Article Text

Abstract
Background Edaravone Dexborneol is a novel neuroprotective agent that comprised edaravone and (+)-borneol, a food additive with an anti-inflammatory effect in animal ischaemic stroke models. This study aims to assess the safety and efficacy of Edaravone Dexborneol compared with edaravone in treating patients with acute ischaemic stroke (AIS).
Methods In this multicentre, randomised, double-blind, multiple-dose, active-controlled, phase II clinical trial, patients with AIS within 48 hours after stroke onset were randomly assigned (1:1:1:1) to low-dose (12.5 mg), medium-dose (37.5 mg) or high-dose (62.5 mg) Edaravone Dexborneol groups, and an active control group with edaravone (30 mg) by 30 min intravenous infusion every 12 hours, for 14 consecutive days. The primary efficacy outcome was the proportion of modified Rankin Scale (mRS)score ≤1 at 90 days and National Institutes of Health Stroke Scale (NIHSS) score change from baseline to 14 days after randomisation. The safety outcome included any adverse event during 90 days after treatment.
Results Of 385 patients included in the efficacy analysis, 94 were randomised to low-dose group, 97 to medium-dose group, 98 to high-dose group and 96 to the control group. No significant difference was observed among the four groups on mRS score (mRS ≤1, p=0.4054) at 90 days or NIHSS score change at 14 days (p=0.6799). However, a numerically higher percentage of patients with mRSscore ≤1 at 90 days in the medium-dose (69.39%) and high-dose (65.63%) groups was observed than in the control group (60.64%). No significant difference in severe adverse events was found among the four groups (p=0.3815).
Conclusions Compared with edaravone alone, Edaravone Dexborneol was safe and well tolerated at all doses, although no significant improvement in functional outcomes was observed at 90days.
Trial registration number NCT01929096.
- compound edaravone
- ischemic stroke
- neuroprotection
- edaravone
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Stroke is the leading cause of death and acquired adult disability in China and has significant economic burden.1 2 However, numerous neuroprotective agents have failed to show any benefit in the treatment of patients with acute ischaemic stroke (AIS), making the search for new treatments imperative.3 Edaravone is an effective free radical scavenger4 5 recommended for AIS treatment by Chinese and Japanese stroke care guidelines.6 7 Edaravone scavenges free radicals, such as hydroxyl free radical (·OH), nitric oxide free radicals (NO·) and peroxynitrite anion (ONOO−), sequentially relieves cerebral oedema, and inhibits delayed neuronal death.4 8 9 However, cerebral ischaemic injury is extremely complex and involves free radicals and inflammatory response. (+)-Borneol inhibits the production or expression of inflammation-related proteins and prevents brain injury or impairment. Edaravone Dexborneol is a novel neuroprotective agent that comprised edaravone and (+)-borneol in a 4:1 ratio10 that may have a better therapeutic effect.11 12 Complementarity exists between edaravone and (+)-2-campheol. Pharmacological research on the efficacy of edaravone combined with (+)-borneol showed that, compared with edaravone alone, Edaravone Dexborneol showed synergistic effect and longer treatment time, which indicated that the protective effect of Edaravone Dexborneol on cerebral ischaemic injury was better than that of the marketed edaravone. The present multicentre, randomised, active-controlled, double-blind study aims to verify the safety and efficacy of Edaravone Dexborneol in patients with AIS.
Methods
Study design
This was designed as a phase II, multicentre, randomised, double-blind, multiple-dose, active-controlled clinical trial conducted at 28 centres in China between May 2013 and February 2015. Patients were assigned to treatment after they had given informed consent.
Patient selection
Patients who met the following inclusion criteria were eligible for enrolment: age 35–75 years, diagnosis of AIS, ability to start the study drug within 48 hours after stroke onset, a National Institutes of Health Stroke Scale (NIHSS) score between 4 and 24, and a total score of upper and lower limbs ≥2 on motor deficits.
Study intervention
For this trial, 400 cases were planned to be randomised into four groups: control group (edaravone injection, 30 mg/dose, once every 12 hours, continued for 14 days), low-dose group (Edaravone Dexborneol injection, 12.5 mg/dose [edaravone 10 mg, (+)-borneol 2.5 mg], one dose every 12 hours, continued for 14 days), medium-dose group (Edaravone Dexborneol injection, 37.5 mg/dose [edaravone 30 mg, (+)-borneol 7.5 mg], one dose every 12 hours, continued for 14 days) and high-dose group (Edaravone Dexborneol injection, 62.5 mg/dose [edaravone 50 mg, (+)-borneol 12.5 mg], one dose every 12 hours, continued for 14 days). Randomisation was stratified according to the interval between the stroke onset and enrolment (≤24 hours vs between 24 hours and 48 hours). The randomisation number was assigned by an automated randomisation system.
Efficacy outcome assessment
The primary efficacy outcome was defined as the proportion of modified Rankin Scale (mRS) score ≤1 at 90 days and NIHSS score change from baseline to 14 days after randomisation; the secondary efficacy outcomes included (1) NIHSS score ≤1 at 14, 30 and 90 days after randomisation; (2) Barthel Index ≥95 at 14, 30 and 90 days after randomisation; (3) Montreal Cognitive Assessment score at 14, 30 and 90 days after randomisation; and (4) Stroke Impact Scale score at 90 days.
Safety outcome assessment
Data for safety assessment included adverse reactions observed during the trial and changes in laboratory data before and after treatment. Severe adverse events (SAEs) included disability, prolonged hospitalisation and death.
Statistical analysis
Based on the principle of intention-to-treat analysis, all randomised patients were included in the safety analysis, and patients who had at least one valid assessment were included in the efficacy analysis. The last observation was used for patients who withdrew from the study and counted as lack of efficacy. Data for patients who withdrew because of safety or other reasons were included throughout the last visit and before the termination of the study. The baseline characteristics in four groups were compared. Proportions were used for categorical variables, and means with SD were used for continuous variables. Differences in efficacy and safety outcomes among four groups were analysed. Continuous data were analysed by analysis of variance or Kruskal-Wallis test, and categorical data examined by χ2 test or Fisher’s exact test. All tests were two-sided, and a p value of 0.05 was considered statistically significant. All statistical analyses were performed using SAS V.9.2 software.
Results
Baseline characteristics
The trial enrolled 400 patients: 98 in the control group, 102 in the low-dose group, 101 in the medium-dose group and 99 in the high-dose group. All received the treatment for the first time and included in the safety analysis. Fifteen patients lost to follow-up before the first assessment were excluded in the efficacy analysis. Of the remaining 385 patients, 303 completed the study according to the protocol (figure 1). Baseline demographic and clinical characteristics were well matched among the four groups analysed based on the efficacy data (table 1).
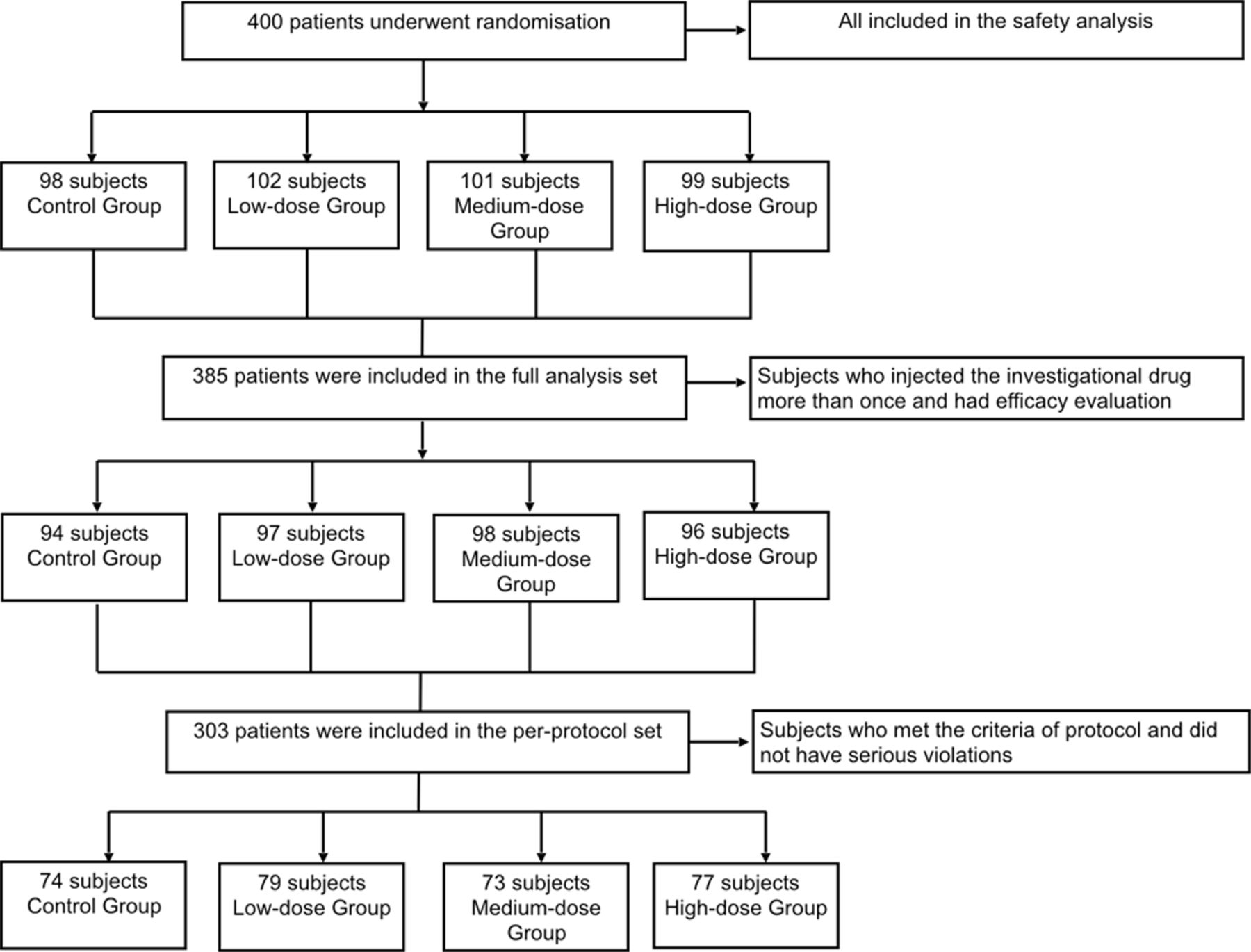
Flow chart of the clinical trial.
Baseline characteristics (FAS)
Safety analysis
The incidence of adverse reactions was 6.12%, 8.82%, 10.89% and 14.14% in the control, low-dose, medium-dose and high-dose groups, respectively. The details of adverse reactions are listed in online supplementary table 1. The severe adverse reactions leading to withdrawal were observed in 3 (3.06%), 2 (1.96%), 3 (2.97%) and 4 (4.04%) patients in the control, low-dose, medium-dose and high-dose groups, respectively. The major adverse reactions included pruritus, skin rash, acute liver injury and kidney injury. SAEs were observed in 10 (10.20%), 4 (3.92%), 6 (5.94%) and 7 (7.07%) patients in the control, low-dose, medium-dose and high-dose groups, respectively, and no significant difference was found (p=0.3815). Among a total of 29 SAEs, 2 events (severe liver and kidney damage) were related to Edaravone Dexborneol, both of which happened in one patient in the high-dose group. However, recovery was achieved after the treatment. Two patients in the edaravone control group and 0 patient in the Edaravone Dexborneol group died. These two deaths in the edaravone control group were considered as unrelated to the treatment, and the causes of death were worsening of stroke and septicaemia.
Supplementary file 1
Efficacy outcomes
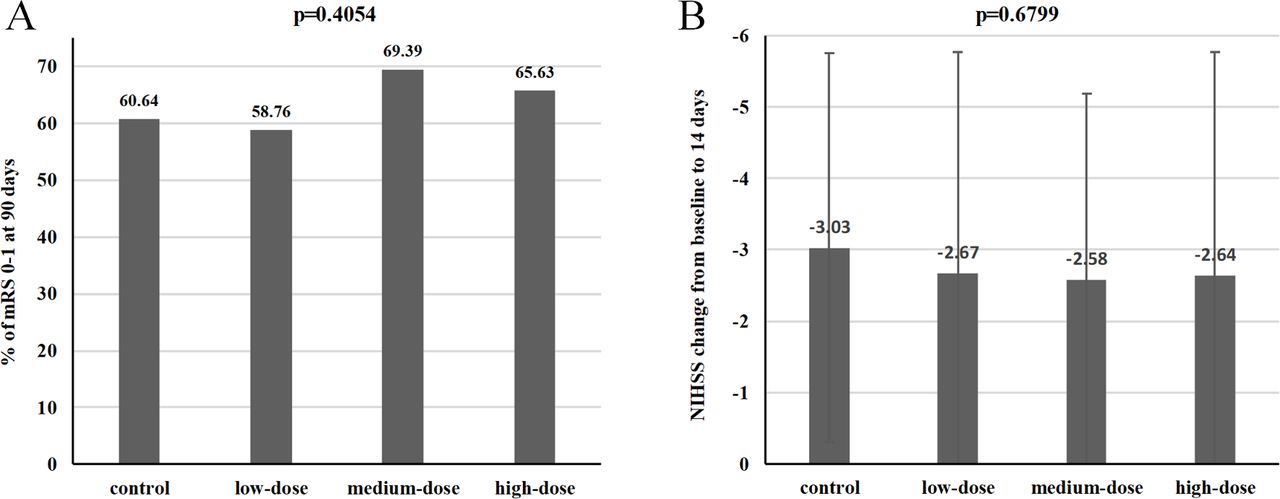
The incidence of primary efficacy outcome (mRS scores of ≤1 after treatment at 90 days) in the control, low-dose, medium-dose and high-dose groups was 60.64%, 58.76%, 69.39% and 65.63%, respectively. No significant difference was observed (p=0.4054). However, the proportion of mRS score of ≤1 in medium-dose and high-dose groups had possible higher trend than in the control group (69.39% and 65.63% vs 60.64%; figure 2A). Moreover, no significant difference was seen among the four groups in terms of NIHSS score changes from baseline to 14 days after treatment (p=0.6799; figure 2B). The secondary efficacy outcomes in this trial are summarised in table 2. There were no significant differences among the four groups in terms of these secondary efficacy outcomes.

{kind=link}
{kind=link}
Primary efficacy outcomes. (A) % of mRS score 0–1 at 90 days. (B) NIHSS score change from baseline to 14 days. mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale.
Secondary efficacy outcomes among the four groups
Discussion
In this phase II, multicentre, randomised, double-blind, multiple-dose, active-controlled clinical trial, Edaravone Dexborneol at different doses was compared with edaravone alone for efficacy and safety. Our result showed that, compared with edaravone alone, Edaravone Dexborneol was safe and well tolerated at all doses, although no significant improvement in functional outcomes was observed.
Neuroprotective drugs might extend the therapeutic time window after stroke for thrombolysis or thrombectomy therapy by delaying cell death and blocking reperfusion injury. Edaravone Dexborneol could provide as a new and effective treatment of stroke in the future.13 After onset of ischaemic stroke, several risk factors were associated with the damage process of neurons under ischaemia: energy failure, free radicals production, formation of neurotoxin, inflammatory responses and apoptosis.14 Although vascular recanalisation could effectively salvage reversible ischaemic tissue,15 the risk of reperfusion injury was high. Edaravone could limit vascular endothelial cell injury, brain oedema,16 17 tissue injury18 and delayed neuronal death, and consequently reduced neurological deficits.19 Additionally, as seen on sequential magnetic resonance spectroscopy, preservation of N-acetyl-aspartate, a neuron-specific amino acid, in the ischaemic brain of edaravone-treated patients has been reported.20 Edaravone Dexborneol is a novel neuroprotective agent indicated for AIS.10 It is a compound preparation comprising edaravone and (+)-borneol in a 4:1 ratio. The natural borneol consists of over 96% borneol that could inhibit the production or expression of inflammation-related proteins such as tumour necrosis factor-α (TNF-α), interleukin-1β, cyclo-oxygenase-2 and induced nitric oxide synthase (iNOS), and prevent brain injury or impairment.11 Borneol has been widely used to treat cerebrovascular disease, but is rarely used alone.21
In this trial, the major adverse reactions included pruritus, skin rash, acute liver injury and kidney injury. The adverse reactions of Edaravone Dexborneol seemed to show a dose-dependent relationship. It is worth noting that, among a total of 29 SAEs, 2 events (severe liver and kidney damage) were related to Edaravone Dexborneol, both of which happened in one patient in the high-dose group. The underlying pharmacological mechanisms remained unclear. In consideration of safety, high-dose Edaravone Dexborneol should not be recommended for further clinical investigation.
Although no significant difference was found among the four groups in the primary efficacy outcome, proportions of the patients with mRS score of ≤1 at 90 days in the group treated with medium-dose (69.39%) or high-dose (65.63%) Edaravone Dexborneol were higher than in the group treated with edaravone (60.64%), and we found the efficacy of the medium-dose Edaravone Dexborneol was likely to be even better than the high-dose one. In combination with efficacy and safety data, a phase III clinical trial with the medium-dose edaravone group, with a dose of 37.5 mg/time (edaravone 30 mg, (+)-borneol 7.5 mg) is suggested.
Edaravone Dexborneol can improve acute brain injury considerably in animal models of focal cerebral ischaemia (reperfused or permanent) and whole cerebral ischaemia reperfusion.22 No drug interaction in vivo between edaravone and (+)-borneol was observed from the preclinical pharmacokinetic study, including absorption, distribution, metabolism and excretion. Edaravone and (+)-borneol rapidly distributed in most tissues and excreted mainly from urine and bile in a conjunction form. Edaravone, (+)-borneol and Edaravone Dexborneol were not inhibitors or inducers of major CYP (Cytochrome P450 proteins) enzymes (online supplementary table 2). The risk of genetic and reproductive toxicity was not observed in the preclinical studies (online supplementary tables 3 and 4). The pathophysiological mechanism of cerebral ischaemic injury is complex, involving factors such as excitatory amino acids, calcium overload, free radicals, inflammatory response and apoptosis.18 Pharmacological intervention alone cannot affect this complex process effectively.9 Studies that engage multiple targets to improve ischaemic injury are ongoing.23–25 In theory, using two different agents to target different steps of ischaemic injury is likely superior to a single agent in preventing ischaemia.26
Edaravone Dexborneol enhanced inhibition of iNOS and TNF-α expression and lower level of ONOO− in the ischaemic brain. It could contribute to the synergetic effect of edaravone and borneol in combination. However, this study has several limitations. First, since the study is a phase II study and the sample is small, we cannot make further explorations on the effect of Edaravone Dexborneol on each TOAST (Trial of Org 10 172 in Acute Stroke Treatment) type with stratification analysis, which will be done in the phase III study. Second, for ethical reasons, only a positive control group (edaravone group) was set up in the study and there was no placebo control group. Third, since no blood samples were collected from the patients in the study, we cannot measure the changes in inflammatory factors before and after medication, and inflammatory factors will be used as secondary indicators to analyse the anti-inflammatory effect of Edaravone Dexborneol.
Conclusion
Medium-dose Edaravone Dexborneol was safe in this phase II, multicentre, randomised, double-blind, multiple-dose, active-controlled clinical trial. However, the efficacy still needs to be explored in a large trial. The medium-dose edaravone group (37.5 mg/time) (edaravone 30 mg, (+)-borneol 7.5 mg) will be the optimal dose for a phase III clinical trial.
References
Footnotes
JX and YW contributed equally.
Contributors YoW had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. JX and YiW contributed equally to this work. Study concept and design: YoW. Supplying patients: XZ, YiW, ZG, XG, HC and JZ. Drafting of the manuscript: JX and YiW. Critical revision of the manuscript for important intellectual content: XZ and YiW. Statistical analysis: AW. Study supervision: YoW.
Funding Simcere Pharmaceutical Group supported the present study.
Competing interests None declared.
Ethics approval The study was approved by the institutional review board of each study centre and was conducted in accordance with the principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it first published. The chemical name of the medicine ’compound edaravone‘ has been changed to ’edaravone dexborneol' throughout the article.
Patient consent for publication Parental/guardian consent obtained.