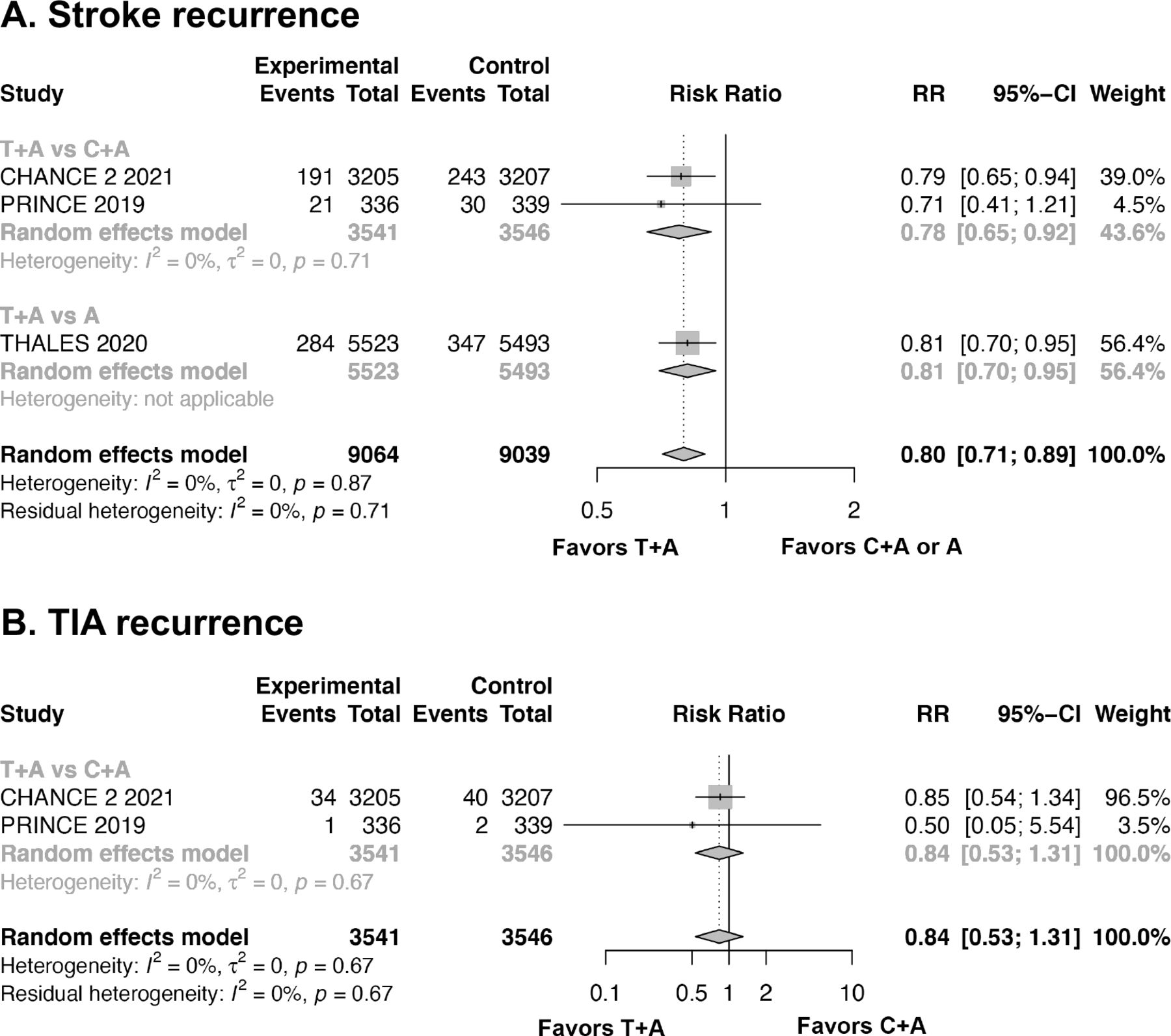
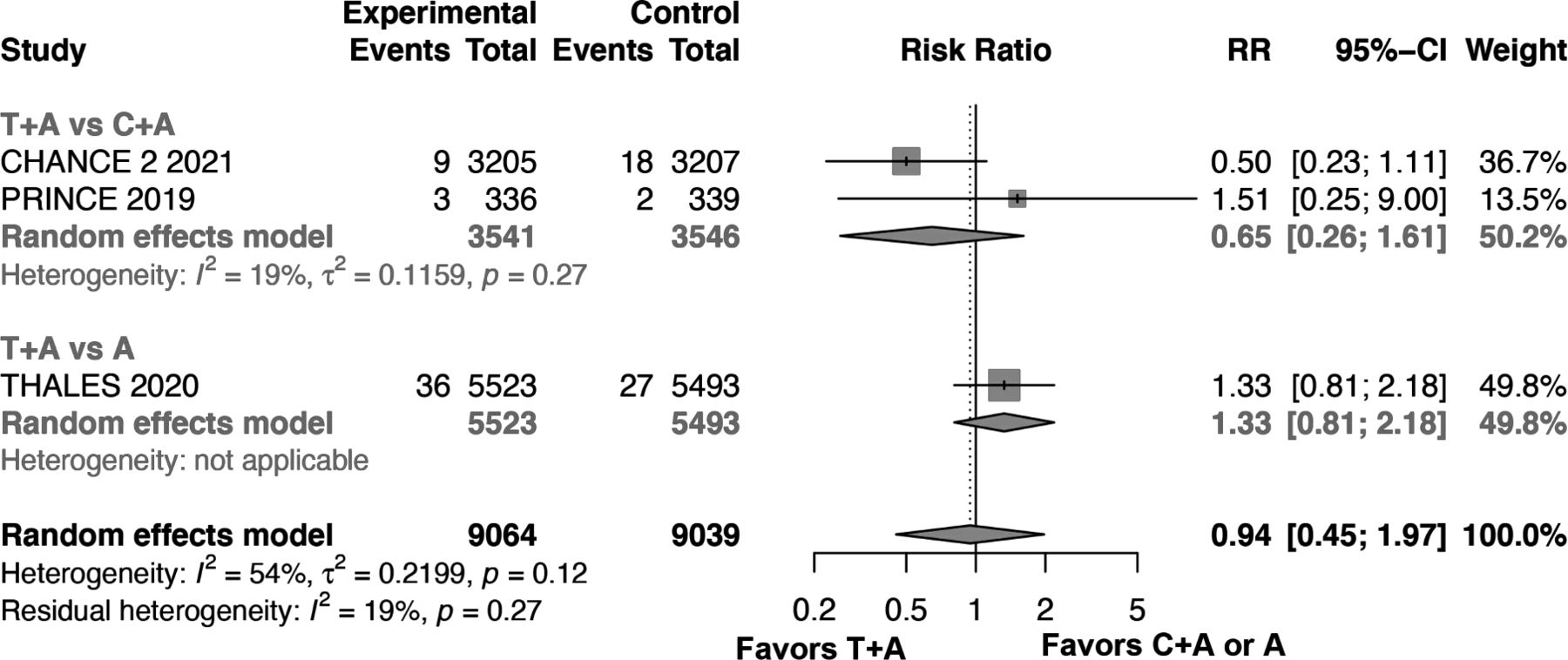
We found that the raletive risk (RR) for all haemorrhagic events was 1.86 (95% Confidence Interval (CI) 1.39 to 2.49) (figure 1) in group treated on ticagrelor plus aspirin. Although there was a significant reduction of stroke in the enrolled patients (figure 2), there was no trend in mortality (RR 0.94, 95% CI 0.45 to 1.97) in ticagrelor plus aspirin group comparing to those won clopidogrel plus aspirin (figure 3).

Forest plot of haemorrhagic events. (A) Forest plot of all bleeding events; (B) Forest plot of intracranial haemorrhage; (C) Forest plot of severe or moderate bleeding events; (D) Forest plot of fatal bleeding events. A, aspirin; C+A, clopidogrel plus aspirin; T+A, ticagrelor plus aspirin; CHANCE 2, Ticagrelor or Clopidogrel with Aspirin in High-Risk Patients with Acute Nondisabling Cerebrovascular Events II; PRINCE, Platelet Reactivity in Acute Stroke or Transient Ischaemic Attack; THALES, Ticagrelor and ASA for Prevention of Stroke and Death; RR, raletive risk; CI, Confidence Interval.
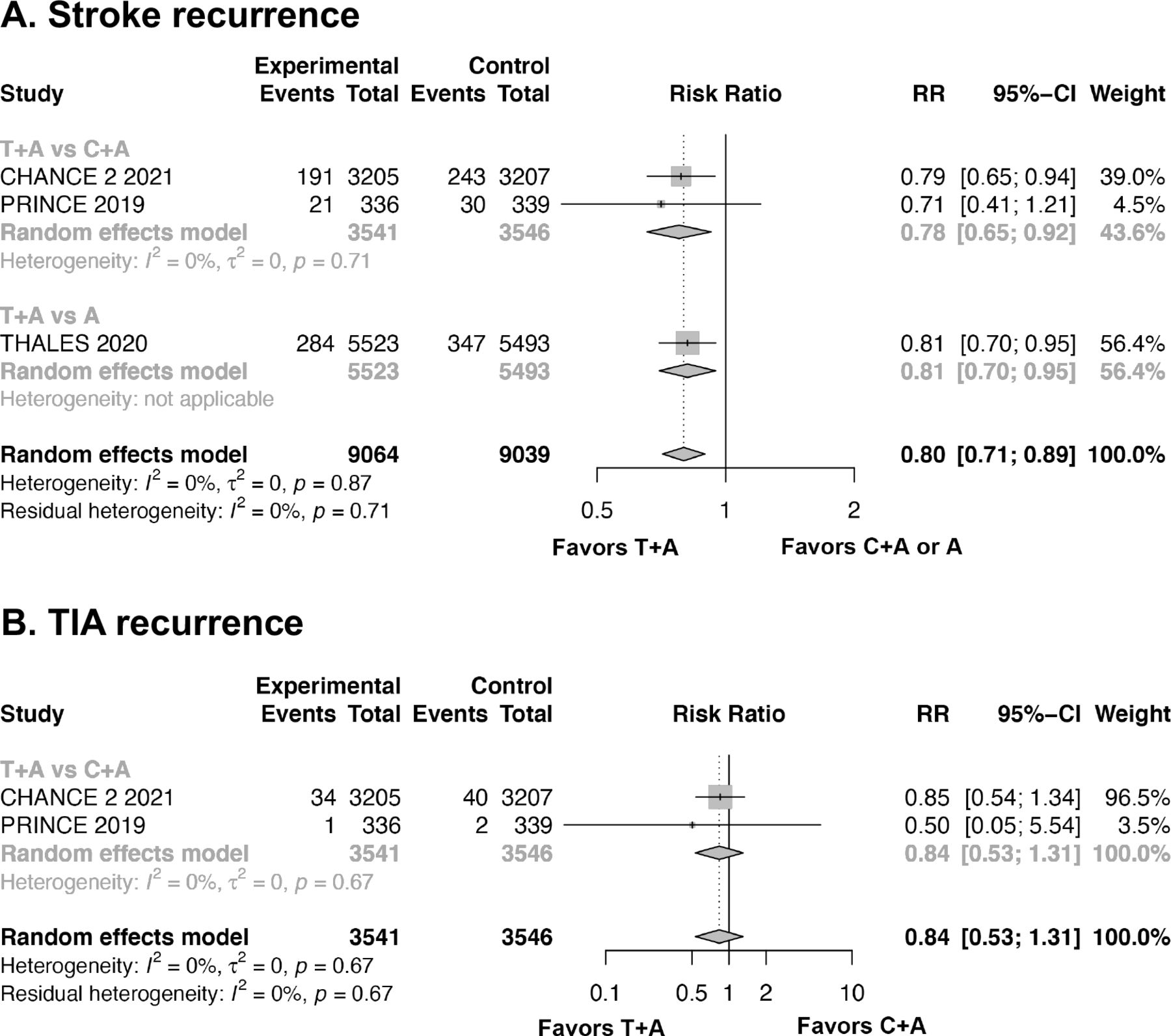
Forest plot of stroke events. (A) Forest plot of stroke recurrence; (B) forest plot of TIA recurrence. A, aspirin; C+A, clopidogrel plus aspirin; T+A, ticagrelor plus aspirin; CHANCE 2, Ticagrelor or Clopidogrel with Aspirin in High-Risk Patients with Acute Nondisabling Cerebrovascular Events II ; PRINCE, Platelet Reactivity in Acute Stroke or Transient Ischaemic Attack; THALES, Ticagrelor and ASA for Prevention of Stroke and Death; TIA, transient ischaemic attack; RR, raletive risk; CI, Confidence Interval.
{kind=link}
{kind=link}
{kind=link}
Forest plot of death. A, aspirin; C+A, clopidogrel plus aspirin; T+A, ticagrelor plus aspirin; CHANCE 2, Ticagrelor or Clopidogrel with Aspirin in High-Risk Patients with Acute Nondisabling Cerebrovascular Events II; PRINCE, Platelet Reactivity in Acute Stroke or Transient Ischaemic Attack; THALES, Ticagrelor and ASA for Prevention of Stroke and Death; RR, raletive risk; CI, Confidence Interval.
Therefore, for every 30 patients treated with ticagrelor plus aspirin, one would experience a haemorrhagic event, compared with those on clopidogrel plus aspirin. Furthermore, for every 68 patients on ticagrelor plus aspirin, one recurrent stroke would be prevented.
Merits and shortcomings
In all trials testing ticagrelor in patients with minor stroke and high-risk TIAs within 24 hours of onset, only CHANCE 2 tested all patients for the carrier state of CYP2C19 loss-of-function alleles (table 1). Our analysis of the published data from these trials showed that ticagrelor plus aspirin might increase the rate of haemorrhagic events, although it also had a moderate reduction of stroke events in patients with minor strokes or high-risk TIAs. Moreover, our analysis showed no benefit from ticagrelor plus aspirin therapy in reducing the rate of mortality.
The intervention of ticagrelor related stroke trials
The major concern of ticagrelor plus aspirin is the higher risk of all bleeding events and severe to moderate bleeding events since the SOCRATES trial. In addition, there was still a controversary between THALES and CHANCE 2 trial. In PRINCE trial, we noticed that any bleeding event was higher in ticagrelor plus aspirin group than clopidogrel plus aspirin group (p=0.007), especially in minimal bleeding events (p=0.003). CHANCE 2 trial showed similar trend of increased rate of haemorrhagic events, but not in the rate of severe haemorrhagic risk.
We noticed that there was a difference in the duration of treatment,which might change the balance of benefit and risk. In the POINT trial, we found that patients on clopidogrel plus aspirin had a lower risk of major ischaemic events but a higher risk of major haemorrhage than those on aspirin alone if the treatment lasted for 90 days.7 However, the first CHANCE trial showed that patients on clopidogrel plus aspirin with lower loading dose and only 21 days reduced the risk of subsequent stroke events without increasing the risk for haemorrhage when compared with those on aspirin alone.8 The results from these two randomised controlled trials (RCTs) may indicate that the haemorrhagic risk might be further lowered by reducing the loading dose and duration of DAPT.
We acknowledge several limitations in our meta-analysis. THALES trial was designed to compare the efficacy of ticagrelor plus aspirin vs aspirin and the other two trials compared ticagrelor plus aspirin to clopidogrel plus aspirin. In addition, there were differences in the study design, endpoint definition and lengths of follow-up.
Future directions
While all three trials analysed favour ticagrelor plus aspirin for secondary stroke prevention in patients already have a minor stroke or TIA, we cannot ignore the haemorrhagic risk of such therapy. While severe or moderate haemorrhagic risk was not that high for either DAPT or aspirin alone in our meta analysis, the available data provide the opportunity for individualised antiplatelet strategy for secondary stroke prevention. The clinicians need to balance the risk of haemorrhage and benefit of preventing a recurrent stroke for every patient that may need DAPT.
Furthermore, a subgroup analysis of the CHANCE trial indicated that patients who were old, male and with a history of aspirin or proton pump inhibitor usage had an increased risk of haemorrhage. In contrary, patients with higher body mass index had a lower haemorrhagic risk. This phenomenon may suggest that DAPT mainly benefit patients at particularly higher risk for recurrent ischaemia but lower risk for haemorrhage.9
Lastly, both PRINCE and CHANCE 2 trial were restricted to Han Chinese patients, which had a higher incidence of intracranial-artery stenosis than non-Asian populations. Our conclusions may not be generalised to other ethnic groups. More RCTs enrolling patients from other ethnic profiles may provide more robust evidence.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Contributors XC and JX performed the analysis, XC, JX and SC drafted the manuscript. YD revised the manuscript. YD and QD concepted this study, supervised the analysis and finalised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.