Article Text

Abstract
Objective Intravenous tissue plasminogen activator (tPA) is the standard therapy for patients with acute ischaemic stroke (AIS) within 4.5 hours of onset. Recent trials have expanded the endovascular treatment window to 24 hours. We investigated the efficacy and safety of using multimodal MRI to guide intravenous tPA treatment for patients with AIS of unknown time of onset (UTO).
Methods Data on patients with AIS with UTO and within 4.5 hours of onset were reviewed. Data elements collected and analysed included: demographics, National Institutes of Health Stroke Scale (NIHSS) score at baseline and 2 hours, 24 hours, 7 days after thrombolysis and before discharge, the modified Rankin Scale (mRS) score at 3 months after discharge, imaging findings and any adverse event.
Results Forty-two patients with UTO and 62 in control group treated within 4.5 hours of onset were treated with intravenous tPA. The NIHSS scores after thrombolysis and/or before discharge in UTO group were significantly improved compared with the baseline (p<0.05). Between the two groups, no significant differences in NIHSS score were observed (p>0.05). Utilising the non-inferiority test, to compare mRS scores (0–2) at 3 months between the two groups, the difference was 5.2% (92% CI, OR 0.196). Patients in the UTO group had mRS scores of 0-2, which were non-inferior to the control group. Their incidence of adverse events was similar.
Conclusions Utilising multimodal MRI to guide intravenous only thrombolysis for patients with AIS with UTO was safe and effective. In those patients with AIS between 6 and 24 hours of time of onset but without large arterial occlusion, intravenous thrombolysis could be considered an option.
- stroke with unknown time of onset
- late reperfusion
- IV thrombolysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Acute ischaemic stroke (AIS) is one of the leading causes of disability and mortality in the world. Ultra-early intravenous alteplase (tissue plasminogen activator, tPA) has been proven effective when given within 4.5 hours of onset. However, many patients with AIS present late to the emergency room and miss the treatment time window. They have an unknown time of onset (UTO) and often have a stroke on waking up. In 2017, two trials have reported that intra-arterial (IA) thrombectomy was effective and safe to treat patients with AIS with an onset of up to 24 hours if multimodal imaging studies identified a diffuse perfusion mismatch. There are very few reports on giving intravenous tPA beyond 4.5 hours under the guidance of multimodal imaging studies at present. The recently published WAKE-UP (Efficacy and Safety of MRI-based Thrombolysis in Wake-Up Stroke) and MR WITNESS (Study of Intravenous Thrombolysis With Alteplase In MRI-Selected Patients) trials used MRI diffusion-weighted images (DWI)/fluid-attenuated inversion recovery (FLAIR) mismatch to select the patients for thrombolysis beyond 4.5 hours.1 In this study, we evaluated the efficacy and safety of using multimodal MRI DWI/perfusion-weighted images (PWI) mismatch to guide intravenous tPA in patients with AIS with UTO.
Methods
Eligibility criteria
Data of all patients who had intravenous tPA at Zhengzhou Central Hospital from August 2015 to July 2017 were reviewed. Patients were eligible for multimodal MRI-guided intravenous tPA if they met the following criteria: (1) >18 years old; (2) AIS with UTO; (3) no impairment of consciousness; (4) no intracranial haemorrhage (ICH) on CT; (5) no obvious hypodensity or early changes of cerebral infarction; (6) presence of PWI/DWI mismatch or DWI/FLAIR mismatch; (7) no large vessel occlusion; (8) no clinical contraindications; and (9) consent signed by the patient or legal representative.
Patients in the control group were treated with intravenous tPA if they met the following criteria: (1) >18 years old; (2) AIS within 4.5 hours; (3) no impairment of consciousness; (4) no ICH on CT; (5) no obvious hypodensity or early changes of cerebral infarction; (6) no clinical contraindications; and (7) consent signed by the patient or legal representative.
Stroke classification, risk factors and imaging examination: CT, MRI, MR angiography, DWI and PWI
The Trial of Org 10172 in Acute Stroke Treatment (TOAST) Classification2 3 was used to classify the subtypes of AIS: large-artery atherosclerosis (LAA), cardioembolism (CE), small-vessel occlusion (SVO) and stroke of undetermined aetiology. The correlation of anatomical area of stroke was divided into: anterior cerebral circulation and posterior cerebral circulation. Risk factors recorded included: hypertension, coronary heart disease, diabetes, hyperlipoidaemia, hyperhomocysteinaemia and atrial fibrillation.
CT scan: All patients had a baseline non-contrast CT of brain to exclude any intracerebral haemorrhage.
MRI, MR angiography (MRA), DWI, PWI: Each patient underwent three-dimensional time-of-flight MRA, DWI and dynamic contrast-enhanced PWI with gadolinium diethylenetriamine pentaacetic acid MRI (Siemens, Germany). PWI processing software was used. Cerebral blood volume, mean transit time, time to peak and cerebral blood flow in bilateral cerebral hemispheres were evaluated by two experienced radiologists who determined whether the perfusion study was abnormal. The DWI/PWI mismatch was defined as a PWI lesion >20% of the DWI lesion in size. The DWI-FLAIR mismatch was defined by the presence of a diffusion restricting infarct core and the complete absence of FLAIR hyperintensity.
Treatment and outcome evaluation
Patients were given intravenous tPA (0.9 mg/kg, 10% intravenous bolus and rest intravenous over 60 min). Vital signs were assessed according to the protocol within 24 hours after intravenous tPA. A follow-up Computer Tomography of Head (CTH) was done at 24 hours after intravenous tPA. Aspirin (oral 100 mg daily) was administered 24 hours after intravenous tPA. Patients were also given standard risk factor modification therapies. The National Institutes of Health Stroke Scale (NIHSS) score was collected before and at 2 hours, 24 hours, 7 days after tPA and before discharge. Modified Rankin Scale (mRS) score was evaluated at 90 days. Outcome measures included any intracranial or systemic haemorrhage and recurrent strokes.
Statistical method
The baseline and clinical characteristics were compared between the two groups by using the χ2 test or Fisher’s exact test for categorical variables and Student’s t-test for continuous variables with normal or skewed distribution, respectively. Continuous variables were expressed as means with SD. Categorical data were presented as proportions. NIHSS scores in both UTO and control groups were analysed by repeated measures analysis of variance and the p value was corrected via Greenhouse-Geisser method. Post-tPA NIHSS scores at different time points were compared with NIHSS scores before thrombolysis. mRS scores of 0–2 in both groups were compared for non-inferiority with a 90% CI. Statistical analysis of the data was performed by using the Statistical Package for the Social Sciences (SPSS) V.19.0.
Results
From August 2015 to July 2017, sixty-two patients who received intravenous tPA had multimodal MRI. Among them, 42 (22 male and 20 female) had UTO. Their average age was 63.93. Thirty-eight (90.5%) had stroke on awakening. Other four had UTO during the day. The average time of last seen normal (LSN) to intravenous tPA was 538.05±167.71 min. According to the TOAST classification, 22 (52.4%) had LAA; 4 (9.5%) had CE; 15 (35.7%) had SVO; 1 had stroke of undetermined aetiology. For the vascular distribution, 23 (54.8%) were in the anterior cerebral circulation and 19 (45.2%) were in the posterior cerebral circulation. Their average NIHSS score on admission was 7.31±5.16. The common risk factors include: hypertension in 28 (66.7%) patients, coronary heart disease in 23 (54.8%), diabetes in 16 (38.1%), hyperlipoidaemia in 29 (69.0%), hyperhomocysteinaemia in 16 (38.1%) and atrial fibrillation in 7 (16.7%).
In the control group, 62 patients (36 male and 26 female, average age 70.39±13.42) had onset within 4.5 hours and received intravenous tPA. Among them, 27 (43.5%) had LAA; 12 (19.4%) had CE; 18 (29.0%) had SVO; 1 (1.6%) had undetermined aetiology; and 4 (6.5%) had undetermined aetiology. Forty-eight (77.4%) had anterior cerebral circulation and 14 (22.6%) had posterior cerebral circulation. For the risk factors, 45 (72.6%) had hypertension, 26 (41.9%) had coronary heart disease, 18 (29.0%) had diabetes, 34 (54.8%) had hyperlipidaemia, 17 (27.4%) had hyperhomocysteinaemia and 12 (19.4%) had atrial fibrillation. Their average NIHSS score on admission was 7.53±6.75. The average LSN to intravenous tPA time was 155.76±55.98 min.
There was no significant statistical difference between the two groups in sex, stroke subtypes and risk factors. However, there were significant differences between the two groups in age, infarct locations and the time from LSN to thrombolysis (table 1).
Demographic and baseline characteristics of patients in the UTO group and the control group
All 42 patients were found to have DWI/FLAIR mismatch. Among them, 32/33 showed PWI/DWI mismatch. The average volume of mismatch was 2.5 mL (0.1–11.2).
The improvement of the NIHSS score at each time period after thrombolysis was observed in both groups but showed no statistical difference (table 2). The overall NIHSS score between the two groups showed no statistical significance (p=0.810). The NIHSS scores at 2 hours, 24 hours, 7 days after thrombolysis and before discharge in UTO group were significantly improved compared with before thrombolysis (p<0.05, table 3). No significant differences were seen for the mRS score (0–2) at 3 months after thrombolysis in both groups (p=0.556, table 2). Utilising the non-inferiority test to compare mRS scores of 0–2 between the UTO group (n=32, 76.2%) and the control group (n=44, 71.0%), the difference was 5.2% (92% CI, OR 0.196). Hence, mRS scores achieved 0–2 in the UTO group were non-inferior to the control group (table 2).
Comparison of the NIHSS scores before and after thrombolysis and the mRS score at 3 months after thrombolysis between the two groups
Comparison of NIHSS scores at the different time points after thrombolysis with before thrombolysis in the UTO and control groups (one-tailed t-test results, p values)
In the UTO group, gingival haemorrhage occurred in five cases (11.9%). No one had ICH or died. In the control group, gingival haemorrhage occurred in three cases (4.8%): two cases (3.2%) had ICH and one (1.6%) died (table 4).
Comparison of adverse events between the two groups
Discussion
In this series, up to 36% of cases of AIS had UTO. Some had stroke on awakening (wake-up stroke, WUS) and others had daytime-unwitnessed stroke.4–6 For the patients with UTO, the time of onset exceeded the therapeutic time window for intravenous tPA since the time of onset was calculated as the patient was LSN.7 8
Intravenous tPA or urokinase is the most effective therapy for AIS if given early but with a tight therapeutic time window. Currently, the internationally recognised therapeutic time window for intravenous recombinant tPA is within 3–4.5 hours and for intravenous urokinase, within 6 hours of onset (only used in China). Unfortunately, the time of onset for a large number of patients with AIS is unclear. They often passed the treatment window when they arrived at the hospital. The rate of thrombolysis in China was around 2%. In recent years, the concept of tissue window offered new hope for patients with AIS presented beyond 6 hours, a time window that was not to be surpassed before.9 10 Multimodal imaging-guided treatment has shown that the benefit in three IA thrombectomy trials could be expanded to 6–24 hours of onset.11–13 If only using intravenous tPA beyond 4.5 hours of onset, multimodal imaging might work.14 The sensitivity and specificity of DWI/FLAIR mismatch detecting a stroke within 3 hours of symptom onset were 94% and 97%, and 62% and 68% within 4.5 hours of symptom onset.15 16 In Desmoteplase in Acute Ischemic Stroke trial, intravenous thrombolysis was used within 9 hours of onset when MRI PWI/DWI showed a mismatch.17 Fink’s study showed that PWI/DWI mismatch was seen in patients in WUS about 73% of time compared with 82% (p=0.4) for those presented within 3 hours of symptom onset, which suggested that the patients with WUS might have a window to get the benefit from thrombolysis.18 There was also an assumption that patients with WUS had their stroke within a short period of time before awakening.19
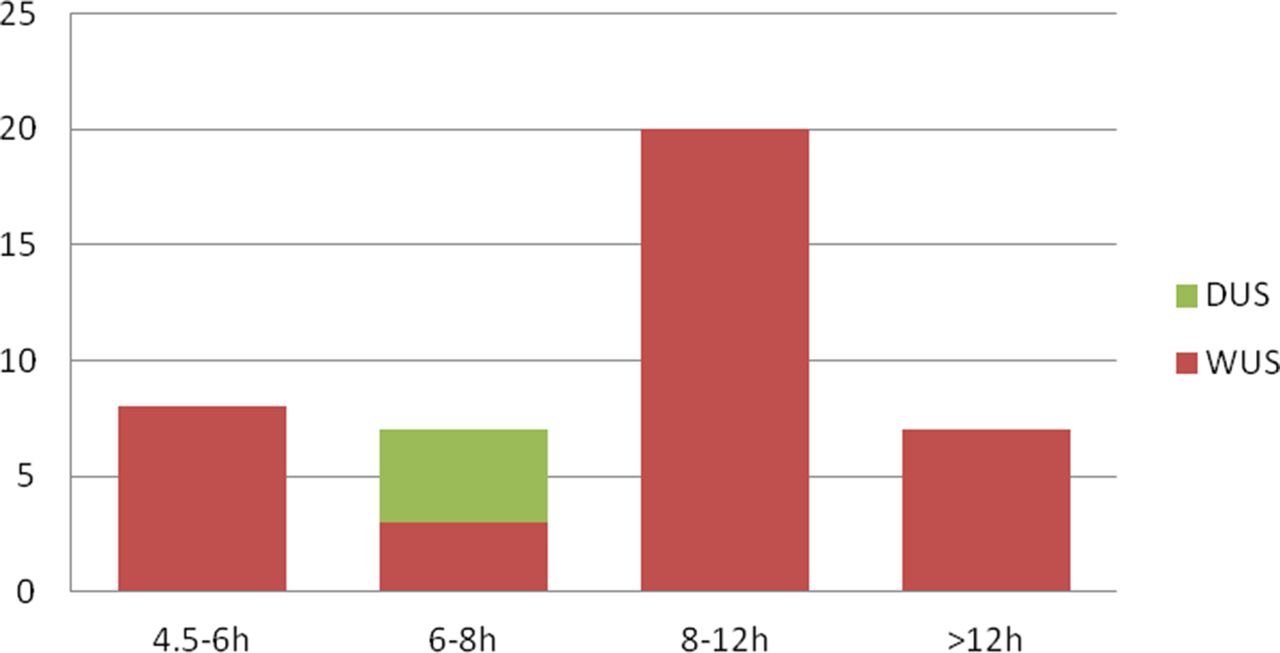
In our study, all 42 patients in the UTO group had DWI/FLAIR mismatch and among them, 32/33 also had DWI/PWI mismatch. They included 7 patients in the group treated >12 hours; 20 treated within 8–12 hours; 7 treated within 6–8 hours; and 8 treated within 4.5–6 hours (figure 1). The favourable outcome after such intervention indicated the likelihood of the presence of penumbra in patients with AIS presented beyond 4.5 hours, and multimodal imaging could guide the treatment better than using the witnessed time window in late presenters. Recently published three IA thrombectomy trials treating patients with AIS with large arterial occlusions presented between 6 and 24 hours certainly illustrated this issue of tissue time window of opportunities determined by DWI/PWI mismatch.11–13 While these three trials used IA thrombectomy, in our series, intravenous tPA was also effective beyond 6 hours of onset in those without large arterial occlusion but with a mismatch on MRI. The WAKE-UP trial was a randomised trial that successfully treated patients with AIS between 8 and 12 hours if there was a DWI/FLAIR mismatch. The average NIHSS score of patients enrolled was 6 and the average lesion volume on DWI was 2 mL. The 90-day outcome showed an mRS score of 1 in the treatment group and 2 in the placebo group. However, tPA group had 10 deaths (4.1%) while placebo group had three (1.2%). Treatment group also had more symptomatic ICH (sICH) (2.0%) than the placebo group (0.4%). In the single-arm MR WITNESS trial, 80 patients received 0.9 mg/kg intravenous tPA at a median of 11.2 hours after onset if a DWI/FLAIR mismatch was present. One had sICH (1.3%). However, 39% achieved mRS scores of 0–1.20

{kind=link}
Time distribution of last seen normal (LSN) to thrombolysis in patients with unknown time of onset (UTO). DUS, daytime-unwitnessed stroke; WUS, wake-up stroke.
Although our series was small in numbers of patients treated and not randomised, patients treated under MRI DWI/PWI guidance were within 538.05±167.71 min, longer than those treated in WAKE-UP trial. Our study showed no statistical difference in outcome when measured by NIHSS scores, mRS score (0–2) at 3 months and complications between the UTO and the control groups. Our series had no ICH.
Our study has several limitations. First, the number of patients in this study was relatively small. Second, this was a retrospective study, which could bring bias in patient selection.
Conclusion
Our study confirmed the findings in the WAKE-UP and MR WITNESS trials and provided some evidence that in real clinical practice, a positive outcome might still be present, with no ICH, extending the time window for treatment with intravenous tPA to even beyond 12 hours of onset if a mismatch was present on MRI DWI/PWI. A large prospective trial treating patients with AIS beyond 12 hours of onset under MRI guidance is needed to confirm our findings.
References
Footnotes
JZ and HZ contributed equally.
Contributors JZ, HZ and RW had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: RW, JZ and HZ. Acquisition of clinical data: JLi, CL, JLv, YL, WL, DM, JLiu, YY, RL, QY, YW, PL and YW. Analysis and interpretation of data: JZ and HZ. Imaging diagnostic data analysis and interpretation: RL, XX and HH. Drafting of the manuscript: JZ and HZ. Critical revision of the manuscript for important intellectual content: JZ and RW. Statistical analysis: JZ and HZ.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This is a retrospect review approved by the Zhengzhou Central Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.