Article Text

Abstract
Coronavirus disease 2019 (COVID‐19) has become a pandemic disease globally. Although COVID-19 directly invades lungs, it also involves the nervous system. Therefore, patients with nervous system involvement as the presenting symptoms in the early stage of infection may easily be misdiagnosed and their treatment delayed. They become silent contagious sources or ‘virus spreaders’. In order to help neurologists to better understand the occurrence, development and prognosis, we have developed this consensus of prevention and management of COVID‐19. It can also assist other healthcare providers to be familiar with and recognise COVID-19 in their evaluation of patients in the clinic and hospital environment.
- brain
- infection
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The 2019-novel coronavirus (2019-nCoV) has been declared a world pandemic by WHO on 11 March 2020.1 Clinical symptoms of 2019-nCoV have mostly resembled that of severe acute respiratory syndrome coronavirus (SARS-CoV) of 2003. Both shared the same receptor, angiotensin converting enzyme 2 (ACE2).2 Therefore, this virus was named SARS-CoV-2. By 28 March 2020, a total of 593 735 SARS-CoV-2 infected cases have been confirmed in 200 countries worldwide. In addition to the respiratory system involvement, recent evidence has shown that SARS-CoV-2 can affect other organ systems including nervous, vascular, digestive, urinary, haematological and so on.3 4 The pathological findings confirmed the nature of multiorgan damaged by SARS-CoV-2, which include pulmonary lesion and cerebral oedema, microvascular steatosis and thrombosis.5 Neurological symptoms can be trivial or non-specific at the early stage of the COVID-19 infected patients, which have often been delayed and misdiagnosed and led to inappropriate management. These patients then become silent contagious sources or ‘virus spreaders’. Although neurological involvement is uncommon in patients with COVID-19, it can be seen in those with severe infection and the patients may manifest as acute cerebrovascular diseases, impaired consciousness or encephalopathy, and skeletal muscle injury.6
In order to help neurologists to understand the occurrence, development and outcome of this disease and be familiar with its diagnosis and treatment process, we present this ‘Consensus for prevention and management of coronavirus disease 2019 (COVID-19) for neurologists’. In this consensus, we summarised the current clinical guidelines and research progress on the management of COVID-19 and emphasised on its neurological manifestations. We hope that this consensus statement can help all recognise the infection early and protect the providers and healthcare environment.
Overview of the novel coronavirus
Coronaviruses (CoVs)
CoVs are enveloped viruses with a single-strand, positive-sense RNA genome, which are separated into four genera based on phylogeny: alpha-CoV (group 1), beta-CoV (group 2), gamma-CoV (group 3) and delta-CoV (group 4). CoVs was first isolated from domestic animals in 1937. The first human coronavirus was isolated from the nasal discharge of patients in 1965. In humans, CoVs infections primarily involve the upper respiratory and gastrointestinal tracts. Under the electronic microscope, there are many evenly arranged protrusions on the surface of viral particles. The entire virus particle resembles a ‘crown’ of a medieval European emperor. Hence, it was given the name of ‘coronavirus’. A coronavirus particle is usually enclosed by an envelope, and its membrane surface has three proteins: spike (S), envelope (E) and membrane (M). Protein spike (S), projecting from the virus membrane and resembling a crown, is the key structure for its infectivity and pathogenicity. These spikes can recognise and bind to receptors on the surface of host cells and subsequently invade the host cells.7
Severe acute respiratory syndrome coronavirus 2
SARS-CoV-2, the β-type novel coronavirus, is one of the viruses that exists in the form of RNA with a total of 29 000 nucleotide bases. These bases preserve the genetic information for its reproduction. Genomic sequence analysis of SARS-CoV-2 has been published on virological.org, nextstrain.org, bioRxiv and other academic journals. In early February of 2020, Chinese researchers shared the total sequences of this new type of virus so they can be used by other researches around the world. SARS-CoV-2 virus sequence is highly homologous to that of bat coronavirus (96.2% similarity). The entire bat coronavirus genomic sequence has 79.5% homology to SARS coronavirus.8
SARS-CoV-2 spike protein and HIV gp120 protein are both recognition proteins on the membrane surface, but their pathogenic mechanisms are quite different. The spike protein enables SARS-CoV-2 to identify ACE2 receptors in the mucosal epithelium and invade. However, the gp120 protein in HIV allows HIV to recognise the CD4 receptor and invade CD4+ T cells.2 There is currently no evidence indicating that SARS-CoV-2 is capable of invading T cells, any cells that express CD4 or any cells that do not express ACE2. SARS-CoV-2 does not invade cells that are not prone to infection by other known coronaviruses.
So far, the reported SARS-CoV-2 sequences in Global Initiative of Sharing All Influenza Data and GenBank database have a maximum of 10 nucleotide differences from the earliest SARS-CoV-2 sequence in Wuhan9 to the latest sequence worldwide including Europe, USA and so on, suggesting that SARS-CoV-2 entered human body recently.
Route of transmission
Although SARS-CoV-2, SARS and Middle East respiratory syndrome coronaviruses belong to the same large family of coronaviruses, their genetic characteristics are significantly different. For COVID-19, transmission through respiratory droplets and contact are the main routes of transmission. It has also been confirmed that live virus and virus nucleic acid can be detected in human stool.10 Thus, we speculated that the digestive tract might be another transmission route. Moreover, SARS-CoV-2 can be transmitted through aerosols under a prolonged exposure in a relatively closed environment.
Clinical characteristics and manifestations
COVID-19 is highly contagious and has a long latency period. The incubation period is generally 3–14 days, but the most extended period was reported to be 24 days.11 12 Local news in Wuhan has reported a case of asymptomatic SARS-CoV-2 infection that had a 38-day incubation period. People who have visited the epidemic area or have a contact history with patients or suspected cases should consider self-quarantine and closely monitor body temperature and related symptoms.
Systemic and respiratory symptoms
Patients with COVID-19 often have a fever, dry cough and fatigue as the primary manifestations, and in some patients, pharyngeal pain, abdominal pain, diarrhoea and conjunctivitis are common. Therefore, if a patient has any of these symptoms, even if the symptoms are mild, testing for COVID-19 is recommended.
Neurological symptoms and signs
Neurological symptoms have been observed in patients with COVID-19.6 It has been reported that more than one-third of patients experienced various neurological symptoms including the involvement of central nervous system (dizziness, headache, impaired consciousness, acute cerebrovascular disease, ataxia and epilepsy), peripheral nervous system (taste impairment, smell impairment, vision impairment and neuralgia) and skeletal muscular damage. Skeletal muscle injury was defined when a patient had skeletal muscle pain and elevated serum creatine kinase level above 200 U/L.6 12 In patients with central nervous system manifestations, the most common complaints were dizziness and headache. In patients with peripheral nervous system manifestations, the most common complaints were taste and smell impairment.
The nervous system manifestations were significantly more common in patients with severe infection, manifested as ischaemic stroke and cerebral haemorrhage diagnosed by clinical symptoms and head CT, impaired consciousness and skeletal muscle injury.6 Rapid clinical deterioration or worsening could be from a neurological event such as stroke, which may have contributed to its high mortality rate. The main reason of clinical worsening is the hyperactivation of inflammatory factors that eventually causes a fatal inflammatory storm as the disease progresses. In addition, coagulation system is damaged causing the D-dimer and platelet abnormalities, which increases the risk of cerebrovascular disease. During the epidemic period of COVID-19, when seeing patients with above neurological manifestations especially more develop nervous system manifestations, doctors should consider SARS-CoV-2 infection as a differential diagnosis so to avoid misdiagnosis and seize the opportunity of stopping it from infecting the others.
Issues require special attention in laboratory inspection
Most patients with COVID-19 have a low grade fever, but a few would have high temperature. It is worth noting that some patients may have difficulty breathing. In some patients, their lung CT scans may have signs of severe damage from the infection, but their temperature remain within normal limit. In these patients, feeling weak or exhaustion was their main complaint. In other patients, their temperature may drop, but their pneumonia actually progressed. Therefore, to judge the progression of the disease, lung CT is essential (figure 1).
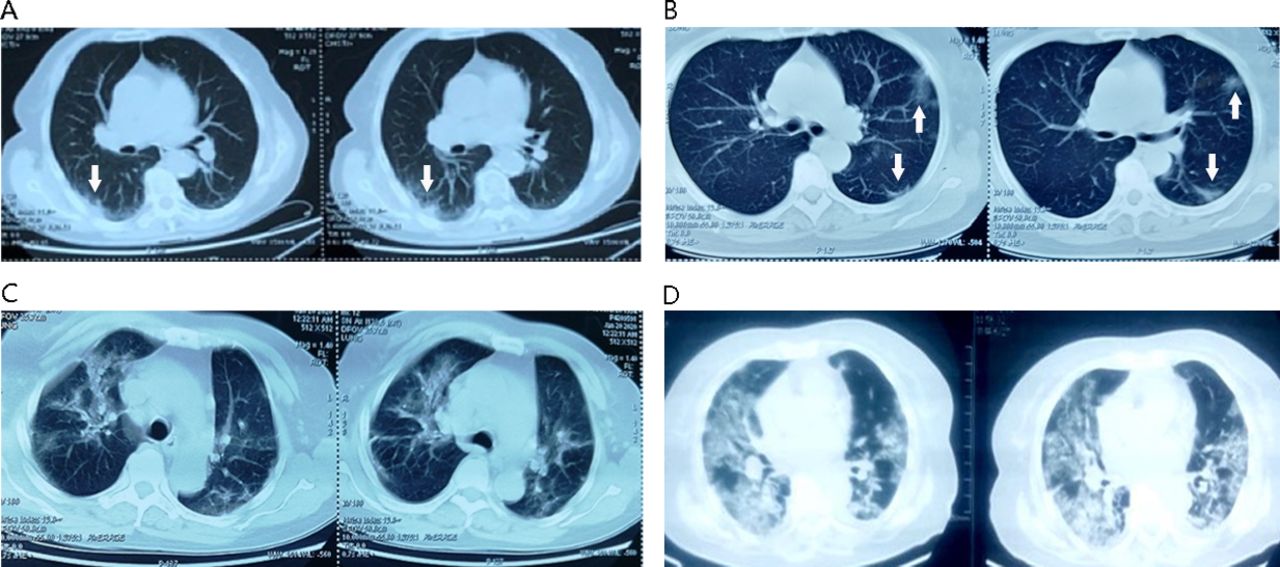
Pulmonary progress on axial chest CT. (A) During the first few days, a single lesion; (B) during the first week, multiple lesions; (C) during the first and second week, nearly 50% involvement of bilateral lungs; (D) after the second week, diffuse lesion of bilateral lungs. Arrows indicate the infected area.
In laboratory examinations, their premorbid routine blood test may show lymphopaenia. Recently, some companies have developed a SARS-CoV-2 antibody test, and its use for clinical monitoring is being studied. These laboratory findings and parameters may serve as a biomarker bearing a value relevant to the prognostic perspective.
At present, nucleic acid testing for SARS-COV-2 is still the essential criterion and gold standard for confirming the diagnosis. However, its sensitivity is low and repeated tests may often be needed. Therefore, the current consensus is that a COVID-19 infected individual may present asymptomatically or symptomatically with or without abnormal laboratory findings and lung changes on CT and an unrevealing nucleic acid test. The diagnosis can be confirmed if there are apparent characteristic changes on lung CT or a positive IgM test for viral antibody. Clinically suspected patients should not be left untreated with SARS-COV-2 infection while waiting for the nucleic acid test result or if nucleic acid test was negative initially.
Current COVID-19 management and key points for prevention and treatment in China
Key points for the treatment of COVID-19 from the Chinese guideline
Based on the ‘Diagnosis and treatment of the novel coronavirus pneumonia (Trial version 7)’ published by the National Health Commission of the People’s Republic of China,11 the following features need to be noted in the prevention and treatment process:
During the first few days, patients with mild infection should be treated as soon as possible with Arbidol (umifenovir hydrochloride), chloroquine phosphate or other drugs recommended by ‘Diagnosis and treatment of the novel coronavirus pneumonia (Trial version 7)’.11 Timely treatment may offer relief within a few days.
Around 3–7 days, if the symptoms are worsening, these patients should have their chest CT repeated to look for any progression of lung infection. For older patients and those with comorbidities, clinicians should pay more attention to possible secondary infection. These patients should be treated quickly in order to halt the progression.
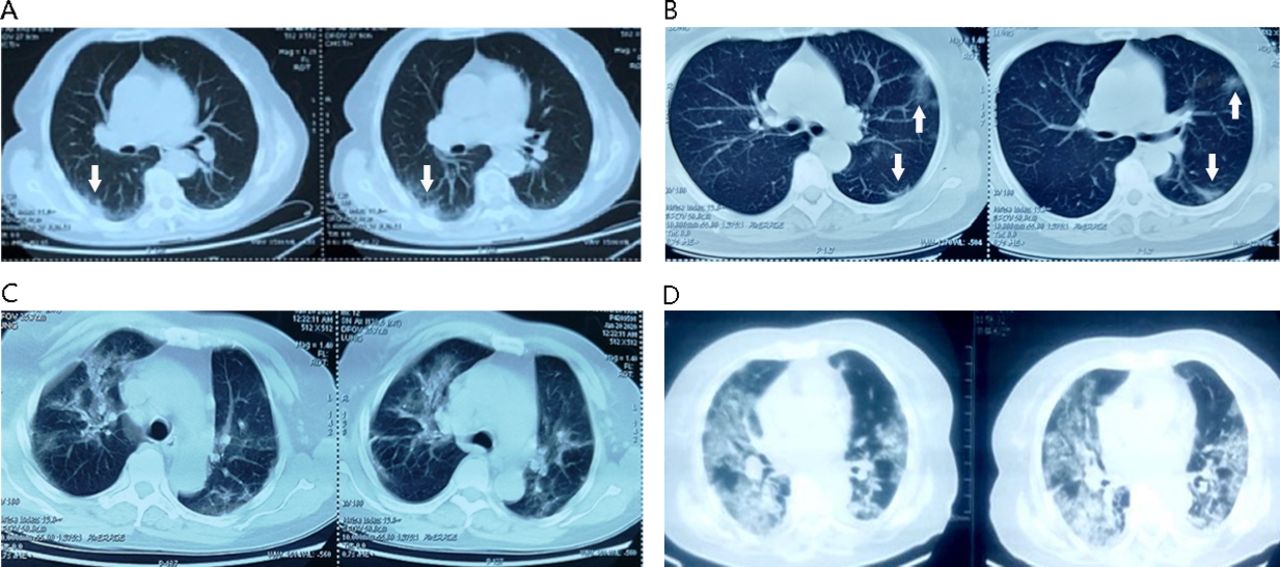
Around 10 days, a few patients may continue to deteriorate. Their chest CT may begin to show multiple lesions and the expansion of the existing damage to over 50% of lung area. Most patients with severe infection may have additional serious secondary infections or multiple infections such as combining with bacterial or mycotic infection. Some may develop acute cerebrovascular disease, which could account for sudden clinical worsening (figure 2). During this period, increased inflammatory response and blood coagulation abnormalities could be the main causes of clinical worsening. These patients are more likely to convert into critical stage. Someone has tried to use the immune modulation treatment, including small doses of methylprednisolone, gamma globulin, haemodialysis and anticoagulation, and found that was effective.
A few weeks later and if the infection is still progressing, the treatment of these critically ill patients would become difficult and the mortality rate becomes high.

{kind=link}
{kind=link}
Brain CT and chest CT images from a critically ill patient with COVID-19. (A) Brain CT showing cerebral infarction. Arrows indicate the infarction area. (B) Diffuse lesion of bilateral lungs from the same patient.
Possible causes of neurological symptoms and precautions for neurologists
Symptoms related to the development of acute cerebrovascular diseases
Among patients with SARS-CoV-2 infection, middle-aged and elderly people accounted for the majority of strokes, especially in critically ill patients. Serum D-dimer level is generally increased, which could be the source of embolic vascular events.11 ,12 Many of these patients may already have other cerebrovascular risk factors, such as hypertension, diabetes mellitus, hyperlipidaemia, smoking or previous stroke history. Some may develop their first-ever acute ischaemic stroke.6 Therefore, medical staff should pay close attention to the manifestation of neurological symptoms. If an acute ischaemic stroke patient with suspected or confirmed diagnosis of COVID-19 are admitted, emergency treatment should be jointly offered by neurologists and infectious disease specialists. For ischaemic stroke patients with a high D-dimer level, preventive anticoagulation is recommended. These patients should be transferred to the isolation ward, and neurologists would assist in the management.
Since SARS-CoV-2 specifically binds to ACE2 receptors,2 patients with hypertension may encounter blood pressure fluctuations following SARS-CoV-2 infection, which may increase the risk of intracranial haemorrhage. Furthermore, some critically ill patients with SARS-CoV-2 infection have severe thrombocytopaenia, another high-risk factor for cerebral haemorrhage. For hypertensive patients with SARS-CoV-2 infection, it is recommended to stop using ACE inhibitors or angiotensin ΙΙ receptor blockers (ARBs) as antihypertensive drugs, and consider calcium channel blockers, diuretics and other classes of antihypertensive drugs.
Symptoms related to intracranial infection
Based on the previous discovery, coronavirus may invade the central nervous system. Researchers have detected SARS coronavirus nucleic acid in patients’ cerebrospinal fluid, and SARS coronavirus was also verified in brain tissue on autopsy.13 14 For this SARS-CoV-2 outbreak, some patients have had symptoms similar to those with intracranial infections such as headache, seizure and disturbance of consciousness. Few patients had central nervous system symptoms before having pulmonary symptoms.6 Therefore, neurologists should be vigilant when seeing COVID-19 infected patients and look for any signs suspicious for intracranial infection, and if possible, MRI of head with and without contrast should be performed. A lumbar puncture to look for SARS-CoV-2 nucleic acid by using PCR is recommended. For these COVID-19 patients with intracranial infection, treatment strategies such as controlling cerebral oedema, treating and preventing seizures and treating psychotic symptoms should be considered and the guidelines should be followed.
Symptoms related to muscle damage
Historically, SARS coronavirus was involved in the myocardial inflammation.15 In clinical observation, some patients with COVID-19 may experience symptoms of skeletal muscle damage, such as fatigue or limb aches, and mild elevation of serum creatine kinase level.6 They are due to inflammatory reaction caused by the SARS-CoV-2 infection or direct muscle damage by the virus. For patients with muscle damage symptoms, screening for SARS-CoV-2 infection is recommended. In addition to active treatment of COVID-19, strengthening nutritional support is recommended.
Precautions for neurologists
In this outbreak, patients with COVID-19 can begin with neurological symptoms or develop neurological complications during the treatment. Neurologists may see these patients in the clinic, emergency room and in-patient ward. According to the ‘Technical guidelines for prevention and control of new coronavirus infection in medical institutions (First Edition)’16 developed by General Office of the National Health Commission of the People’s Republic of China and clinical characteristics of these patients, we propose the following precautions for neurologists, especially for those who are working in high-risk areas.
Cautions in neurology clinic
Neurologists need to wear disposable work caps, medical protective masks, work clothes such as scrubs, disposable latex gloves and carry hand sanitiser that contains ethanol, hydrogen peroxide or sodium hypochlorite.
Patients and their companions must have temperature measured in triage routinely before entering the consulting room. To reduce cross-infection, companions should avoid entering the room. Everyone must wear disposable medical masks.
For patients with neurological symptoms but also highly suspicious of COVID-19, it is recommended that the patient go to a fever clinic first and consult a neurologist later.
After work, doctors should remove the protective gear step by step according to the decontamination protocol. It is forbidden to leave the contaminated area wearing personal protective equipment for the purpose of preventing cross-infections.
Management in neurological emergency and staffing acute stroke green pathway 17
The protection level in the emergency room and stroke green pathway should be at least at level 2: wearing working clothes and caps, medical protective masks, goggles/face shields and disposable isolation gown. When treating suspected or confirmed cases of COVID-19 or patients with close contact history, the protection level should be appropriately raised: wearing medical protective masks, goggles/face shields, disposable medical protective clothing, disposable latex gloves and long shoe covers.
Neurological emergency and stroke green pathway (including consultation rooms, CT/MRI rooms, interventional operating rooms and so on) should be strictly separated from routine emergency and fever clinics to ensure no direct interaction with a patient with fever.
Doctors should ask patients and their companions whether they have typical symptoms of COVID-19, such as fever, sore throat and so on, within 14 days of exposure or a contact history with suspected or confirmed cases. Patients should have a chest CT at the same time of having a head CT. In any suspected conditions, a specialised medical staff should accompany the patient to the fever clinic and carry out stroke triage/emergency treatment in the fever clinic. The patient should be admitted to an isolation ward after treatment. Patients without suspected situations can be admitted to a buffer ward to receive the next treatment and do further screening for COVID-19 at the same time. A neurologist should round on these patients regularly. Patients will be transferred to the general ward of neurology only when COVID-19 has been definitely ruled out.
Patients who receive thrombolysis or thrombectomy should avoid entering the neurological intensive care unit and should be treated in a private room first. Medical staff should pay close attention to those in isolation. If the body temperature (monitoring at least for 3 days), blood routine, chest CT and SARS-CoV-2 nucleic acid tests are negative, the patient can be transferred to a semiprivate or multiperson ward.
Medical staff treating neurological emergency and responsible for acute stroke green pathway must have a good work/life balance, avoid long working hours and sleep deprivation. Appropriate exercises and nutritional support are also very important to fend off infections.
Management in neurology wards
During the epidemic period or working in areas with high risk of COVID-19, medical staff in general wards should wear disposable work caps, medical protective masks and work clothes. It is recommended that to assess and treat those with severe infection in an intensive care unit (ICU), a team of two should be organised to enter the areas and depart together. Forming such partnership can help healthcare providers to look out for and assist each other. In case one healthcare provider feels ill, which make him unable to continue to work in the ICU, the other one can help evaluate and evacuate.
Only one family companion is permitted for each patient, and the companion must have had the same screening tests to exclude COVID-19 before entering the ward. A guard at the entrance of the ward is needed to take the temperature of anyone entering the ward. All people in the ward must wear disposable medical masks to avoid cross infection.
Everyone in the ward should monitor body temperature regularly. Patients and their companions should have COVID-19 screening test every few days until discharge. Once a person with fever has been identified, medical staff should notify the prevention and control team of the hospital immediately, then assist the treatment, examination, isolation and disinfection of wards.
If a highly suspected case has been identified during the monitoring, doctors should notify the prevention and control team and arrange for an in-hospital COVID-19 specialist consultation immediately. Other patients, their companions and medical staff who came in contact with should be separated. The temperature and COVID-19 related symptoms of all contacts should be closely monitored. The patient should be temporarily taken to a separate room and then quickly transferred to the isolation ward or a designated hospital once the diagnosis has been confirmed. The space where the patient stayed must be disinfected strictly.
Conclusion
COVID-19 is a highly contagious disease that has become a worldwide pandemic. Patients infected may show neurological symptoms first. Healthcare providers and neurologists should pay close attention to these symptoms and have a high index of suspicion when evaluating patients in an endemic area. Early recognition may help initiate treatment and isolation early so to prevent clinical worsening and spreading of virus.
Footnotes
Collaborators Kangning Chen (ckn_640827@126.com, Department of Neurology, The Southwest Hospital, the First Affiliated Hospital of Third Military Medical University, Chongqing, China), Liying Cui (pumchcuily@sina.com, Department of Neurology, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, China), Qiang Dong (dong_qiang@fudan.edu.cn, Department of Neurology, Huashan Hospital, Fudan University, Shanghai, China), Chuanqiang Pu (pucq30128@sina.cn, Department of Neurology, The General Hospital of Chinese People’s Liberation Army, Beijing, China), Furong Wang (wangfurong.china@163.com, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China), Yongjun Wang (yongjunwang@ncrcnd.org.cn, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China), Bo Xiao (xiaobo_xy@126.com, Department of Neurology, Xiangya Hospital, Central South University, Changsha, China), Peng Xie (xiepeng@cqmu.edu.cn, Department of Neurology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China), Anding Xu (tlil@jnu.edu.cn, Department of Neurology and Stroke Center, the First Affiliated Hospital, Jinan University, Guangzhou, China), Yun Xu (xuyun20042001@aliyun.com, Department of Neurology, Drum Tower Hospital, Medical School of Nanjing University, Nanjing, China), Qingwu Yang (yangqwmlys@163.com, Department of Neurology, Xinqiao Hospital, Third Military Medical University, Chongqing, China), Jinsheng Zeng (zengjs@pub.guangzhou.gd.cn, Department of Neurology and Stroke Center, the First Affiliated Hospital of Sun Yat-Sen University, Guangdong, China), Junjian Zhang (wdsjkx@163.com, Department of Neurology, Zhongnan Hospital of Wuhan University, Wuhan, China), Zhaohui Zhang (zhzhqing1990@163.com, Department of Neurology, Renmin Hospital of Wuhan University, Wuhan, China) and Gang Zhao (zhaogang@fmmu.edu.cn, Department of Neurology, Xijing Hospital, The 4th Military Medical University, Xi’an, China).
Contributors BH and LW designed the framework and also participated in revision. HJ drafted the sections of key points for the treatment of coronavirus disease 2019 (COVID-19) and revised the whole manuscript. CH drafted the sections of precautions for neurologists. SC drafted the sections of clinical characteristics of COVID-19. YZ drafted the sections of introduction and the overview of the novel coronavirus. YW drafted the sections of possible causes of neurological symptoms and precautions in treatment. LM, YL, QH, ML, YS and DW revised the whole manuscript.
Funding This work was supported by the National Key Research and Development Program of China (No. 2018YFC1312200 to BH), the National Natural Science Foundation of China (No. 81820108010 to BH, No. 81974182 to LM and No. 81671147 to HJ) and major refractory diseases pilot project of clinical collaboration with Chinese and Western Medicine (SATCM-20180339).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.