Article Text

Statistics from Altmetric.com
Background
In this study, we performed emergency stent angioplasty in a patient with basilar artery occlusion (BAO) at 21 hours after onset. Serial diffusion tensor tract imaging revealed that the ischaemic corticospinal tracts (CSTs), which passed through pontine infarct, rapidly recovered to normal level even after delayed reperfusion. This case provided in vivo evidences that ischaemic white matter was still salvageable even after prolonged ischaemia. It also provided a new method (diffusion tensor tract imaging) and a novel therapeutic target (white matter) in the evaluation and treatment of acute BAO.
Case presentation
A 35-year-old man suffered acute onset of dizziness, generalised weakness and mental dullness for 21 hours. Neurological examination revealed consciousness disturbance, drooping eyelids, horizontal gaze-evoked nystagmus, facial weakness, dysarthria, dysphagia, bilateral limb weakness (Medical Research Council grade III) and a NIHSS score of 19.
Investigations
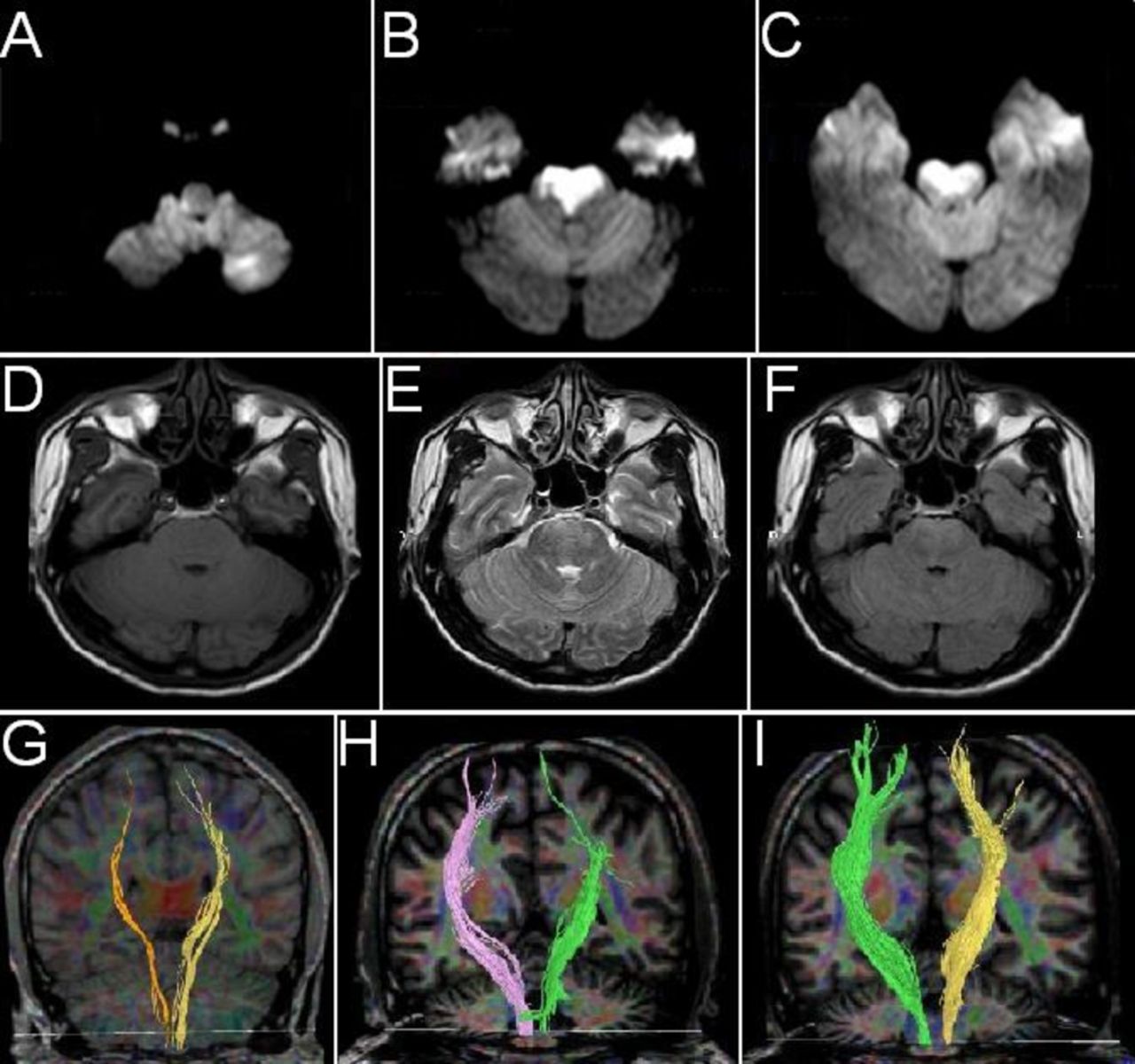
Diffusion weighted imaging after admission revealed acute ischaemic lesions in right dorsolateral medulla, left cerebellum and bilateral pontine base (figure 1A–C). No intracranial haemorrhage was detected (figure 1D–F). On MR angiography, left vertebral artery (VA) and basilar artery (BA) were not patent while right VA was faintly visible (data not shown). Diagnostic cerebral angiography was performed after obtaining informed consent from the next of kin. After intravenous sedation and general anaesthesia, a sheath passage of size 6 Fr was applied by Seldinger technique. Angiography of the aortic arch was performed by a 5F pigtail catheter (Cordis, Miami, Florida, USA). Angiography of left internal carotid artery (ICA) and left VA were performed by a 5F VER catheter (Cordis, Miami, Florida, USA). Complete occlusion of BA beyond the anterior inferior cerebellar artery branch was demonstrated (figure 2A). Posterior cerebral artery (PCA) and superior cerebellar artery were supplied by collateral circulation from left ICA (figure 2B).

MRI revealed acute ischaemic lesions in the right dorsolateral medulla, the left cerebellum and the pontine base (A–C). No intracranial haemorrhage was detected (D–F). Injured corticospinal tracts at admission (G) recovered to normal level at 1-month (H) and 3-month (I) follow-up. FA values of bilateral pontine also increased during the follow-up (FA at admission, 1 month and 3 months: Left side: 0.421, 0.578, 0.525; Right side: 0.396, 0.550, 0.583). FA, fractional anisotrophy.

{kind=link}
{kind=link}
(A) Angiogram demonstrated complete occlusion of BA beyond the AICA branch. (B) Filling of PCA and SCA was achieved on left ICA angiogram as a result of collateral circulation. (C) Stenting deployment. (D) The antegrade flow partially reversed after the therapy (Upper row coronal view, lower row sagittal view). At 1-year follow-up, repeated cerebral angiography revealed that (E) BA was supplied by the dominant left VA. (F) The right VA was hypoplastic. (G) PCA and SCA was not opacified on left ICA angiogram, indicating that the opening of the left postcommunicating artery (B) was temporary at the disease onset. (H). Filling of PCA and SCA by right ICA. AICA, anterior inferior cerebellar artery; BA, basilar artery; ICA, internal carotid artery; LICA, left internal carotid artery; LV, left vertebral artery; PCA, posterior cerebral artery; RICA, right internal carotid artery; RV, right vertebral artery; SCA, superior cerebellar artery; VA, vertebral artery.
Treatment
Under roadmap guidance, a 0.014-inch microwire was carefully steered through the occlusion to the left PCA. A 2.5×13 mm balloon-expandable stent (Apollo stent system, MicroPort Medical, Shanghai, China) was advanced to the occlusion over the microwire (figure 2C). The stent was released by gradual balloon inflation up to 6 atm within 15 s. At 2 hours after admission, complete recanalisation (TICI 3) of BA was achieved (figure 2D). After the endovascular therapy, oral administration of aspirin, clopidogrel and atorvastatin were initiated.
Outcome and follow-up
Neurological deficits of the patient resolved rapidly within 2 weeks and NIHSS score at 1 month follow-up was only 2. The injured CST, visualised by diffusion tensor imaging (DTI) using FiberTrak software (Philips Healthcare, Amsterdam, The Netherlands), recovered to normal level during a 3-month follow-up (figure 1G–I). Repeated cerebral angiography demonstrated that the stent was patent along its whole length and there was no sign of stent deformity or in-stent thrombosis over a follow-up of 1 year (figure 2E–H).
Discussion
BAO is one of the most devastating forms of ischaemic stroke. Without rapid and timely revascularisation of occluded BA, the patients have a negligible chance of good functional outcome and the mortality was high.1 2 Although a favourable outcome has been reported in scattered BAO cases with delayed reperfusion3 and the therapeutic time window has been extended to 24 hours,4 there is a lacking of in vivo evidences supporting these results and recommendations. In this study, we performed emergency stent angioplasty in a patient with BAO. Complete recanalisation of BA, together with the collaterals from anterior circulation led to a very good outcome. The primary purpose of the surgery was to rescue the salvageable penumbra area. However, we were surprised to find out that the injured CSTs, which passed through the pontine infarct, also benefited from the reperfusion and even recovered to normal level. As far as we know, no similar cases have been reported. For the first time, we provided in vivo evidence that the white matter infarct was still salvageable even after delayed reperfusion.
The therapeutic target of acute ischaemic stroke has always been the penumbra area. The collateral circulation together with the duration of occlusion determines the existence, the volume and the evolvement of penumbra.5–7 The infarct core, no matter cerebral cortex or white matter, has never been thought to be salvageable or taken as therapeutic target, as long as the ischaemia persists for over 1 hour.8 This is the truth for cerebral cortex but cerebral white matter was more resistant to ischaemia9 10 and thus may require alternative therapeutic strategies.10 In this study, we followed up microstructure change of the ischaemic CST after the emergency stent angioplasty. We found that it could still recover to normal after delayed reperfusion. We proposed that brainstem white matter may serve as a novel target for the treatment of acute BAO.
This case has several limitations. First, DTI imaging is subject to artefact such that loss of apparent integrity of white matter tracts does not necessarily correlate directly with damage to underlying myelin or axons but may rather represent attenuation from vasogenic (rather than cytotoxic) oedema. It therefore remains a matter of debate whether the observed improvement on DTI imaging actually represented underlying physiological improvement in the reconstitution of these tracts or simply ‘unmasking’ of the tracts by the resolving vasogenic oedema related to the infarct. The other limitation of DTI currently is the lack of standardisation across different software programmes and differences in results of these programmes among different MRI vendors as well as the dependence of image quality on the strength of the magnet. Until such standardisation is achieved, any inferences with respect to white matter tracts based solely on DTI imaging should be viewed with circumspection.
In conclusion, here we reported a rare case of BAO that was successfully treated by acute stent angioplasty. Complete recovery of the patient was achieved, accompanied with the recovery of the injured CSTs. This case demonstrated that ischaemic white matter was still salvageable even after complete and prolonged ischaemia. It provided a brand new therapeutic target for acute BAO and it would prompt re-evaluations of the time window for BAO. This case report suggests significant implications on prognosis and potential future treatment paradigms related to basilar occlusions and certainly merit further investigation.
References
Footnotes
XL and YW contributed equally.
Contributors XL, YW and JY evaluated the condition of the patient and prepared him for the emergency recanalisation surgery. PW performed the stent angioplasty surgery for the patient. JY and ZW followed up the neuroimaging profiles of the patient. YW and CS wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Ethics approval Ethics Committee of Guangdong 999 Brain Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.