Article Text

Abstract
Background and purpose This study aimed to investigate the association of metabolic syndrome (MetS) with both intracranial atherosclerotic stenosis (ICAS) and imaging markers of cerebral small vessel disease (CSVD) in a community-based sample.
Methods This study included 943 participants (aged 55.6±9.2 years, 36.1% male) from the community-based Shunyi cohort study. MetS was defined according to the joint interim criteria and quantified by the MetS severity Z-score. ICAS was evaluated by brain magnetic resonance angiography. The MRI markers of CSVD, including white matter hyperintensities (WMHs), lacunes, cerebral microbleeds (CMBs) and enlarged perivascular spaces (EPVS), were assessed. Multiple regression models were used to investigate the association of MetS severity Z-score with ICAS and these CSVD markers.
Results We found that risk of ICAS (OR=1.75, 95% CI 1.39 to 2.21, p<0.001) increased consistently with MetS severity. MetS severity was significantly associated with higher risks of WMH volume (β=0.11, 95% CI 0.01 to 0.20, p=0.02) and lacunes (OR=1.28, 95% CI 1.03 to 1.59, p=0.03) but not the presence of CMBs (OR=0.93, 95% CI 0.74 to 1.16, p=0.51) and PVS severity (EPVS in basal ganglia: OR=0.96, 95% CI 0.84 to 1.09, p=0.51 and EPVS in white matter: OR=1.09, 95% CI 0.96 to 1.23, p=0.21).
Conclusions Our findings suggest that WMH and lacunes share risk factors with atherosclerosis of the cerebral artery, whereas the impact of glucose and lipid metabolic disorder to CMB or EPVS might be weak.
- atherosclerosis
- brain
- MRI
- stroke
- artery
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Metabolic syndrome (MetS), which is defined as a clustering of three or more metabolic risk factors by the joint interim criteria,1 has become a major health hazard of the modern world. The syndrome feeds into the developing of diseases like diabetes mellitus, coronary diseases, cerebrovascular disease and other disabilities. Epidemiological studies over the past decade have shown that about one-quarter to one-half of adults meet the diagnostic criteria of MetS in the USA and Europe. With the economic development and lifestyle changes, the prevalence of MetS in China was as high as 33.9%, with approximately 454 million people affected.2 All of these results suggest that MetS has caused considerable loss of clinical and socioeconomic cost.
The clinical relevance of MetS with cardiovascular disease has been widely recognised since we can see the effect of all these inter-related risk factors of MetS on increasing the burden of coronary diseases. However, few studies have established a strong link between MetS and cerebrovascular disease as the biological mechanisms underlying cerebrovascular disease are much more complicated and not all cerebrovascular diseases can be interpreted by one consistent and reliable mechanism. Convincing evidence has revealed that the atherosclerotic process generally affects the cerebral large vessels, while in the pathogenesis of cerebral small vessel disease (CSVD), non-atherosclerotic and non-occlusion mechanisms, such as hyaline arteriolosclerosis and increased blood–brain barrier (BBB) permeability, also play important roles.3 Therefore, the differential effect of MetS on small or large cerebral arteries should be taken into consideration.
MetS was independently associated with intracranial atherosclerotic stenosis (ICAS) and even was a predictor of future intracranial atherosclerotic stroke.4 However, current evidence about the relationship between MetS and CSVD is limited and controversial. The neuroimaging features of CSVD include white matter hyperintensities (WMHs), lacunes, cerebral microbleeds (CMBs) and enlarged perivascular spaces (EPVS).5 None of the studies, to date, has systematically studied the effect of MetS on these neuroimaging markers of CSVD in one population. We are not yet certain whether MetS is the shared risk factor for all CSVD markers or quite different results are seen for distinct CSVD markers.
In the present study, we focused on the impact of MetS on two different pathological states of cerebral vessels, ICAS and CSVD, in a Chinese community population.
Methods
Population
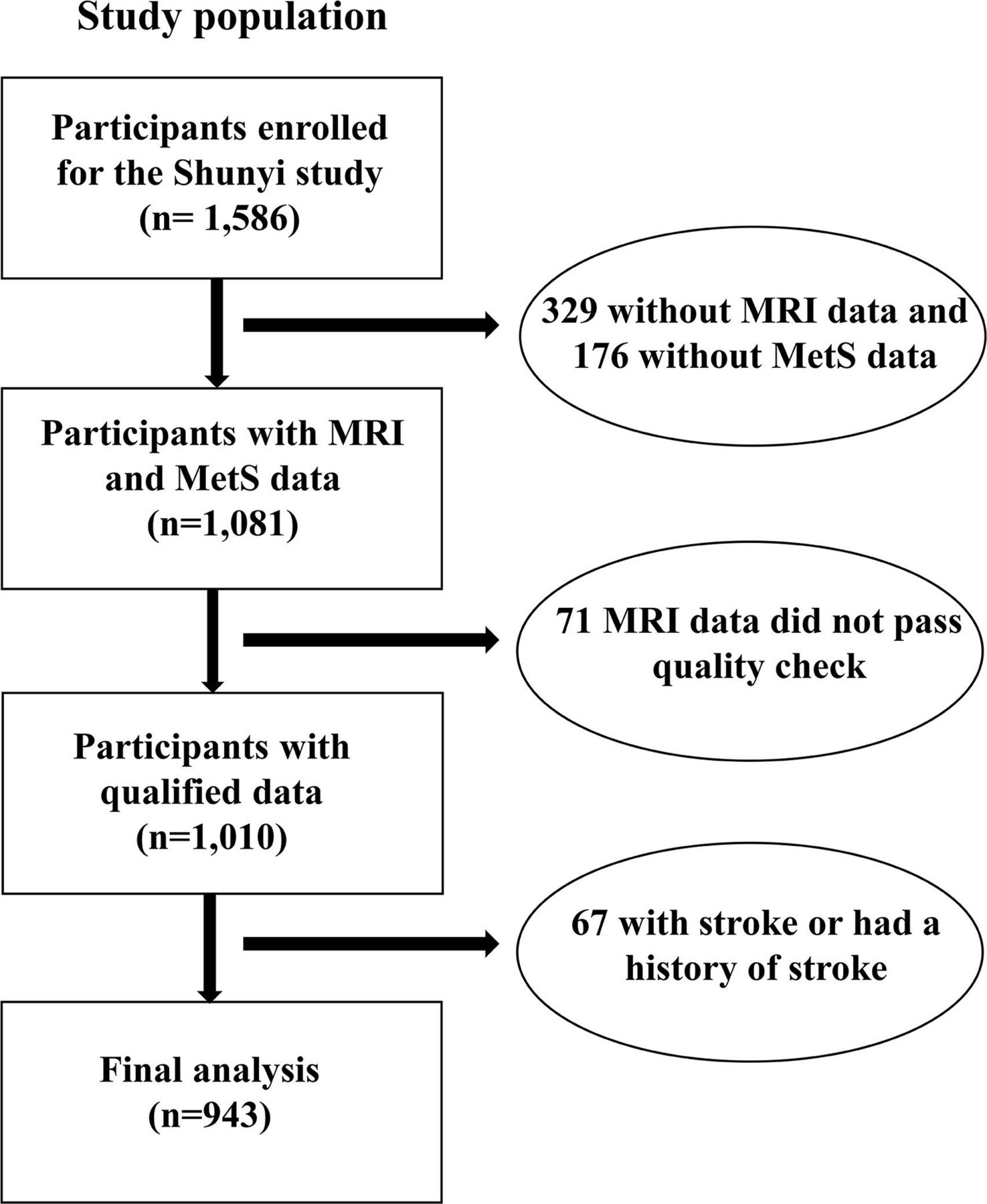
Shunyi study is an ongoing community-based prospective cohort, which is designed to investigate the risk factors and consequences of cardiovascular and age-related brain diseases.6 All inhabitants aged 35 years and older residing in five villages of Shunyi, a suburb district of Beijing City, were invited. The original sample for the Shunyi study included a total of 1586 individuals recruited from June 2013 to April 2016. In total, 1257 participants received MRI scans, and those without MRI scans had contradictions to MRI or were eligible but did not undergo MRI. Compared with participants who underwent brain MRI, those who did not were older, more likely to be male and current smoker (shown in online supplemental materials). Out of the remaining 1257 subjects, 247 subjects were excluded from our study because they had missing data for diagnosing MetS (n=176) or their MRI data did not pass the quality check (n=71). For the present analysis, 67 subjects were further excluded from our study because they were diagnosed with a stroke or had a history of stroke.
Supplemental material
The final analysis was performed based on 943 subjects (figure 1).

{kind=link}
Flow diagram of the study population. MetS, metabolic syndrome; MRI, magnetic resonance imaging.
Definition and quantification of MetS
For assessment of metabolic risk factors, structured questionnaires and standardised physical examination were used together with essential laboratory measurements. Detailed protocols are shown in online supplemental materials.
According to the joint interim criteria, the metabolic risk factors of MetS were defined as followed: (1) waist circumference ≥90 cm in males and ≥85 cm in females, (2) decreased plasma high-density lipoprotein cholesterol (HDL-C) levels <1.03 mmol/L (40 mg/dL) in males and <1.29 mmol/L (50 mg/dL) in females, (3) elevated plasma triglyceride levels ≥1.69 mmol/L (150 mg/dL), (4) elevated blood pressure ≥130/85 mm Hg or administration of antihypertensive medication and (5) elevated fasting plasma glucose level ≥5.6 mmol/L (100 mg/dL) or treatment with glucose-lowering medication. Of note, we modified the cut-off value of waist circumference for Chinese.7 The presence of MetS was diagnosed when three or more of the above MetS risk factors were met in one participant.
Considering the limitations of these dichotomous MetS criteria in previous studies, we deployed a continuous MetS severity Z-score. This score was on a sex-specific and race/ethnicity-specific basis with a different weighted contribution of each component. Briefly, a set of confirmatory factor analyses were performed on the five traditional MetS components, namely WC, HDL, triglycerides, systolic blood pressure and fasting glucose, to calculate the MetS severity Z-score, the detail of which was described previously.8 The MetS severity Z-score can be automatically calculated by the Metabolic Syndrome Severity Calculator, which is an HTML and JavaScript implementation using established and well-researched equations (https://metscalc.org/). The name of MetS severity Z-score was derived from its standard normal distribution, with increased scores representing a higher risk for the value of latent MetS factor. The MetS severity Z-score has been proven useful in identifying people with an increased risk for MetS-related diseases, such as serving as a good predictor of future type 2 diabetes and cardiovascular disease.9
Brain MRI acquisition and analysis
Participants were scanned MRI on a single 3T Skyra scanner (Siemens, Erlangen, Germany). The thorough detailed MRI protocols have been described in online supplemental materials.
The MRI markers of CSVD were defined according to published criteria. The automagical quantification of WMHs volume was achieved by the lesion growth algorithm implemented in the lesion segmentation tool (LST) toolbox (http://www.statistical-modelling.de/lst.html) of Statistical Parametric Mapping(https://www.fil.ion.ucl.ac.uk/spm/). According to the STandards for ReportIng Vascular changes on nEuroimaging (STRIVE) criteria, lacunes were defined as focal round or oval deep infarcts between 3 and 15 mm in diameter, which had the same signal characteristics as cerebrospinal fluid on all sequences.10 We defined CMBs as round or ovoid hypointense lesions on SWI sequences according to the standard published criteria.11 The EPVS severity was rated using the visual grading method both in basal ganglia (BG) and white matter (WM).12 The EPVS burden was categorised as mild EPVS (degree 1), moderate EPVS (degree 2) and severe EPVS (degrees 3 and 4).
The presence of ICAS was evaluated on brain MRA according to the criteria described in Warfarin-Aspirin Symptomatic Intracranial Disease trial.13 The presence of ICAS was defined as any stenosis of the following arteries on MRA: intracranial segment of internal carotid arteries, anterior cerebral artery, middle cerebral arteries, posterior cerebral artery, intracranial segment of vertebral artery and basilar artery (BA).
Well-trained readers blinded to all clinical data rated WMHs, lacunes, CMBs, EPVS and ICAS independently. The intra-rater agreements were assessed in a randomly selected sample of 50 individuals with an interval of more than 1 month between the first and second readings. The results of the intrarater agreement were as follows: the intraclass correlation coefficient was 0.95 for BA diameter, 0.96 for ICA diameter, 0.75 for EPVS-BG and 0.67 for EPVS-WM, and kappa coefficient was 0.95 for lacunes and 0.90 for CMB. For automatic segmentation of WMH using the LST toolbox, the Dice coefficient was 0.62 at threshold κ=0.15 when compared with manual segmentation.
Statistical analysis
The baseline characteristics were presented as mean (SD) for continuous variables, frequency (percentage) for categorical variables and the median (IQRs) for the skewed distributed parameters. Between-group differences in demographic and neuroimaging characteristics were examined by independent Student’s t-test (for normally distributed data), Mann-Whitney U test (for non-normally distributed data) or Pearson χ2 test (for categorical variables).
Since the skewness of the distributions of the WMHs volume, the WMHs volume was log-transformed with a base of e for statistical model inferences. Binary logistic regression models with ORs and 95% CIs were used to explore associations of the MetS severity Z-score with the presence of CMBs, lacunes and ICAS. Multiple linear regression models with mean differences and 95% CIs were constructed to evaluate the relationship between the MetS severity Z-score and the volume of WMH. Multiple logistic regression model was used to investigate the association between the MetS severity Z-score and EPVS severity in both BG and WM. Models initially adjusted for age and sex (model 1). Additional analyses were adjusted for use of antihyperlipidaemic medication, use of antihypertensive medication, use of antidiabetic medication and current smoking status (model 2).
All numerical calculations were performed by SPSS software (Statistical Package for Social Science, SPSS V.25, SPSS Inc, Chicago, Illinois, USA). For all statistical analyses, two-tailed p<0.05 was considered to be statistically significant.
Results
The final study sample consisted of 943 subjects. The baseline characteristics of the study subjects were shown in table 1. Of the 943 participants, the mean age of the final study population was 55.6 years (SD 9.2), and 340 (36.1%) participants were male. According to the joint interim criteria, the presence of MetS was found in 496 (52.6%) subjects. Subjects with MetS were older and more likely to be female.
Baseline characteristics of the participants with and without metabolic syndrome (MetS)
Association between MetS and the presence of ICAS
At baseline, a total of 123 (13.0%) participates had ICAS. Out of all subjects with MetS, 88 (17.7%) had ICAS, whereas only 35 subjects of the non-MetS group (7.8%) had ICAS (p<0.001) (table 2). The associations between ICAS and MetS severity were shown in table 3. We found that the one who had more severe MetS had a higher risk of having ICAS (OR=1.75, 95% CI 1.39 to 2.21, p <0.001).
Neuroimaging characteristics of the participants with and without metabolic syndrome (MetS)
Association between ICAs, MRI markers of CSVD and MetS severity Z-score
Association between MetS and CSVD markers
For neuroimaging markers of CSVD, presence of lacunes was observed in 137 (14.5%) participants and CMBs were observed in 102 (10.8%) participants. Severe EPVS in BG and WM were found in 135 (14.3%) and 141 (15.0%) participants, respectively. The mean WMH volume was 0.9 (0.3–2.8) mL. Compared with subjects without MetS, MetS group presented an increased level of WMHs volume (1.1 (0.3–2.9) vs 0.7 (0.2–2.2) mL; p=0.001) and higher risk of lacunes (84 (16.9%) vs 53 (11.9%), p=0.03), while there existed no significant difference as for the presence of CMBs (57 (11.5%) vs 45 (10.1%), p=0.48) and EPVS severity (EPVS in BG: p=0.72; EPVS in WM: p=0.52) (table 2).
The associations between CSVD markers and MetS severity Z-score were shown in table 3. MetS severity was associated with increased levels of WMHs volume (β=0.16, 95% CI 0.07 to 0.24, p<0.001) and elevated risk for lacunes (OR=1.40, 95% CI 1.14 to 1.72, p=0.002). However, there existed no significant association among MetS severity with presence of CMBs (OR=0.98, 95% CI 0.79 to 1.22, p=0.86) and severity of EPVS (EPVS in BG: OR=0.97, 95% CI 0.86 to 1.11, p=0.69 and EPVS in WM: OR=1.13, 95% CI 1.00 to 1.27, p=0.06). Further adjustments for current smoking status, use of antihyperlipidaemic medication, use of antihypertensive medication and use of antidiabetic medication did not attenuate these associations.
Discussion
In the present study, we found that increasing MetS severity was associated with an increased occurrence of ICAS, as well as WMHs and lacunes. However, no association between MetS and CMBs or EPVS was found.
Consistent with previous studies, we found an association between MetS and ICAS in our community-based study population. Recent clinical studies found that MetS was related to various indices of early atherosclerosis, such as carotid intimal medial thickness or carotid plaque,14 suggesting that MetS plays an important role in initiating the progression of atherosclerosis. Our finding adds to the evidence that MetS might be a risk factor for intracranial large artery atherosclerosis.
In terms of CSVD markers, MetS severity was associated with higher WMHs volume and presence of lacunes but not the presence of CMBs and EPVS severity. The effect of MetS on these CSVD markers remains inconclusive as there were respective results in different pieces of literature. Two studies found the association between MetS and WMHs volume in the elderly population15 16 and one study concluded that the MetS is associated with the incidence of deep CMBs in the Japanese population.17 However, the other two studies concluded that MetS was associated with neither an increased occurrence of WMH nor the presence of lacunes and CMBs.18 19 The discrepancies between the studies might come from the differences in subject characteristics and study design. None former studies have been performed to explore the association between MetS and EPVS severity.
Our findings indicate the heterogeneous pathological nature of CSVD markers. One possible explanation of the association between MetS and WMH or lacunes is that it is the secondary outcome of MetS being a risk factor for large artery atherosclerosis. Abundant evidence suggests that the small infarctions located in BG or WM can result in WMH or lacunes in the chronic stage. These small infarctions could be secondary to obstruction of perforating arteries via the mechanisms of atheromatous branch occlusion or artery-to-artery embolism, which is not pure CSVD but rather a consequence of large artery atherosclerosis. Our results of the coexisting strong relation between MetS and ICAS also support this hypothesis.
We found no association between MetS and CMBs or EPVS, suggesting the two CSVD markers are more likely to relate to distinct pathogenesis. CMBs as the perivascular deposition of haemosiderin-containing macrophages and EPVS as focal accumulations of interstitial fluid following the path of perforating arteries both indicate that BBB disruption plays an important role. Results reported by the Three-City Dijon MRI study showed that hypercholesterolaemia, a steady risk factor for large vessel atherosclerosis, was inversely associated with EPVS severity in WM.20 The Rotterdam Scan study found that serum total cholesterol levels were inversely related to the presence of CMBs, especially the presence of strictly lobar microbleeds.21 In regard that MetS is an indicator mainly describing the disorder of glucose and lipid metabolism, our results armed with previous evidence probably suggest the weak or lacking impact of glucose and lipid metabolic disorder to the certain lesion of the cerebral small vessel wall.
The main strengths of the current study include the large population sample size, the application of MetS severity Z-score and the comprehensive evaluation of atherosclerotic and CSVD markers. There are several limitations to address. One limitation is that our study has a cross-sectional design that precludes us to make a causal inference from the observed associations between MetS and two distinct types of cerebral vascular diseases. Therefore, longitudinal prospective studies are warranted to elucidate the relationship. Second, this is a study based on a community in rural China, primarily involving individuals with a higher prevalence of MetS, which therefore constrain the generalisability of these conclusions to other populations.
Overall, our findings demonstrated that MetS was significantly associated with ICAS, WMHs and lacunes. However, MetS was not associated with CMBs and EPVS severity. The diversity of potential pathogenesis of cerebral large and small vessel implies the necessity of future studies on different treatment or prevention strategies targeting large or small vessel.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for the Shunyi study was obtained from the Medical Review Ethics Committee of Peking Union Medical College Hospital (Reference number: B-160). Written informed consent was obtained from all participants before they were included in the study.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception or design of the work: M-JS, Y-CZ. Acquisition of data: M-JS, D-DZ, F-FZ, FH, L-XZ, JN, MY, L-YC, S-YZ, Z-YJ and Y-CZ. Analysis of data: M-JS, F-FZ, FH, D-DZ and Y-CZ. Interpretation of data: M-JS, H-JZ and Y-CZ. Drafting the work: M-JS, D-DZ and F-FZ. Revising the work for valuable intellectual content: M-JS, D-DZ, H-JZ and Y-CZ. Final approval of the version: H-JZ and Y-CZ.
Funding The study was funded by the '13th Five-Year' National Science and Technology Major Project for New Drugs(grant number: 2019ZX09734001), National Natural Science Foundation of China (grant number: 81971138), and the Strategic Priority Research Program“Biological basis of aging and therapeutic strategies”of the Chinese Academy of Sciences (grant number: XDB39040300).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.