Article Text

Abstract
Background In recent years, a growing number of stents and stent-like devices have become available to facilitate the treatment of challenging aneurysms. However, the need for dual antiplatelet therapy can limit their use, especially in ruptured aneurysms. The hydrophilic polymer coating (pHPC, phenox) is a novel glycan-based multilayer polymer that reduces platelet adhesion. This study aims to report our initial experience using the pCONUS HPC device for the treatment of unruptured wide-necked bifurcation aneurysms (WNBA) using acetylsalicylic acid (ASA) as single antiplatelet therapy (SAPT).
Methods We retrospectively identified all patients who were treated with the pCONUS HPC for unruptured WNBA in a multi-staged procedure using ASA as SAPT. Records were made of periprocedural complications, clinical outcome and angiographic and clinical follow-up.
Results We identified 15 patients with 15 WNBA. The average age was 69 years old (range, 41–76). Seven aneurysms were located in the middle cerebral artery, five in the anterior communicating artery, two at the basilar tip and one in the posterior communicating artery. Immediate post-treatment angiography showed five aneurysms with modified Raymond-Roy classification (mRRC) grade I and four aneurysms with mRRC grade II. There were no haemorrhagic complications. Four patients developed thrombus formation during the second treatment session, all of them completely resolving after administration of glycoprotein IIb/IIIa antagonists. Angiographic follow-up data were available for 10 patients and showed adequate occlusion (mRRC I or II) in eight aneurysms (80%). In-stent stenosis was observed in one patient whereas two patients showed de novo stenosis in one of the efferent branches.
Conclusions This early experience on the use of the pCONUS HPC device suggests that it can be useful for treating unruptured WNBA under ASA as SAPT. Further investigation with a randomised treatment registry and larger cohort is needed.
- aneurysm
- coil
- device
- drug
- platelets
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Wide-necked bifurcation aneurysms (WNBA) have classically been considered challenging for endovascular treatment (EVT). In recent years, numerous stent-like devices have specifically been designed to treat this kind of aneurysms, including the pCONUS1 and the pCANVAS2 (phenox, Bochum, Germany), the PulseRider3 (Pulsar Vascular, Los Gatos, California, USA) and the eCLIPs4 (Evasc Medical Systems Corp). Although these devices have facilitated the treatment of WBNA, the need for dual antiplatelet therapy (DAPT) to prevent thromboembolic complications remains a major issue. In daily practice, issues related to DAPT (eg, hypo-response, hyper-response and non-compliance) are frequent.5 The possibility to implant less thrombogenic devices under single antiplatelet therapy (SAPT) may minimise the risk of both thromboembolic and haemorrhagic complications.
Recent in vitro studies have shown that the hydrophilic polymer coating (pHPC, phenox, Bochum, Germany) has strong antithrombogenic effects.6 7 In this retrospective study, we describe our initial experience using the pCONUS HPC device under acetylsalicylic acid (ASA) as SAPT exclusively in unruptured aneurysms, and discuss the technical success, complication rates, and clinical and angiographic outcomes.
Materials and methods
Device description
Both the pCONUS and the pHPC coating are CE marked and are available for clinical use in Europe. A detailed description of the pCONUS1 and pCONUS2 as well as its coated versions has previously been given by other authors.8
Patient selection
We retrospectively reviewed our prospectively maintained database to identify all patients that underwent pCONUS HPC-assisted coil embolisation of an incidental WNBA using ASA as SAPT in a multi-staged procedure.
All patients were informed about the entire range of therapeutic options, including conservative management, microsurgical clipping, endovascular coil occlusion and stent-assisted coiling. The use of the pCONUS device was based on the anatomic features of the target aneurysm. The use of the traditional uncoated device (pCONUS) under DAPT versus the use of the coated version (pCONUS HPC) under SAPT as a device with reduced thrombogenicity was explained and offered to each patient. The patient’s informed consent was obtained in written form in all cases at least 24 hours before the procedure.
Endovascular treatment
All patients were treated under general anaesthesia using a biplane digital subtraction angiography (DSA) unit (Axiom Artis, Siemens, Erlangen, Germany). Procedures were performed via the right common femoral route using a 7F access system and were performed under heparin anticoagulation with a 3000 IU or 5000 IU bolus dose of unfractionated heparin intravenous at the start of the procedure. All flushing solutions, including the guide catheters and microcatheters, were heparinised (5000 IU unfractionated heparin/L). Activated clotting time was not routinely tested.
Rotational angiography was used to accurately assess the anatomy of the aneurysm, the afferent artery, and any vessels efferent from the neck of the aneurysm. Rotational angiography with three-dimensional reconstruction was also used to correctly size the pCONUS device to both the afferent artery and the aneurysm neck/base.
Unlike the standard technique for the use of the pCONUS, in which device implantation and coil occlusion are performed in one setting, all patients included in this series underwent a stepwise treatment, in which the pCONUS was implanted in the first intervention, followed by coiling of the aneurysm in a subsequent session. Though the one setting technique has been shown to be technically successful and safe, complete occlusion rates at follow‐up was only 60% in the meta-analysis by Sorensen et al,1 with 14% of aneurysms requiring retreatment. Our logic behind performing staged treatment was to enable some endothelialisation of the pCONUS between sessions. This may prevent the device from dislodging during coiling, and therefore allow denser packing and stable occlusion. Staged stenting procedures have previously been described for the EVT of intracranial aneurysms.9 The second setting was normally scheduled for 6 weeks after pCONUS implantation.
Antiplatelet regimen
The decision to perform the treatment under SAPT was based on an interdisciplinary discussion and individual aspects. Clinical arguments in favour of SAPT were a higher risk under DAPT (eg, essential thrombocytopenia, simultaneous treatment with vitamin K antagonist or history of gastrointestinal bleeding) or anticipated patient non-compliance. Patients received 100 mg ASA per os (PO) twice a day for at least 5 days before treatment or a loading dose of 500 mg ASA PO on the day before treatment. Post-procedural medication consisted of 100 mg ASA PO twice a day continued for 3 months following treatment and a daily dose of 100 mg ASA PO continued for life thereafter. The effectiveness of the antiplatelet regimen was tested using the Multiplate analyser (Roche Diagnostics, Mannheim, Germany) and VerifyNow (Accriva, San Diego, California, USA).
Data collection and follow-up
Patient age and gender, type of aneurysm, location, size, status at presentation, degree of occlusion as well as technical and clinical complications during or after the treatment were all retrospectively evaluated.
To establish a correlation between the coated device and the risk of silent microembolic lesions, we routinely obtained an MRI with diffusion-weighted imaging (DWI) approximately 24 hours after each procedure. Microembolic lesions appear as high signal intensity (HSI) spots on DWI. Cases showing any HSI spot in the arterial territory of the vessel where the guiding catheter was placed were regarded as DWI positive.
Immediate and follow-up occlusion was rated according to the modified Raymond-Roy classification (mRRC).10 Clinical evaluation was performed and recorded after the procedure, at discharge and follow-up by a neurologist or a certified stroke nurse not involved in the EVT. Morbidity and mortality were scored using the modified Rankin Scale (mRS).11 Angiographic follow-up was routinely scheduled initially at 3–6 months, again at 9–12 months and then at 2 years.
Results
We identified 15 patients (10 women, 5 men) with 15 unruptured WNBA that were sequentially treated with the pCONUS HPC device using only ASA as SAPT. The average age of the patients was 69 years old (range 41–76). The middle cerebral artery bifurcation was the most common location (N=7), followed by the anterior communicating artery (AcomA, N=5), the basilar tip (N=2) and a single case involving the posterior communicating artery (PcomA, N=1). The average dome height was 9 mm (range 3–12 mm), average dome width was 6 mm (range 3–14 mm) and average neck width was 5 mm (range 2–8 mm).
One patient (Patient 3) had been prescribed Dabigatran for concomitant atrial fibrillation. In the remaining 14 patients, premedication and postmedication consisted of SAPT with ASA as described above. Patient 4 was found to be non-compliant with this standard dose, so this had to be increased to 500 mg ASA PO daily after treatment. In Patient 7 a periprocedural dissection of the internal carotid artery (ICA) caused by the guide catheter was observed at the end of the first treatment. The patient remained asymptomatic, but MRI on the following day showed worsening of the dissection with almost complete obliteration of the true lumen and local thrombus formation. The ICA was reconstructed with three flow diverter stents (FDS) followed by coil occlusion of the aneurysm 2 days after the first setting after switching the patient to DAPT. Table 1 summarises the baseline demographics, aneurysms characteristics and antiplatelet therapy (APT) in this series.
Aneuryms size, location and antiplatelet regimen
Complications
Periprocedural complications occurred in 5 of the 30 interventions (16.7%). Four non-occlusive thrombi formations were observed coming out of the aneurysm into one of the protected efferent branches during the coil occlusion. All of them resolved after intra-arterial administration of 2 mL (4 mg) eptifibatide (Integrilin, GlaxoSmithKline, Munich, Germany) and the remainder of the weight adapted bolus given intravenously. Postoperative infusion of eptifibatide intravenous was not needed for any patient. There were no clinical consequences from the formation of these thrombi (figure 1). In Patient 7 a dissection of the cervical ICA was observed at the end of the first treatment, which was initially treated conservatively. Despite the patient remaining asymptomatic, the MRI performed the following day showed radiological worsening with almost complete occlusion of the true lumen and local thrombus formation. Reconstruction of the ICA with FDS and coil occlusion of the aneurysm was successfully performed after switching the patient to DAPT.

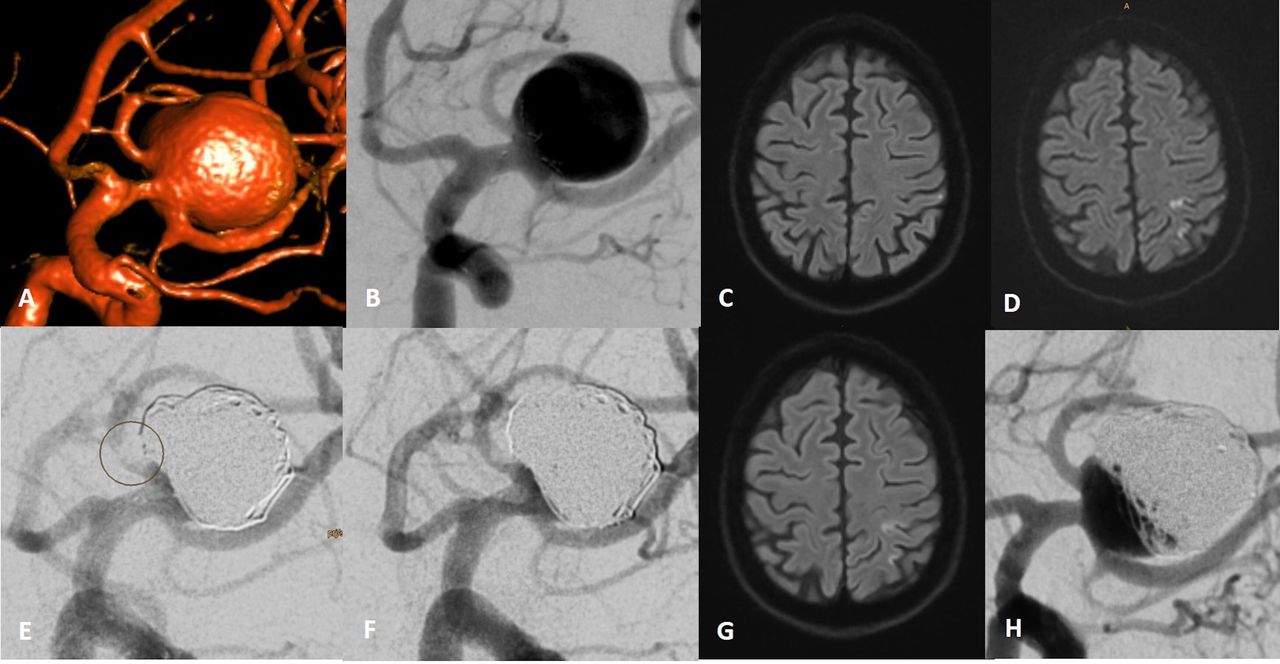
Working projection for proper deployment of the pCONUS HPC device in an incidental wide-necked middle cerebral artery (MCA) bifurcation aneurysm on the right side (A). Positioning of a 4-15-10 mm pCONUS2 HPC with correct expansion of the four petals by the arrangement of the radiopaque markers (B). Diffusion-weighted imaging obtained the following day showed small high signal intensity spots in the right postcentral gyrus (C). Working projection for coil occlusion of the aneurysm 7 days after pCONUS HPC implantation (D). After complete embolisation of the aneurysm, a non-occlusive thrombus was observed at the neck of the aneurysm and superior branch of the MCA (E, arrow). Final run after a weigh-adapted bolus of eptifibatide with nearly complete thrombus removal (F).
Additionally, one patient (Patient 11) presented with in-stent-thombosis 3 months after the first session. This patient was being treated for an AcomA aneurysm with the pCONUS HPC in a staged fashion. After the first session, the patient had to be operated on for breast cancer, with a second surgery due to rebleeding. After the second intervention, the patient presented with acute paresis of the left leg. MRI and DSA examination showed complete thrombosis of the aneurysm sac with thrombus formation along both A2 segments as well as the stent shaft. The patient was then switched to DAPT. Angiographic follow-up after 2 weeks showed complete reperfusion of the aneurysm and resolution of the previous thrombus along the stent. Coil occlusion of the aneurysm sac was then successfully performed. mRS at discharge was rated as 2.
Postinterventional MRI was available for all but one patient after the first treatment session (93.3%) and in 13/15 patients after the second session (86.7%). Microembolic lesions (DWI+) were observed in 13 of 14 patients (92.8%), and in 8 of 13 patients (61.5%), respectively, with all patients remaining asymptomatic. In Patient 7, DWI lesions were most probably secondary to the iatrogenic ICA dissection. Patient 4 showed an isolated spot after the first treatment. At the time of the second treatment, the patient commented that she had stopped the medication without consultation. MRI was then performed, showing multiple HSI spots in the arterial territory of the treated vessel. After insufficient inhibition to the standard dose of ASA was confirmed, the patient was reloaded with 500 mg ASA intravenous and DSA was performed, showing complete patency of the pCONUS HPC. This patient was one of the two patients presenting with periprocedural thrombus formation. Table 2 summarises the clinical and angiographic follow-up results for this series.
Clinical and radiographic outcome
Angiographic results
The pCONUS HPC was successfully deployed and detached in the first treatment session in all patients. Coil occlusion was done at an average of 40 days (range 2–106) after the pCONUS HPC implantation. Successful catheterisation of the aneurysms through the stent shaft for coiling was possible in all procedures. Although the literature suggests that endothelisation takes at least 6 weeks for standard stents, partial endothelisation has been observed within a week and might help to stabilise a recently implanted pCONUS.12 Inadvertent migration of the respective pCONUS HPC device was not encountered in any of the patients who were treated in a staged fashion, either before or during coil occlusion, including those patients with less than 1 week between both treatment settings such as Patient 4 and 7.
Complete occlusion of the aneurysm after the coiling procedure was achieved in five patients (33.3%) whereas four patients (26.7%) showed a neck remnant, and six patients (40%) showed residual perfusion at the end of the procedure.
One patient in our cohort died during the follow-up period for reasons unrelated to the EVT. Angiographic follow-up was performed in 10 of the 14 surviving patients (71.4%) at an average of 168 days (range 77–394 days). Of these 10 patients, 5 showed completely occluded aneurysms (50%), 3 patients showed neck remnants (30%), and residual filling was seen in the remaining 2 patients (20%). One patient had to be retreated during the follow-up period (Patient 4) (figure 2).
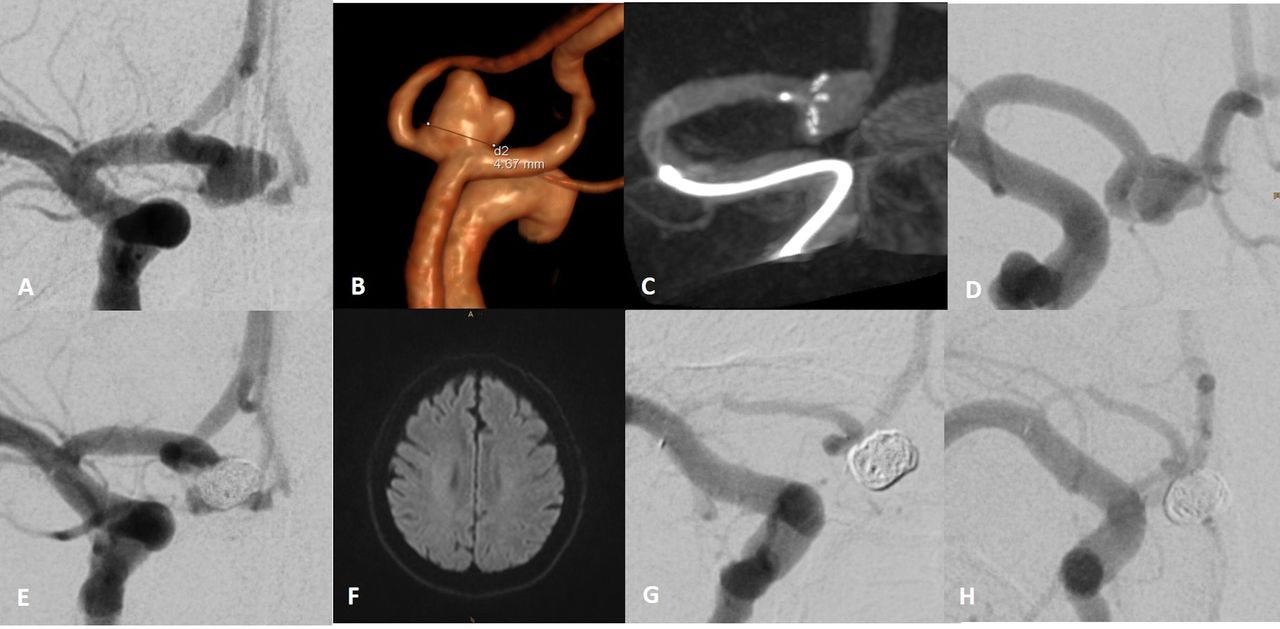
Three-dimensional reconstruction showing a wide-necked middle cerebral artery (MCA) bifurcation aneurysm on the left side (A). Positioning of a 4-15-15 mm pCONUS2 HPC via a 21-inch microcatheter within the aneurysm under acetylsalicylic acid (ASA) as single antiplatelet therapy (B). Diffusion-weighted imaging (DWI) obtained the following day showed a single high signal intensity (HSI) spot in the left precentral gyrus (C). DWI obtained at the time of the second treatment showed multiple new HSI spots (D). Patient had stopped the medication without consultation. VerifyNow confirmed insufficient inhibition (ARU:513). After administration of 500 mg ASA intravenous, coil occlusion was performed 7 days after the pCONUS HPC implantation. After coiling, a non-occlusive thrombus at the superior branch of the left MCA was observed (E, circle). Final run after an intravenous weigh-adapted bolus of eptifibatide showing its nearly complete disappearance (F). DWI obtained the following day showing no new HSI spots (compare D and G). Follow-up performed 163 days after treatment showed reperfusion of the aneurysm, which needed retreatment (H).
Patient 2 presented with an asymptomatic in-stent stenosis along the pCONUS HPC shaft at follow-up. The patient had been discharged with 100 mg ASA PO twice a day for 3 months following treatment. At follow-up, the medication was already reduced to 100 mg ASA PO daily. Insufficient inhibition for ASA was confirmed in the platelet function testing and the medication was again increased to twice-daily (figure 3). Patient 7 and 9 presented with asymptomatic stenosis in one of the efferent branches, which were protected with the pCONUS HPC device. No explanation for this phenomenon could be found.

{kind=link}
{kind=link}
{kind=link}
Posterior−anterior view of the right internal carotid artery showing an incidental wide-necked anterior communicating artery aneurysm (A). Three-dimensional reconstruction showing the aneurysm with a neck width of 5 mm (B). Dyna-CT reconstruction showing the position of a 4-15-6 mm pCONUS2 HPC within the aneurysm and along the right A1 segment (C). Procedure was performed under acetylsalicylic acid (ASA) as single antiplatelet therapy. Working projection for coil occlusion of the aneurysm 39 days after pCONUS HPC implantation (D). Final run after coiling of the aneurysm with small neck remnant visible (E). No high signal intensity spots were observed in the diffusion-weighted imaging performed the following day. Follow-up angiogram 8 months after coil occlusion (F,G) showed complete occlusion of the aneurysm and severe intimal hyperplasia along the stent-shaft (compare D and H). VerifyNow confirmed insufficient inhibition for ASA (ARU:569).
Discussion
Currently, improved endovascular techniques such as balloon-assisted coiling, stent-assisted coiling, and intra-saccular and extra-saccular flow diversion have facilitated the treatment of WNBA.13 However, due to the thrombogenic surface of vascular implants, DAPT is needed to prevent thromboembolic complications. Although DAPT has been shown to reduce thromboembolic events, it also leads to increased bleeding risk in patients with acutely ruptured aneurysms or in patients with pre-existing conditions, such as gastric ulcers, which is associated not only with higher mortality but also patient distress, inconvenience and premature discontinuation. Similarly, there is a requirement for patients to maintain their APT as well as potential drug interactions, which may interfere with the effectiveness.14
An individual selection of the APT is essential to reduce the risk of both thromboembolic and hemorrhagic complications as the individual variability of platelet reactivity is recognised as a risk factor for vascular events.15 16 Resistance to clopidogrel has been observed in approximately one-third of patients, and therefore there has been increasing interest in the efficacy of newer antiaggregation drugs, such as ticagrelor or prasugrel.17–19 These new drugs inhibit platelet aggregation more effectively and rapidly than clopidogrel, with lower rates of individual variability. However, the cost of medication (especially with prasugrel) and patient compliance (twice a day in the case of ticagrelor) have to be kept in mind.
The use of platelet function testing has been proposed as a possible solution to guarantee an appropriate level of platelet inhibition. VerifyNow (Accriva), Multiplate (Roche Diagnostics) and the Platelet Function Analyzer (PFA-100, Siemens, Erlangen, Germany) are the most widely used methods.20 Its clinical value, however, remains controversial.21
Therefore, the development of low-thrombogenic implants that would minimise the need for APT could be a milestone for the use of vascular implants. Although the coating materials developed to date for stents and FDS have shown biocompatible and hemocompatible properties, DAPT is still necessary.22 pHPC is a glycan-based hydrophilic polymer coating which can be applied to nitinol surfaces. It is intended to simulate the glycocalyx, a covering that can be found on the luminal surface of the endothelium, making the coated device hydrophilic and less thrombogenic.6 pHPC is a biocompatible coating that has no pharmaceutical effect, no evidence of acute inflammatory response, and does not interact with the physical properties of the metallic implant underneath.23 24
Until now, only the series of Aguilar-Perez et al have reported the use of this device in treating 15 ruptured aneurysms using ASA monotherapy. They reported three instances of intraprocedural thrombus formation and no hemorrhagic complications.8 In this series, all but two patients required increased doses of ASA to maintain adequate platelet inhibition. This preliminary data suggests that pHPC may play a role in the treatment of selected aneurysms which are not suitable for other interventions, but that adequate management of the SAPT prior to and after treatment must be meticulous. The increased platelet turnover created as a consequence of a stressful state may lead to increased dosages needed to maintain adequate platelet inhibition, as described in the series by Aguilar-Perez et al. Manning et al 25 reported the use of a twice-daily aspirin regimen since this may reduce complications due to platelet function recovery. Keeping this data in mind, we also used twice-daily 100 mg ASA in our series for at least for 3 months following treatment. One of our patients showed in-stent stenosis at angiographic follow-up. The patient was an active smoker and continued smoking after treatment. This state likely increased the platelet turnover as shown by the insufficient platelet inhibition at a daily dose of 100 mg ASA PO. We suggest that the dose of ASA should be kept at twice a day in patients with higher anticipated turnover, such as smokers or diabetics.26 27
Although the overall incidence of HSI on DWI following treatment of intracranial aneurysms is approximately 50%,28 this rate was higher in our series after the first intervention, ergo during stent implantation (82.8%). In contrast, we found a lower rate of DWI lesions after the second setting (61.5%), although four patients showed thrombus formation directly associated with the coil occlusion. A possible explanation for the higher rate of silent ischemic events during the stent implantation might be the lack of full heparinisation during our procedures. However, heparin alone is limited in preventing thromboembolic events following aneurysm coiling.29 Hahnemann et al 30 reported no significant difference in the incidence of DWI lesions in patients with and those without heparinisation in their series of 75 aneurysms treated with stent-assisted coiling under DAPT. Another explanation might be the deployment of the stent under ASA as SAPT. Although ASA has shown efficacy in reducing the risk of intraoperative thrombotic complications,31 32 Matsumoto et al 33 suggested that clopidogrel has a significant potential to inhibit platelet function more effectively. By extrapolating from Matsumoto’s paper we can suggest that any P2Y12 inhibitor has a greater potential to inhibit platelet function than ASA alone. In order to compare our recent pCONUS HPC data, we retrospectively reviewed our database and identified 15 patients that were treated with the uncoated pCONUS device for incidental WNBA in a sequential way. Microembolic lesions were noted in 10 of 15 patients (66.6%) after the first treatment and in 5 of 12 patients (three did not have postprocedural MRI) after the second setting (41.6%). However, all these procedures, as well as any stent-assisted coiling, were performed under DAPT, which has been demonstrated to significantly reduce the risk of thromboembolic complications associated with all kind of endovascular procedures.31 32
In a recently publicised study, pHPC has been shown to significantly reduce the thrombogenicity of the p48 FDS in an in vitro flow model.7 Similarly, we saw neither evidence of thrombus formation on the surface of the pCONUS HPC intraoperatively nor at follow-up angiography, suggesting that the origin of these HSI spots is more likely related to the deployment technique itself rather than the device’s thrombogenicity. However, the higher rate of DWI lesions observed in our series cannot be fully explained by the available data.
In view of the rate of intraprocedural thrombus formation and periprocedural DWI lesions in our series, we may assume that the use of the pCONUS HPC under DAPT or under a P2Y12 inhibitor such as Ticagrelor or Prasugel as SAPT might have less risk of thromboembolic complications than under ASA monotherapy. From this initial experience, we suggest the use of the device under DAPT during the perioperative period followed by ASA monotherapy, and keeping its use under SAPT for cases at higher risk under DAPT.
Bhogal et al 34 reported the use of the p48MW HPC FDS in treating five patients with unruptured aneurysms using prasugrel monotherapy. There were no thromboembolic complications but one patient suffered a minor hemorrhage from the aneurysm 2 weeks postoperatively.34 On the other hand, Aguilar Perez et al 35 reported the use of the p48MW in eight ruptured aneurysms using either ASA or prasugrel. They observed four intraprocedural thrombus formation and one stent-thrombosis on day 3, but none of the aneurysms rebled after treatment. They concluded that thromboembolic complications were a potential problem that may be more likely to occur under ASA rather than prasugrel since patients who received prasugrel showed less variability and failure in platelet inhibition before and after treatment.35
Regarding the pCONUS itself, it is unclear whether the device offers a benefit with respect to other treatment modalities such as microsurgery or other endovascular options, since the nature of the study does not allow for comparison. In our series, the rate of adequate occlusion (mRRC I or II) at follow-up was 80%. That our rate is higher than in Sorensen et al’s meta-analysis (60%) may be secondary to the staged treatment. However, our data do not allow us to conclude that a staged approach is superior as there was a higher rate of thromboembolic complications in our series than in others where the treatment was performed in a single session.1 8 Additionally, only 10 of our 15 patients were available for follow-up and this follow-up period was too short to provide any insight into whether residual or recurrent aneurysm formation can occur. Nevertheless, recurrent aneurysm perfusion prompting retreatment has been observed after coiling36 and has not been overcome with newer implants like the Woven EndoBridge (WEB; MicroVention, Aliso Viejo, California, USA).37 However, it is critical to continue to advance endovascular technology, as not all patients are candidates for microsurgery.
Our study has several limitations, including the single-centre retrospective design as well as the relatively small number of patient and the short follow-up period. There were no ruptured aneurysms included and all patients in our series were treated in a staged way, which was a potential source of increased complications. This data are considered preliminary, and further investigation is required to evaluate the safety of SAPT in the context of pCONUS HPC-assisted coiling in selected cases of unruptured aneurysms.
Conclusions
This early experience on the use of the pCONUS HPC under ASA as SAPT suggests that it may be useful for treating selected cases of unruptured WNBA not suitable for other interventions. Larger registries and randomised controlled trials with larger cohorts and longer follow-up periods are underway.
Acknowledgments
The authors are grateful to our stroke and study nurse C Knispel for the tireless collection of clinical data. Only the expert technical support by CTress and her colleagues makes our service possible.
References
Footnotes
Contributors MAP: data gathering, manuscript preparation. CSC and VH: data gathering. CW, OG, HB: review, editing. HH: guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MAP has proctoring and consultancy agreements with phenox; VH has consultancy agreements with phenox; HH is co-founder and shareholder of phenox.
Patient consent for publication Not required.
Ethics approval The responsible local ethics committee approved the retrospective collection, evaluation, and publication of the concerning data (Reference Nr.: F-2019-023). Informed consent was obtained from all patients included in the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.