Article Text

Abstract
This editorial discusses the importance of improving awareness of stroke in young individuals. Stoke can occur in any age group and is not restricted to elderly populations. Today, the average age of the first-time stroke patient continues to decrease. However, the incidence of stroke in seemingly healthy, young adults remains neglected, and stroke awareness among young patients remains poor, even in well-developed countries. Education targeting two common barriers to stroke care, identification and rescue, should be implemented for both medical professionals and the public domain. Only through education can we reduce preventable stroke-related death and damage in young patients moving forward.
- stroke
- young
- global health
- awareness
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
In March, Hollywood reeled from the shocking stroke death of 52-year-old Luke Perry.1 The death of a relatively young former actor from ‘stroke’, a frightening brain attack mostly seen in the elderly, was shocking. However, <2 months later, tragedy struck again. After experiencing leg weakness on a long flight from Costa Rica, writer-director John Singleton sought medical treatment. Days later, it was revealed he had suffered a stroke. Falling into a coma soon after, he passed away at only 51 years old.2 These recent tragedies involving Perry and Singleton bring to light the prevalence of stroke in relatively young individuals. While their stroke cases have been highly publicised, Perry and Singleton are far from alone. Patients near their ages and younger have suffered devastating consequences and even death at the hands of society’s lack of stroke awareness.
In February 2018, a 20-year-old student at the University of Lincoln embarked on a school trip.3 Within the next 2 days, she woke up in a stroke ward. In the time that passed, she suffered seven strokes, and a lack of stroke awareness plagued her access to emergency care. A chaperone on her trip disregarded the partial paralysis of her face. A paramedic at her school event simply dismissed her symptoms as an ear infection. A primary care physician she visited never suspected a stroke. She waited for hours in the emergency room to be seen until imaging revealed a stroke, and she finally received proper stroke management. She stated months later that the left side of her body was completely numb. The devastating delay in treatment was due to a failure in timely stroke recognition by both the public and experienced medical professionals.
This college student’s viral news story3 and video4 detailing the incident are tragic. However, just 2 years earlier, a similar incident had occurred when a 33-year-old UK mother collapsed when she suffered a stroke. Three paramedics on the scene failed to recognise the stroke and left her at home to recover. Ten hours later, after another call from the patient’s family, an ambulance finally transported the patient to a hospital, where she fell into coma vigil despite emergent surgery.5 In July 2018, a similar tragedy occurred involving a stroke in a 30-year-old Florida woman and triggered massive news coverage. Paramedics on the scene failed to follow proper protocol required for appropriate prehospital care and subsequent stroke diagnosis. The patient was eventually driven to a nearby hospital by her mother. She passed away 5 days later.6
These cases occurred in well-developed societies with advanced stroke care systems, but they highlight a harsh reality: no society is immune to a lack of stroke awareness and education. Almost half of the global stroke burden now affects young individuals, especially young women, who are at a higher risk.7 Researchers estimate 3.6 million young people are ischaemic stroke victims each year, and rates of ischaemic stroke among the young have continued to increase since the 1980s.7 Stroke death and damage in these cases, which involved both ischaemic and haemorrhagic strokes, is attributable to two primary barriers: failure to identify and failure to rescue. These tragedies, occurring in well-developed societies, have significant implications for other countries and regions, where failure to identify and rescue could be equally or more prevalent. Emergency medical service (EMS) education programmes and public stroke awareness programmes must respond accordingly. Education in both the public and medical domains is vital to preventing similar stroke tragedies in the young.
Identification remains the first barrier to quickly receiving stroke care, and a delay in proper stroke identification by patients, bystanders and medical professionals in the above cases has dire implications for societies all over the world. Since 2007, ‘FAST’ has been the paradigm for educating the general population on stroke recognition and response. It has been widely used in developed, English-speaking regions of the world, especially the USA and the UK. Moreover, programmes similar to it have been used in other nations. To address language and action barriers, we designed two stroke awareness educational programmes: Stroke 120 for China where 120 is used as the emergency medical phone number, and Stroke 112 for countries and regions where 112 is used as the emergency phone number.8 9 Both programmes have stroke and an emergency phone number in their titles, making them easy to remember. While these programmes were designed for developing, non-English speaking countries and regions, similar education programmes are needed for both the general population and emergency medical responders in the developed, English speaking world. Stroke 112 could potentially be used in the USA and the UK; dialling 112 can be redirected to 911 in the USA and 999 in the UK.
Bystanders are crucial to identifying stroke, especially when young stroke victims are disoriented or unresponsive. Children and young adults may often be bystanders to stroke events in young people. Educational programmes for children could therefore improve stroke rapid recognition for young stroke victims and should be integrated in education systems. In the UK student’s case, her young adult classmates were helpful in understanding that something was wrong, but none of them ever explicitly suspected a stroke. In the Florida case, the victim’s daughter alerted her grandmother about her mother’s condition and took the first step in a potentially life-saving effort. In New York City’s Harlem neighbourhood, where many community members are at a high risk of stroke, researchers created an educational programme to teach young children to identify stroke and create a plan of action to seek emergent care. The programme, called ‘Hip-Hop’ stroke, is still used today and uses music and dance to drastically increase students’ knowledge of stroke symptoms and urgency to call 911.10 Educational programmes including information about stroke in younger adults might someday aid in reducing stroke onset-to-door times.
Regardless of public stroke identification, EMS personnel and physicians are needed for formal diagnosis. Emergency medical responders did not properly identify stroke in the three cases. EMS correctly transported the UK student to the hospital, but the patient did not receive immediate stroke care due to late identification. A robust EMS with fast stroke identification capabilities is crucial for timely treatment. A 2007 study on US emergency health line operators revealed that 22% of health line operators confronted with hypothetical stroke symptoms suggested seeing a primary care physician.11 While EMS responders have stroke identification training, they, along with primary care and emergency room physicians, should be reminded of the prevalence of stroke in young adults.
Understanding ‘time is brain’ is equally crucial for prioritising timely brain rescue. Members of the public should understand that calling EMS immediately is critical to minimising delay as demonstrated previously. Only ambulance transportation can potentially alert a stroke centre and bypass the complicated triage and waiting time in emergency rooms.12 This is especially true for young patients, where stroke risk is underestimated and even ignored due to the concept ‘too young to have a stroke’. A recent study indicated a delayed presentation in younger stroke patients.13 Singleton’s case illustrates the sometimes challenging nature of identification. While the time of onset of his stroke is unclear, leg weakness that he experienced is a symptom of stroke and may have been an indicator that he was suffering from one. It is unclear if Singleton knew if his leg weakness might be potentially related to a stroke. While he undoubtedly made the right choice in seeking treatment, making sure patients know stroke symptoms and to call EMS in their presence is vital.
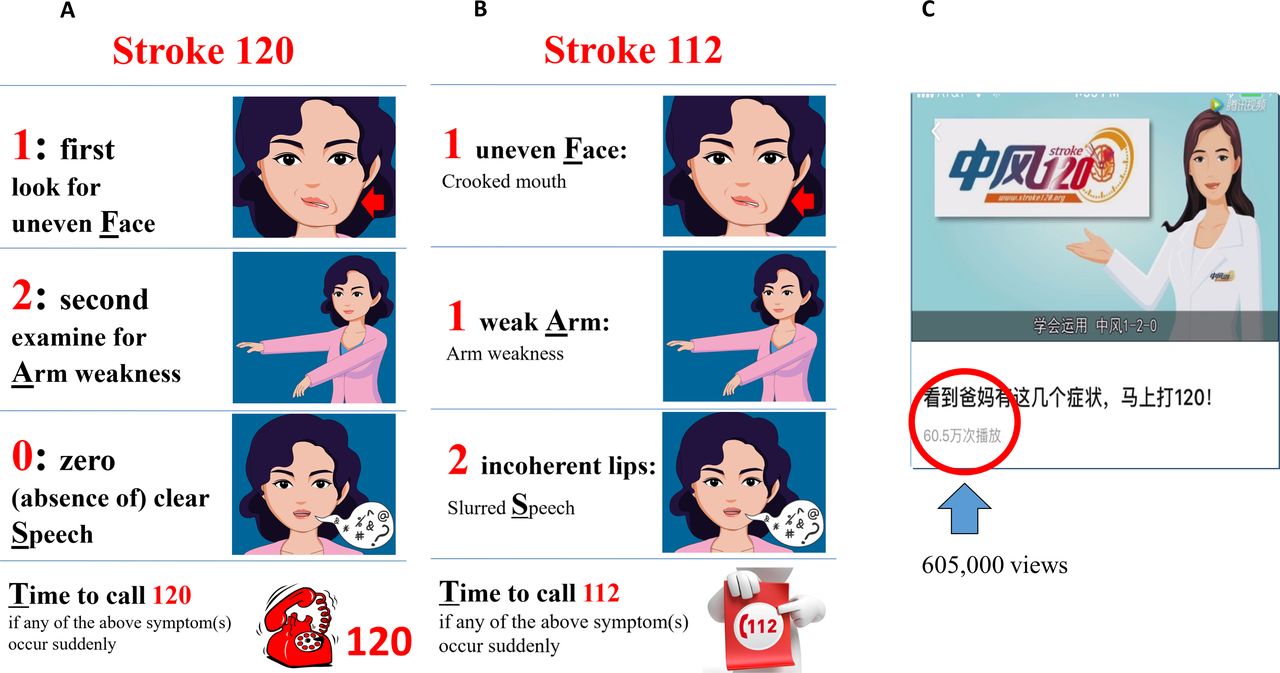
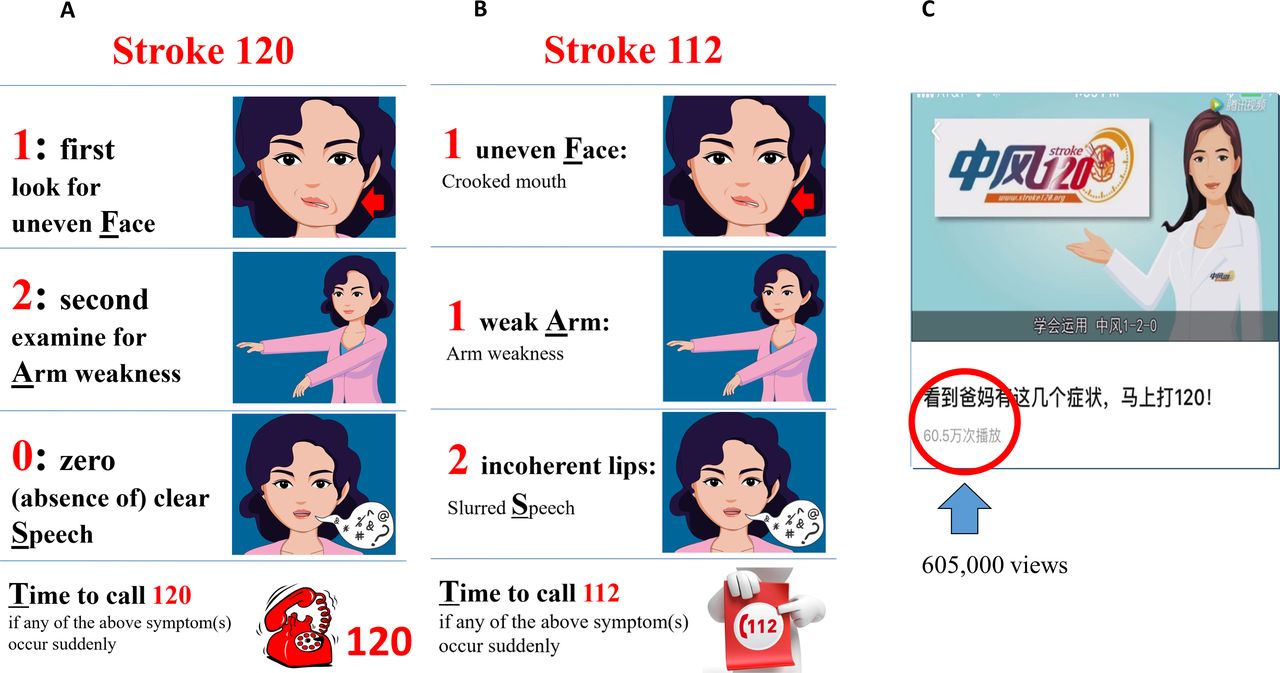
As mentioned previously, identification remains challenging. Therefore, young children and bystanders should also feel comfortable enough to call medical emergency numbers for stroke patients. Our novel educational tools, Stroke 120(figure 1A) and Stroke 112 (figure 1B), could play critical roles in helping the public call EMS quickly.8 9 Figure 1A and B is our newly designed educational material raising awareness about stroke in the young. These educational cartoons remind viewers what stroke symptoms might look like in the otherwise healthy young female. As indicated in figure 1C, videos based on these tools can reach hundreds of thousands of people in a short time span. Stroke 120 programme is written into multiple stroke care guidelines in China.14 15
{kind=link}
Introduction of Stroke 120 and Stroke 112 strategies targeting the young using young adult cartoon. (A) Stroke 120 is a strategy used in China. ‘120’ is the specific medical emergency phone number (EPN) used in the China. (B) Stroke 112 can be used in regions where ‘112’ is the emergency phone number. Please note that Stroke 112 could potentially be used in the USA and the UK; dialling 112 can be redirected to 911 in the USA and 999 in the UK. (C) This demonstrates that one of our stroke educational videos using Stroke 120 strategy went viral immediately after its release. There were 605 000 views of this video within 3 months of its release in a hosting site similar to YouTube, indicating a huge immediate impact.
Stroke is still a leading worldwide cause of death; it can strike patients at any age. More importantly, its ability to strike seemingly healthy, young adults is often overlooked. The stories of Luke Perry, John Singleton, and these three young women remind us how vulnerable younger patients can be as a result of poor stroke awareness, even in the most well-developed countries. To raise stroke awareness in the young, we hosted an international symposium on 30 June 2019 in the Penn Wharton China Center in Beijing, China, with 200 000 active online participants, indicating the public’s great enthusiasm toward’s learning about stroke. We will continue our efforts on a global scale using strategies outlined in a recent summary statement from our group.16 Education targeting two common barriers to stroke care, identification and rescue, should be implemented for both the medical and public domains. Only through education can we prevent similar tragedies moving forward.
Acknowledgments
We appreciate the following funding support from the National Natural Science Foundation of China (81572232, PI: JZ); Shanghai Natural Science Foundation (17dz2308400, PI: JZ); China Research Engagement Funding of the University of Pennsylvania (CREF-030, PI, RL).
Footnotes
Contributors AV drafted the paper. JZ and RL organised the original idea, instructed and revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.