Article Text

Abstract
Background and purpose Functional outcomes after ischaemic stroke are worse in women, despite adjusting for differences in comorbidities and treatment approaches. White matter microvascular integrity represents one risk factor for poor long-term functional outcomes after ischaemic stroke. The aim of the study is to characterise sex-specific differences in microvascular integrity in individuals with acute ischaemic stroke.
Methods A retrospective analysis of subjects with acute ischaemic stroke and brain MRI with diffusion-weighted (DWI) and dynamic-susceptibility contrast-enhanced (DSC) perfusion-weighted imaging obtained within 9 hours of last known well was performed. In the hemisphere contralateral to the acute infarct, normal-appearing white matter (NAWM) microvascular integrity was measured using the K 2 coefficient and apparent diffusion coefficient (ADC) values. Regression analyses for predictors of K 2 coefficient, DWI volume and good outcome (90-day modified Rankin scale (mRS) score <2) were performed.
Results 105 men and 79 women met inclusion criteria for analysis. Despite no difference in age, women had increased NAWM K 2 coefficient (1027.4 vs 692.7×10–6/s; p=0.006). In women, atrial fibrillation (β=583.6; p=0.04) and increasing NAWM ADC (β=4.4; p=0.02) were associated with increased NAWM K 2 coefficient. In multivariable regression analysis, the K 2 coefficient was an independent predictor of DWI volume in women (β=0.007; p=0.01) but not men.
Conclusions In women with acute ischaemic stroke, increased NAWM K 2 coefficient is associated with increased infarct volume and chronic white matter structural integrity. Prospective studies investigating sex-specific differences in white matter microvascular integrity are needed.
- stroke
- leukoaraiosis
- MRI
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sex disparities in acute ischaemic stroke (AIS) outcomes represent an important clinical issue. Compared with men, women have worse functional outcomes.1 2 Women are known to be older at the time of stroke,3 have higher rates of antecedent disability and atrial fibrillation,2 and lower rates of treatment with thrombolytic therapy.4 Even after adjusting for these differences, however, functional outcomes are worse in women.5 Understanding the factors that contribute to this sex disparity in stroke outcomes represents an opportunity to improve patient care and stroke outcomes.
The decreased structural integrity of cerebral white matter and increased blood–brain barrier (BBB) permeability are factors that negatively affect poststroke outcomes.6–9 Evidence of cerebral microvascular dysfunction can be detected on T2-weighted MRI as white matter hyperintensities (WMH), enhanced BBB permeability on perfusion-weighted imaging (PWI), or measured in normal-appearing white matter (NAWM) as loss of microstructural integrity on diffusion-tensor imaging (DTI), and reflected as an increase in the apparent diffusion coefficient (ADC) values.7 10 Both increased diffusivity and BBB permeability have been linked to poor outcomes after AIS,6–8 with a potential sex-specific contribution.11 We have also reported a novel association between increasing NAWM K 2 coefficient, as a potential surrogate of BBB permeability, and worse functional outcomes after AIS.7 Two important findings were observed in that analysis: (1) increased NAWM K 2 coefficient in women compared with men and (2) increased matrix metalloproteinase-2 (MMP-2) levels, as a measure of acute BBB disruption,12 were associated with worse long-term outcomes. The underlying aetiology of these sex-specific differences in BBB permeability and influences on ischaemic tissue and functional outcomes, however, was unclear.
In this study, we evaluated sex-specific clinical and radiographic variables associated with NAWM K 2 coefficient and their impact on infarct volume and 90-day functional outcomes after AIS.
Methods
Standard protocol approvals, registrations and patient consents
This study and the use of human participants was approved by the local Institutional Review Board. Written informed consent was obtained from all participating subjects or their surrogates.
Subjects and inclusion/exclusion criteria
We performed a retrospective analysis of a prospective biomarker cohort study of consecutive adult AIS subjects admitted between February 2007 and 2011 (National Institutes of Health Specialized Program of Translational Research in Acute Stroke).13 14
All subjects presenting to two academic medical centres within 9 hours of the last known well (LKW) and with signs and symptoms of AIS were screened for eligibility. To be eligible for inclusion in this study, subjects were required to undergo brain MRI within 9 hours from LKW containing diffusion-weighted imaging (DWI), dynamic-susceptibility contrast (DSC) perfusion-weighted MRI, and fluid-attenuated inversion recovery (FLAIR) MRI sequences; have a confirmed acute infarct on DWI; and have plasma MMP-2 levels collected at the time of study enrollment. We excluded patients with artefactual MMP-2 recordings and those with acute infarcts in both hemispheres.
Clinical assessments
Age, medical history and antecedent medications were obtained from the subject or their surrogates or otherwise from the review of the medical record at the time of admission. Admission systolic and diastolic blood pressures were acquired from the first documented vital signs. Treatment with intravenous alteplase was recorded. Tobacco use was dichotomised as current or past use versus never. Alcohol use was defined and dichotomised as current versus none. Anticoagulant use was defined as prehospital use of lovenox or coumadin.
Imaging analysis
MRI protocol
The majority of MRIs were performed on a 1.5T General Electric Signa HDx scanner with the following acquisition parameters. DTI: repetition time (TR)/echo time (TE)=5000/85.3 ms, 220 mm field-of-view, 5 mm slice thickness with 1 mm gap, in-plane resolution of 0.86×0.86 mm2 (128×128 acquisition matrix up-sampled to 256×256), three 0 s/mm2 (b-zero) and 1000 s/mm2 in 25 directions. FLAIR: TR/TE/TI=10 002/145/2200 ms, 220 mm field-of-view, 5 mm slice thickness with 1 mm gap, and in-plane resolution of 0.86×0.86 mm2. For 10 subjects, FLAIR scans were acquired at a separate time from the original DWI and DSC sequences due to an unavailable or unusable FLAIR scan on the original MRI. DSC: 80 acquisitions, TR/TE=1500/40 ms, 220 mm field-of-view, 5 mm slice thickness with 1 mm gap, 1.72×1.72 mm2 in-plane resolution. DSC sequences were acquired using bolus tracking of a single dose of gadolinium-based contrast agent (0.1 mmol/kg) administered with a power injector. Motion and eddy current distortions were corrected in all DTI datasets and the ADC maps were then derived from the high-b-value and low-b-value DTI sequences.15
To estimate BBB permeability, the K 2 coefficient (/s) was mathematically derived from the concentration-time curves using the Boxerman-Weisskoff model.16 In brief, the effective transverse relaxation rate due to the contrast agent, a parameter representing the per voxel concentration of contrast agent, is represented as:

A least-squares fit to this equation can subsequently be used to solve for the K 2 coefficient on a voxelwise basis.
Mean transit time (MTT) maps were calculated from deconvolved DSC data converted to concentration changes over time using a tracer arrival timing-insensitive technique.17 18
Volumetric lesion mapping
The DWI and MTT lesions were outlined using an intensity threshold-based method. All DWI lesions were cross-referenced to ADC maps to exclude subacute and chronic infarcts as well as infarcts involving the bilateral cerebral hemispheres. The acute infarct volume and ipsilateral perfusion deficit, assessed on DWI sequences (DWIv) and MTT maps (MTTv), respectively, were calculated semiautomatically using MRIcro software (University of Nottingham School of Psychology, Nottingham, UK; www.mricro.com).
WMH lesions in the hemisphere contralateral to the acute infarct were outlined in a semi-automated manner using MRIcro software as described previously.11 19 All images were analysed by trained research staff that were blinded to all outcome data.
NAWM segmentation and analysis
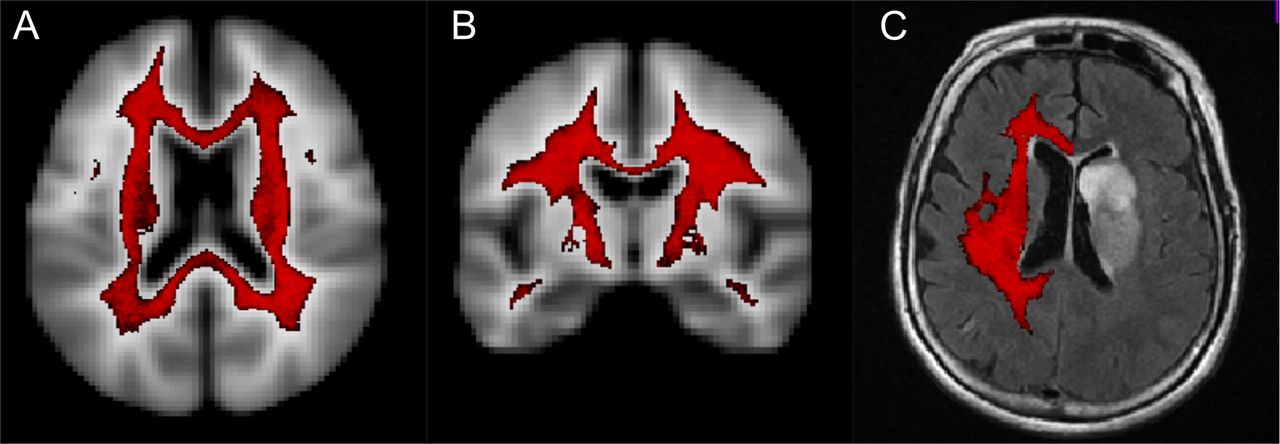
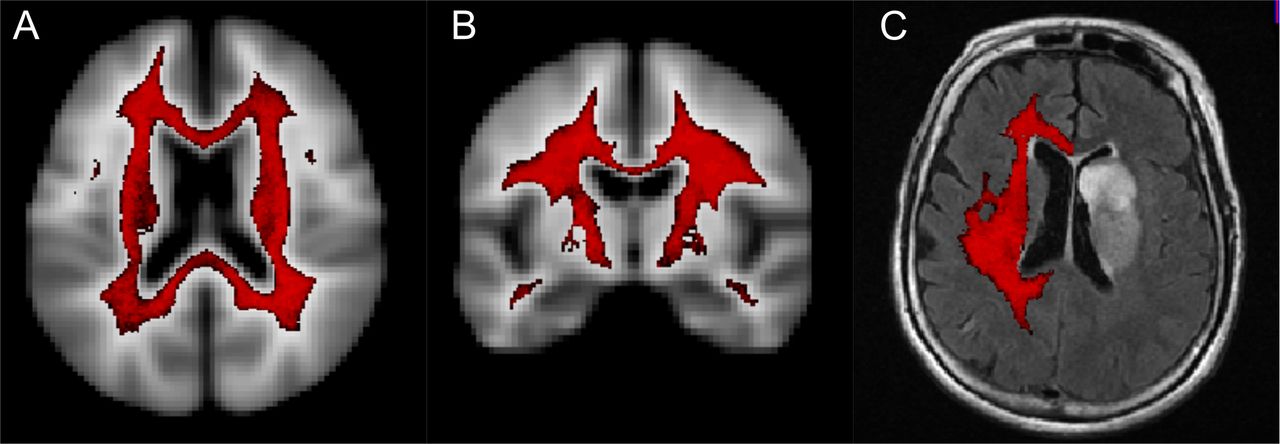
NAWM segmentation in the contralateral hemisphere was performed as described previously (figure 1).7 The mean ADC and K 2 coefficients were measured in contralateral NAWM as defined by the probabilistic mask.
{kind=link}
NAWM segmentation. (A) Axial and (B) coronal views of probabilistic white matter mask with threshold of >95% probability white matter (red) superimposed on the International Consortium for Brain Mapping 425 atlas. (C) Representative image of final contralesional normal-appearing white matter mask (red) overlaid on FLAIR image.
Stroke and outcomes assessment
All subjects were evaluated at the time of admission by a trained neurologist and stroke severity was determined using the National Institutes of Health Stroke Scale (NIHSS). Stroke subtype was categorised according to the Causative Classification of Stroke System (CCS) score.20 Haemorrhagic transformation was defined as the presence of any petechial or parenchymal haematoma on follow-up CT or MRI (obtained within 48 hours of LKW). Functional outcome at 90 days was measured using the mRS score, which was obtained either through an in-person or validated telephone-based interview.21 Good functional outcome was defined as a 90-day mRS score of <2.
Statistical analysis
WMH volume (WMHv) and DWI volume (DWIv) were normalised to the intracranial area.22 Univariable analysis was performed using linear regression to determine factors associated with K 2 coefficient and DWIv and logistic regression to evaluate factors associated with good functional outcome. Variables that displayed an association, a priori set at p<0.05, in univariable analysis were inserted into a backward stepwise elimination multivariable regression model. To minimise influences of collinearity, WMHv and NAWM ADC, as markers of global structural integrity, were input into separate multivariable regression models when significant in univariable analysis. Admission NIHSS was excluded from multivariable regression models for DWIv and good outcomes due to the known strong association between NIHSS and DWIv.23 24 Statistical significance was set at a p value of<0.05.
Results
A total of 105 men and 79 women met inclusion criteria for analysis in this study. The baseline demographics are shown in table 1. Women were more likely to have atrial fibrillation and cardioembolic strokes. Men had a greater incidence of hyperlipidaemia and strokes attributed to large-artery atheroembolism. Treatment rates with intravenous alteplase were similar between men and women and only one patient in the cohort underwent intra-arterial therapy. There was no difference in WMHv, DWIv, MTT volume or NAWM ADC between men and women. Women, however, had significantly greater NAWM K 2 coefficient (table 1).
Comparison of admission and clinical variables in men and women with AIS
In women, WMHv, NAWM ADC and atrial fibrillation were associated with greater NAWM K 2 coefficient in univariable linear regression analysis (table 2). In multivariable analyses, increasing NAWM ADC was associated with increased NAWM K 2 coefficient in women, whereas WMHv was not (table 3). In contrast, in men, WMHv and age were associated with NAWM K 2 coefficient in univariable linear regression but only WMHv remained an independent predictor in the multivariable analysis (table 3). In the entire cohort, we observed no association between strokes attributed to large-artery atheroembolism (β=75.0; p=0.84) or cardioembolism (β=163.1; p=0.58) and the NAWM K 2 coefficient.
Univariable analysis of sex-specific associations with NAWM K 2 coefficient
Multivariable backward stepwise elimination linear regression analysis for sex-specific predictors of NAWM K 2 coefficient
In both men and women, the admission NIHSS was a significant predictor of DWIv in univariable analysis (table 4). In women, administration of intravenous alteplase, haemorrhagic transformation and increasing NAWM K 2 coefficient were independently associated with DWIv. In comparison, in men, only atrial fibrillation was associated with increased DWIv. Subsequent linear regression analysis including sex, NAWM K 2 coefficient and an interaction term (male sex · NAWM K 2 coefficient) showed that NAWM K 2 coefficient (β=0.006; p=0.037) and the interaction term (β=−0.007; p=0.027) were independent predictors of DWIv for the entire cohort.
Sex-specific associations with acute infarct volume
In multivariable logistic regression analysis, increasing NAWM ADC was an independent predictor of the decreased likelihood of good outcome for both sexes (table 5).
Sex-specific associations with good outcomes
Discussion
We report that the NAWM K 2 coefficient, as a measure of microvascular integrity, is significantly increased in women compared with men with AIS. In addition, in women we observe sex-specific relationships: NAWM K 2 coefficient is independently associated with NAWM ADC values and a predictor of infarct volume. These findings suggest that increased NAWM K 2 coefficient in women, as a surrogate of BBB dysfunction, is associated with increased infarct size, which predisposes to worse long-term outcomes after stroke.
Our finding of sex-specific differences in NAWM K 2 coefficient, as a putative measure of BBB dysfunction, is of clinical interest. We have previously reported an association between NAWM structural integrity (fractional anisotropy) and sex-specific functional outcomes.11 Together, these observations offer some insight into the potential factors contributing to the disparity in stroke outcomes between sexes as they suggest that sex-specific differences in NAWM microvascular integrity predispose to worse outcomes in women. There are several potential explanations for the observed sex-specific differences in NAWM K 2 coefficient. First, we observed no substantial difference in age, hypertension, diabetes, anticoagulant use, intravenous alteplase treatment, rate of haemorrhagic transformation, WMHv or stroke severity in women. A relationship between NAWM BBB permeability and white matter structural integrity has been reported in individuals with cerebral small-vessel disease.25–27 In our acute cohort, however, we observed no difference in strokes attributed to small-vessel occlusive disease between sexes. We also observed no difference in baseline MMP-2 levels between sexes, a molecule thought to play a role in BBB remodelling.7 Another study showed that diastolic blood pressure and blood glucose were independently associated with BBB permeability abnormalities,28 however, we observed no differences in admission blood pressure or rates of hypertension between sexes. Another hypothesis is the potential hormonal dysregulation of the BBB in women. Different murine models of oestrogen depletion have shown an association with increased BBB permeability.29 30 These observations could suggest that in our female patient population, which is likely predominantly postmenopausal based on age, relative oestrogen deficiency contributes to increased NAWM K 2 coefficient. Future studies investigating the association between menopausal status and BBB permeability could therefore be informative.
We also demonstrate an association between increasing white matter structural injury and alterations in NAWM BBB permeability. In both men and women, increased WMH burden is associated with NAWM K 2 coefficient. These findings support the hypothesis that early microvascular dysfunction in NAWM, causing BBB leakage, precedes white matter damage and WMH development. Corroborating this hypothesis, in patients with the small-vessel disease, increased BBB permeability is associated with WMH burden and hypertension.31 We go on to show in women that NAWM ADC, a marker of altered water mobility, is associated with increased BBB permeability. These findings suggest that there may be sex-specific differences in the early relationship between NAWM BBB permeability and abnormal water mobility or structural integrity, which represents a risk factor for incident stroke and poor outcomes.8 27 32
In women, NAWM K 2 coefficient is associated with larger acute infarct volume. This occurred despite no difference between groups in age, intravenous alteplase administration, small-vessel occlusive stroke subtype, WMH burden and rates of haemorrhagic transformation. One interpretation of these results is that increased NAWM K 2 coefficient predisposes, or is a surrogate, for larger acute infarct volume. In support of this hypothesis, prior work in patients with AIS has shown that the K 2 coefficient of the DWI lesion is inversely associated with rates of reperfusion post alteplase,33 and positively associated with the DWI volume and severity of intracranial haemorrhage postendovascular thrombectomy.34 Based on what has been shown previously on the relationship of increasing BBB permeability and poor functional outcomes after AIS,7 8 35 our findings are promising and hypothesis generating for a role of microvascular integrity in the sex-disparity of stroke outcomes.
There are several limitations of this study that warrant consideration. First, this was a retrospective analysis of a hospital-based biomarker study of AIS subjects who underwent a clinical MRI with PWI within 9 hours from LKW. Non-isotropic voxels were used for analysis of diffusivity anisotropy, which could raise the possibility of partial volume effects as confounders of the MRI measurements.36 This was also an analysis of clinical MRIs performed on patients with acute stroke where differences in patient head orientation, for example, could introduce registration errors of the automated NAWM mask. By automatically applying the same probabilistic white matter mask to each subject, however, this approach reduces human bias from manually placed region-of-interests. An automated approach for selecting NAWM regions-of-interest is therefore a clinically feasible method for measuring global NAWM microstructural and microvascular integrity in patients with AIS.
The interpretation of changes in the K 2 coefficient also warrants discussion as this approach is relatively new for measuring BBB permeability in AIS subjects. At the individual voxel level the K 2 coefficient is a representation of the contribution of the T1 leakage effects due to contrast agent kinetics and the T2* leakage effects due to the tissue microstructure.37 38 For these reasons, the K 2 coefficient may reflect differences in other microvascular and tissue microstructural properties. The measurement of K 2 in the acute setting is also likely a dynamic process with possible global influence from the acute ischaemic event.39 As compared with dynamic contrast-enhanced (DCE) MRI and K trans, the measurement of NAWM K 2 coefficient might have reduced sensitivity in the setting of delayed bolus arrival. However, by restricting our analyses to the hemisphere contralateral to the acute infarct we attempted to account for this limitation. We also cannot exclude the possibility that AIS can influence blood regulation and BBB permeability on remote sites or that differences in contralateral NAWM K 2 reflect differences in reactivity in the acute setting. A DSC-based approach has, however, previously been shown to be feasible for characterising BBB disruption in AIS33 34 and there are distinct advantages of the DSC technique for this population. DCE-MRI has a long acquisition time, which limits its feasibility for studying AIS subjects. In contrast, DSC image acquisition takes 1–2 min. Several prior reports have also demonstrated a strong correlation between K2 and Ktrans.38 40 Lastly, although we show sex-specific differences in NAWM K 2 coefficient and the relationship with infarct volume, the aetiology of this observation is less clear. Future stroke studies applying DSC-MRI to characterise sex-specific differences in BBB permeability, stratified for comorbidities, are therefore necessary.
Conclusions
Despite no differences in age and stroke severity, the NAWM K2 coefficient is increased in women with AIS and associated with infarct volume. These observations suggest that sex-specific differences in microvascular integrity may contribute to the sex disparity in poststroke outcomes.
References
Footnotes
Contributors MRE: designed and conceptualised study; analysed the data; data acquisition; drafted the manuscript for intellectual content. OW: designed and conceptualised study; analysed the data; data acquisition; revised the manuscript for intellectual content. PC, SL, HL, LC, MJRJB, AL, KA and EHL: data acquisition; revised manuscript for intellectual content. SKF and KLF: designed and conceptualised study; revised manuscript for intellectual content. NSR: designed and conceptualised study; analysed data; revised manuscript for intellectual content.
Funding This work was supported by the National Institutes of Health NINDS Specialized Program of Transitional Research in Acute Stroke grant P50-NS051343; R01NS082285; R01NS086905; R01NS059775. Mark Etherton is supported in part by AHA – 17CPOST33680102. Ona Wu is supported in part by NIH-NINDS P50NS051343, R01NS059775, R01NS063925, R01NS082285 and R01NS086905. Pedro Cougo, Svetlana Lorenzano, Hua Li, Steven Feske, and Karen Furie were supported by NIH 5P50NS051343. Natalia S. Rost is supported in part by NIH-NINDS R01NS082285 and R01NS086905.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.