Article Text

Abstract
Offering routine carotid endarterectomy (CEA) or carotid artery stenting (CAS) to patients with asymptomatic carotid artery stenosis (ACS) is no longer considered as the optimal management of these patients. Equally suboptimal, however, is the policy of offering only best medical treatment (BMT) to all patients with ACS and not considering any of them for prophylactic CEA. In the last few years, there have been many studies aiming to identify reliable predictors of future cerebrovascular events that would allow the identification of patients with high-risk ACS and offer a prophylactic carotid intervention only to these patients to prevent them from becoming symptomatic. All patients with ACS should receive BMT. The present article will summarise the evidence suggesting ways to identify these high-risk asymptomatic individuals, namely: (1) microemboli detection on transcranial Doppler, (2) plaque echolucency on Duplex ultrasound, (3) progression in the severity of ACS, (4) silent embolic infarcts on brain CT/MRI, (5) reduced cerebrovascular reserve, (6) increased size of juxtaluminal hypoechoic area, (7) identification of intraplaque haemorrhage using MRI and (8) carotid ulceration. The evidence suggests that approximately 10%–15% of patents with asymptomatic stenosis might benefit from intervention; this will become more clear after publication of ongoing studies comparing stenting or endarterectomy with best medical therapy. In the meantime, no patient should be offered intervention unless there is evidence of high risk of ipsilateral stroke, from modalities such as those discussed here.
- asymptomatic carotid stenosis
- stroke risk
- carotid endarterectomy
- best medical therapy
- identification of high risk subgroups
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- asymptomatic carotid stenosis
- stroke risk
- carotid endarterectomy
- best medical therapy
- identification of high risk subgroups
Introduction
There are almost 800 000 strokes each year in USA, causing about 140 000 deaths annually.1 About 610 000 of these are first strokes.1 Similarly, in UK, there are more than 100 000 strokes/year.2 In 2015 alone, over 40 000 people died of stroke in UK.2 Stroke causes twice as many deaths/year in women than breast cancer and twice as many deaths/year in men than prostate and testicular cancer combined.2 Stroke is the second most common cause of death in the world, causing around 6.7 million deaths each year (or one death every 5 s).2 About 85% of all strokes are ischaemic and 15% are haemorrhagic.2 Thromboemboli originating from an ipsilateral asymptomatic carotid stenosis (ACS) are the cause of a substantial proportion of first-ever ischaemic strokes.
As a result of three landmark randomised controlled trials showing that carotid endarterectomy (CEA) conferred a 50% relative risk (RR) reduction in the 5-year stroke risk compared with best medical treatment (BMT) alone,3–5 offering CEA routinely to patients with ACS was considered as the treatment-of-choice in the 1980s and 1990s. In the early and mid-2000s, however, this began to change. Due to improvements in BMT (eg, smoking cessation strategies, implementation of statins and so on), the number of cerebrovascular events/year (ie, the annual stroke rate) among patients with ACS declined significantly.6 7 It therefore became apparent that offering CEA routinely to patients with ACS was no longer optimal management. At the same time, however, the opposite theory supporting BMT alone as the treatment-of-choice for all patients with ACS and condemning prophylactic CEA for any patient with ACS8 9 is equally suboptimal and misleading. This theory is not based on Level I Evidence; it is an extrapolation from the improved results achieved with current BMT in various observational studies and meta-analyses.
In the last few years, several methods have been proposed as reliable predictors for the identification of ACS individuals at high risk of stroke. For some of these predictors, the evidence is adequate and robust, whereas for others it is weaker. The current article will outline methods to identify which asymptomatic carotid patients could benefit from a prophylactic carotid intervention.
Microemboli detection on transcranial Doppler (TCD)
The predictive value of microemboli detection on TCD for the identification of patients with ACS at high risk for future stroke is well-established. Spence et al first reported that patients with ACS with >2 microemboli/hour on TCD had a >1500% increased risk of 1-year ipsilateral ischaemic stroke compared with patients with ACS without TCD-detected microemboli (15.6% vs 1.0%, respectively; P<0.0001).6 Figure 1 shows a microembolus. In 2010, the same group reported that as a result of improvements in BMT, there was a marked reduction in TCD-detected microemboli (12.6% before 2003 vs 3.7% after 2003; P<0.001) and in cardiovascular events (17.6% before 2003 vs 5.2% after 2003; P<0.001) in 468 patients with ACS.6 A few months later, these results were verified in an independent multicentre international study on 467 patients with ACS, the Asymptomatic Carotid Emboli Study (ACES).10 As in the study by Spence et al,6 patients participating in ACES also had two 1-hour TCD recordings 1 week apart.10 Patients with one or more TCD emboli had a >550% higher risk of 1 year ipsilateral stroke compared with patients without emboli (HR: 5.57; 95% CI 1.61 to 19.32; P=0.007).10

Transcranial Doppler embolus detection. Microembolus in a patient with asymptomatic carotid stenosis. The upper channel is an M-mode image of an embolus in the middle cerebral artery; the lower panel shows the high-intensity transit signal in the Doppler channel. Besides the visual appearance of the microembolus, a characteristic clicking sound is heard. (Reproduced by permission of the Society for Vascular Ultrasound from: Spence JD. Transcranial Doppler: uses in stroke prevention. The Journal for Vascular Ultrasound 2015;39:183–7.)
Contradictory results had been earlier reported by a small prospective, observational, cohort study.11 This early study showed a trend to higher stroke risk in patients with ACS with microemboli, but was underpowered, with only 202 patients.11 Besides the small sample size, another likely reason for the negative results of this study was that it accepted one microembolus as positive, and the test was repeated at 6-monthly intervals.11 There is compelling evidence that at least two embolic signals detected in a recording lasting 1 hour identifies patients with ACS at very high risk of stroke,12 13 suggesting a high-risk, unstable asymptomatic plaque or a plaque with a thrombus on its surface.13
TCD embolus detection is currently the best validated method for the identification of high-risk patients with ACS.14 This is also supported by a meta-analysis including five prospective studies (n=677 patients).15 In this meta-analysis, the presence of TCD-detected embolic signals in patients with ACS was a significant predictor of ipsilateral stroke (OR: 7.46; 95% CI 2.24 to 24.89; P=0.001).15 The 2017 European Society for Vascular Surgery carotid guidelines recommend intervention based on TCD microemboli.16
Plaque echolucency on Duplex ultrasound
Early studies from the 1990s demonstrated that carotid plaque echolucency corresponds to lipid-rich necrotic core or intraplaque haemorrhage, more commonly found in patients with symptomatic rather than ACS.17 18 Several studies evaluated whether or not carotid plaque echolucency was associated with increased risk of future stroke in patients with ACS (table 1).19–26
Studies evaluating the association between carotid plaque echolucency and risk of ipsilateral stroke
The majority of studies independently reported a strong association between plaque echolucency and increased risk of stroke in patients with ACS.19–21 23–26 The only exception was a study from Denmark which demonstrated that carotid plaque echolucency was positively associated with risk of future stroke in patients with symptomatic, but not with ACS.22
A recent meta-analysis (7557 patients; mean follow-up: 37.2 months) demonstrated a positive association between plaque echolucency and the risk of future ipsilateral stroke (RR: 2.31; 95% CI 1.58 to 3.39; P<0.001).27 Of the total study sample, 1741 patients (23.0%) had a positive ultrasound test for echolucency, whereas 5816 (77.0%) had a negative test for echolucency. A total of 100 ipsilateral strokes occurred in the echolucent-positive test group, while 141 ipsilateral strokes occurred in the echolucency-negative test group (cumulative incidence of ipsilateral stroke: 5.7% vs 2.4%, respectively). In patients with ≥50% carotid stenosis, the stroke risk was higher (RR: 2.61; 95% CI 1.47 to 4.63; P=0.001).27 The association between carotid plaque echolucency and increased risk of future ipsilateral stroke was verified in an independent meta-analysis.28
The predictive value of echolucent plaque morphology on carotid ultrasound increases even further if it is combined with TCD-detected emboli.24 In ACES,24 carotid plaque echolucency was associated with a >600% increased risk of ipsilateral risk (HR: 6.43; 95% CI 1.36 to 30.44; P=0.019), while the combination of plaque echolucency with TCD-detected emboli was associated with a >1000% increased risk of ipsilateral stroke (HR: 10.61; 95% CI 2.98 to 37.82; P=0.0003).24
Progression of the severity of stenosis
Most would agree that the progression of the severity of ACS in successive ultrasound examinations despite the implementation of BMT is not a good sign. Several reasons may account for ACS progression despite BMT. Up to half of patients with ACS may have ‘resistant atherosclerosis’.29
The largest prospective study on patients with ACS undergoing medical intervention alone, the Asymptomatic Carotid Stenosis and Risk of Stroke (ACSRS) study,30 demonstrated quite clearly that progression in the severity of ACS was a predictor of future stroke. As shown in ACSRS,30 the 8-year cumulative ipsilateral ischaemic stroke rate was 0% in patients with regression of stenosis, 9% if the stenosis was unchanged and 16% if there was progression of stenosis. In the subgroup with unchanged stenosis, the 8-year cumulative ipsilateral cerebral ischaemic stroke rates for patients with baseline stenosis of 50%–69%, 70%–89% and 90%–99% were 4%, 8% and 13%, respectively.30 In contrast, in the presence of progression, the stroke rate was 8%, 15% and 25%, respectively.30
An independent study from Boston, Massachusetts, verified that progression of ACS despite BMT is not a good prognostic factor.31 In this study, 794 patients (900 carotid arteries) with moderate (50%–69%) ACS had a mean follow-up of 3.6 (range: 0.3–6.7) years. Stenosis progression occurred in 262 of 900 (29.1%) carotid arteries despite BMT and 36 (13.7%) of these developed symptoms. The symptomatic conversion rate in patients with stenosis progression was considerably higher than of those without stenosis progression (13.7% vs 8.5%, respectively; P=0.02). Overall, BMT failed to prevent carotid disease progression or the development of ipsilateral neurologic symptoms in a significant proportion of the patient cohort.31
These results once again verify the results of an earlier study on 1065 patients with ACS followed up with carotid ultrasound.32 During the initial study period of a median 7.5 (range: 6–9) months, progression of carotid lesions was demonstrated in 93 of 1065 patients (9%). During a median follow-up of 3.2 (IQR: 2.9–3.5) years, 495 major adverse cardiovascular events (a composite of myocardial infarction (MI), percutaneous coronary intervention, coronary artery bypass graft, stroke, peripheral percutaneous angioplasty, peripheral vascular surgery, amputation due to critical limb ischaemia and all-cause mortality) were recorded in 421 patients (40%). Patients with progressive ACS had a 200% higher risk for composite major adverse cardiovascular events compared with patients with non-progressive disease (adjusted HR: 2.01; 95% CI 1.48 to 2.67; P<0.001), consisting of a >200% higher risk of MI (HR: 2.38; 95% CI 1.07 to 5.35; P=0.044), a 200% higher risk for stroke (adjusted HR: 2.0; 95% CI 1.02 to 4.11; P=0.035) and a 175% higher risk for cardiovascular death (adjusted HR: 1.75; 95% CI 1.03 to 2.97, P=0.039).32
Progression of carotid plaque burden may be a better predictor of cardiovascular outcomes than carotid intima-media thickness (cIMT). A study from Canada compared the progression/regression of cIMT, total plaque area and total plaque volume as predictors of cardiovascular outcomes in 349 patients attending stroke prevention clinics.33 After a median follow-up of 3.17 (range: 0.07–5.0) years, there were 50 first events: 20 vascular deaths, 11 strokes, 13 transient ischaemic attacks (TIAs) and 6 MIs. Progression of total plaque volume predicted stroke, death or TIA (P=0.001), stroke, death or MI (P=0.008) and stroke, death, TIA or MI (P=0.001). Progression of total plaque area weakly predicted stroke, TIA or death (P=0.097), but not stroke, death or MI (P=0.59) or TIA, stroke, death or MI (P=0.143). Similarly, change in cIMT did not predict stroke, death or MI (P=0.13) or TIA, stroke, death or MI (P=0.455). By Cox regression analysis using a backward stepwise Wald approach, total plaque volume progression remained a significant predictor of events after adjustment for coronary risk factors (P=0.001). This study showed that measurement of total plaque volume is a superior predictor of cardiovascular events that either total plaque area or cIMT.33 In patients with ACS, plaque burden, but not per cent stenosis, predicted the risk of stroke.34 In the High Risk Plaque BioImage study,35 plaque burden was strongly correlated with coronary calcium whereas IMT was not, and plaque burden was as predictive of events as coronary calcium.36
Silent embolic infarcts on brain CT or MRI
Both the Cardiovascular Health Study37 and the Rotterdam Scan Study38 demonstrated that the presence of silent embolic infarcts on brain CT or MRI scans is associated with an increased risk of stroke in the general population. Two studies (ACSRS39 and an independent study from Japan)40 showed that silent embolic infarcts on brain CT or MRI are an independent predictor of stroke. In ACSRS, patients with 60%–99% ACS having silent embolic infarcts on brain CT scans had a 300% higher risk of future ipsilateral stroke compared with patients without silent embolic infarcts (annual stroke rate: 3.6% vs 1.0%, respectively; HR: 3.0; 95% CI 1.46 to 6.29; P=0.002).39
These results suggest that the presence of silent infarcts on brain CT or MRI in patients with ACS reliably identifies patients with ACS at high risk for a future ipsilateral cerebrovascular event. However, one of the limitations of brain CT scans is that they may miss up to 40% of brain infarcts in patients with ACS.41
Reduced cerebrovascular reserve (CVR)
With increasing degree of carotid stenosis, cerebral perfusion pressure is reduced. By the mechanism of autoregulation of the cerebral vasculature, the cerebral arterioles dilate maximally to maintain cerebral blood flow. With further reduction in cerebral perfusion pressure (such as may occur during a hypotensive episode), the cerebral blood flow will also decrease and potentially increase the risk of stroke. Several studies have demonstrated that impairment in CVR is associated with the development of stroke in patients with ACS (table 2).42–46
Association between impaired CVR and the development of stroke in patients with asymptomatic carotid stenosis
Normal CVR values range from as low as 15% and up to 40%. Values below 10% suggest impaired CVR.47 A meta-analysis (n=13 studies; 991 patients; mean follow-up: 32.7 months) on the association between CVR impairment with stroke risk demonstrated an almost 400% higher stroke risk in asymptomatic patients with impaired cerebral blood flow (random effects OR: 3.96; 95% CI 2.60 to 6.04).47 A limitation of this meta-analysis was that in the majority of the studies the investigators were not blinded to the CVR results. Additionally, the definition of study end-points (stroke or TIA) varied between studies as well as the definition of asymptomatic versus symptomatic disease. Despite these potential limitations, the authors concluded that the preservation of the association between CVR impairment and risk of stroke/TIA is robust. Reduced CVR may therefore identify patients with ACS at high risk for stroke.
Size of juxtaluminal hypoechoic area
In unstable symptomatic plaques, the necrotic core is twice as close to the lumen compared with asymptomatic carotid plaques.48 Cross-sectional studies using ultrasound have demonstrated an association between the juxtaluminal hypoechoic (black) area and the presence of neurological symptoms.49–51
The ACSRS tested the hypothesis that the presence and size of a juxtaluminal hypoechoic area in the absence of a visible echogenic cap predicts future ipsilateral ischaemic stroke in patients with ACS.52 The 5-year ipsilateral cerebral or retinal ischaemic event rate was 3% in patients with a juxtaluminal hypoechoic area <4 mm2, 21% in patients with an area between 4 and 8 mm2, 36% in patients with an area 8–10 mm2 and 43% in patients with a juxtaluminal black area>10 mm2 (average annual rates: 0.6%, 4.2%, 7.2% and 8.6%, respectively).52 These results support the theory that the size of juxtaluminal hypoechoic area may be a predictor of future ipsilateral ischaemic stroke.
Identification of intraplaque haemorrhage using MRI
Several studies have evaluated whether or not MRI assessment of specific components of the carotid plaque can be used to predict stroke in patients with ACS (table 3).
Studies evaluating the risk of stroke in patients with ACS using carotid plaque MRI
In some of these studies, the authors described blinding of MRI results to researchers who assessed ischaemic outcomes53 54 55 whereas such blinding was not reported in others.56–58 The majority of the studies showed that carotid plaques with intraplaque haemorrhage, lipid-rich necrotic core or thinning/rupture of the fibrous cap are significantly more likely to result in ipsilateral ischaemic events with this increased risk present across a wide range of stenosis severity.
The ability of carotid intraplaque haemorrhage, lipid-rich necrotic core and thinning/rupture of the fibrous cap to predict future ipsilateral ischaemic stroke was verified in a meta-analysis (n=9 studies; 779 patients).59 The HRs (95% CI) for intraplaque haemorrhage, lipid-rich necrotic core and thinning/rupture of the fibrous cap as predictors of subsequent stroke/TIA were 4.59 (2.91–7.24), 3.00 (1.51–5.95) and 5.93 (2.65–13.20), respectively. This meta-analysis concluded that MRI characterisation of these specific plaque elements can provide additional measures of stroke risk not provided by simple measurement of luminal stenosis. These results suggest that carotid plaque MRI may be used to select high-risk groups that may benefit from revascularisation.
Carotid ulceration
The North American Symptomatic Carotid Endarterectomy Trial showed that ulceration on angiography was associated with up to a 350% higher RR of stroke.60 A study from Canada showed that, in ACS, compared with no ulcers, the presence of three or more ulcers (the sum of both carotids) predicted the 3-year risk of stroke or death (18.2% vs 1.7%, p = 0.03 respectively) to a similar degree as microemboli (20% vs 2.0%, p = 0.003).61 Ulcer volume also predicts risk among patients attending a stroke prevention clinic (figure 2). Contrast-enhanced ultrasound is superior to colour Doppler ultrasound for the detection of ulcerated plaques.62 Contrast-enhanced ultrasound can be used to identify the ‘vulnerable carotid plaque’ associated with high embolic potential.63 Three-dimensional carotid ultrasound-based texture analysis is another way to evaluate both the composition of the carotid plaque and to predict vascular events.64 65
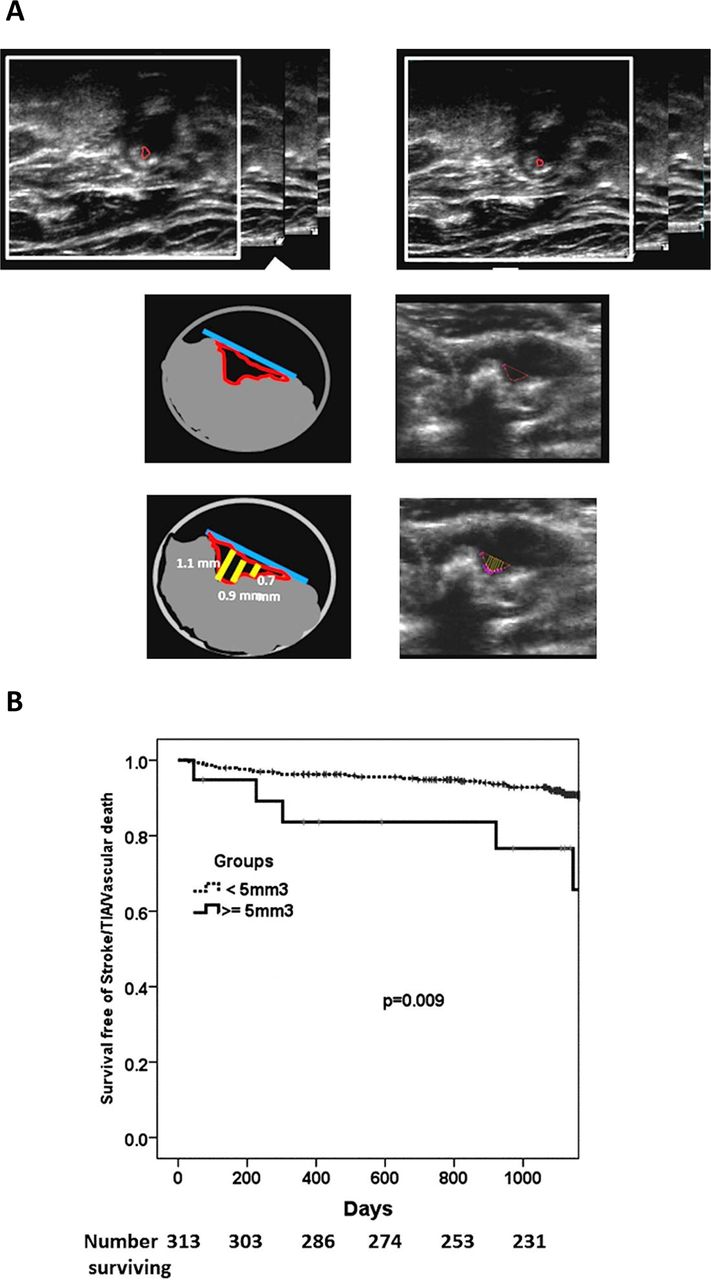
Carotid ulcer volume as a predictor of risk. (A) Measurement of ulcer volume and ulcer depth. Contours of ulcers were traced and depth of ulcers measured in cross-sectional views. Each slice had a thickness of 1 mm; total ulcer volume (TUV) was computed from the sum of the volumes of all slices in which ulceration was traced. (B) Kaplan–Meier survival analysis curves for participants with TUV≥5.00 mm3 and those with no ulcerations or TUV<5 mm3. Time is shown in days until the first occurrence of any of the following events: stroke, TIA or cardiovascular death during the duration of follow-up; log-rank P=0.009. TIA, transient ischaemic attack; TUV, total ulcer volume. (Reproduced by permission of Wolters Kluwer Health. from: Kuk M, Wannarong T, Beletsky V, Parraga G, Fenster A, Spence JD. Volume of Carotid Artery Ulceration as a predictor of Cardiovascular Events. Stroke 2014;45:1437–41.)
What is the % of asymptomatic patients who could benefit from intervention?
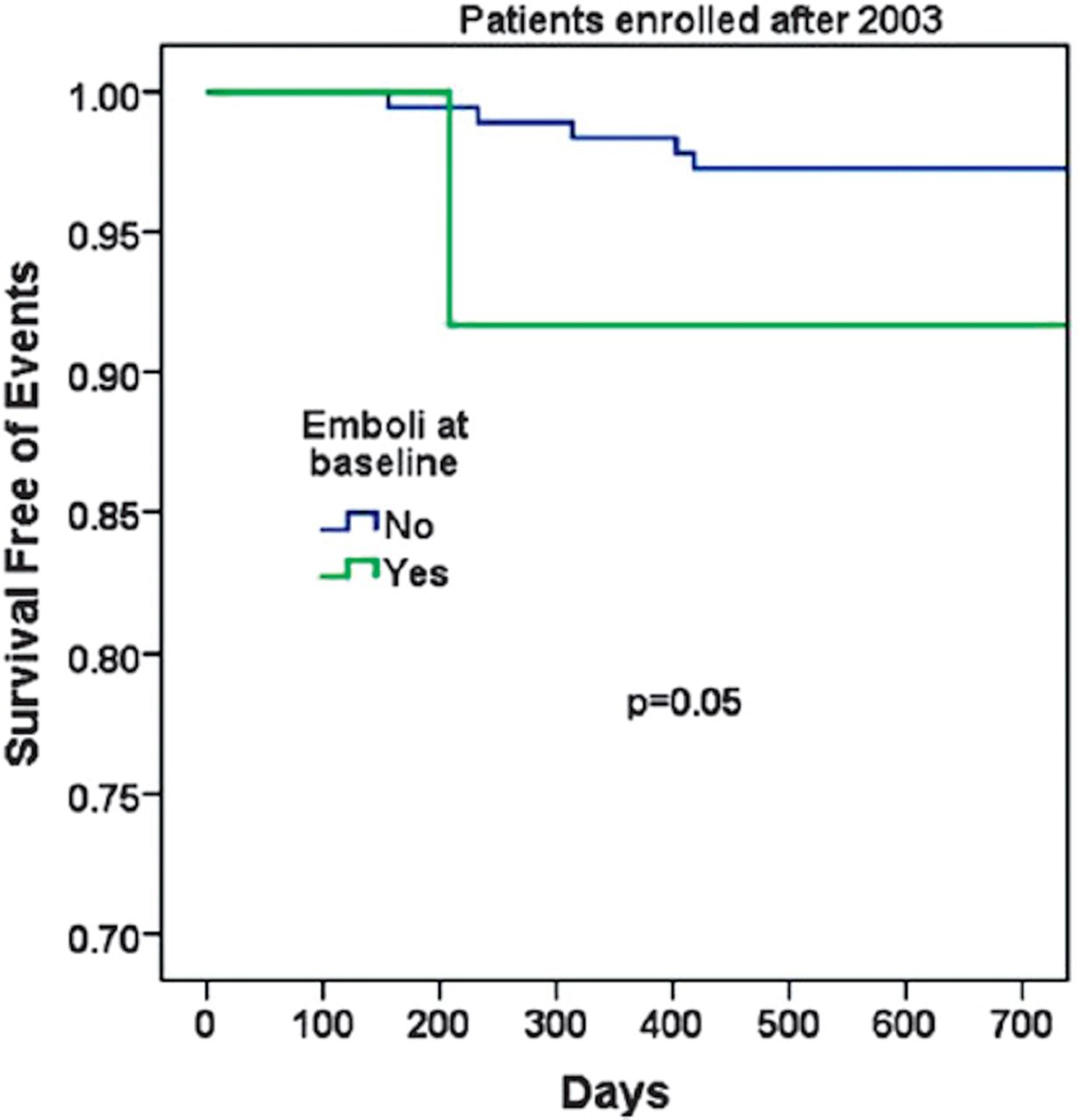
In 2005, Spence et al reported that in a period from 2000 to 2005, 10% of patients with ACS had two or more microemboli, with a 15.6% 1-year risk of stroke.6 In 2010, they reported that this had declined from 12.6% before 2003 to 3.7% after 2003 with more intensive medical therapy implemented in that clinic, based on ‘treating arteries instead of risk factors’.7 Two or more microemboli still predicted a higher risk of stroke after 2003 (figure 3). It should be noted that the intensive medical therapy in that clinic after 2003 was much more intensive than in most clinics around the world; it is described in detail in a study reporting the low risk of stroke at the time of a new carotid occlusion.34 Part of the process includes showing patients pictures of their plaque and explaining that their disease is much worse than that of healthy people of the same age and sex. Doing so has been shown to improve compliance with medical advice by 400%.66

Event-free survival in asymptomatic carotid stenosis with and without microemboli on transcranial Doppler since 2003. After more intensive medical therapy based on ‘treating arteries’, two or more microemboli on TCD remained a significant predictor of stroke/TIA/death, but to a lesser degree than before 2003. TIA, transient ischaemic attack; TCD, transcranial Doppler. (Reproduced by permission of the Society for Vascular Ultrasound from: Spence JD. Transcranial Doppler: uses in stroke prevention. The Journal for Vascular Ultrasound 2015;39:183–7.)
ACES10 reported that 16.5% of patients with ACS had one or more microemboli, but this was observed on repeated TCD embolus detection studies over 18 months; the risk of ipsilateral stroke in the 2 years following baseline microembolus detection was 3.62% in patients with embolic signals versus 0.70% without.10 In the study of 3D ultrasound detection of carotid ulceration described above,6110% of patients had either three or more ulcers or microemboli, with comparable risks and, surprisingly, these did not overlap by much: only 1.2% of patients with ACS had both two or more microemboli and three or more ulcers. However, some of these patients were studied before implementation of intensive medical therapy in 2003. In 2009, Singh et al reported intraplaque haemorrhage in 36.7% of 98 carotid arteries with moderate asymptomatic stenosis.53 In a larger pathological study of endarterectomy specimens, intraplaque haemorrhage was observed in 69.9% of plaques from patients who had been asymptomatic prior to surgery.67 It is likely that many of the pathologically observed haemorrhages may have been too small for detection on MRI or ultrasound.
It seems reasonable to assume that some of the other features that predict risk of stroke, such as reduced CBF reserve, intraplaque haemorrhage and plaque inflammation, will also not overlap with microemboli or ulceration, so approximately 10%–15% of patients with ACS could benefit from CEA or carotid artery stenting (CAS) despite intensive medical therapy.16 No patient with asymptomatic stenosis should be offered intervention in the absence of such evidence. In most cases, particularly in the elderly, CEA is associated with a lower risk of stroke compared to CAS. Another paper in this issue of the journal will review that topic.
Conclusion
Current evidence suggests that certain patients with ACS (eg, those with TCD-detected microemboli, silent embolic infarcts on brain CT/MRI scans, reduced CVR, ACS severity progression despite BMT, size of black juxtaluminal plaque area≥8 mm2 without a visible echogenic cap and intraplaque haemorrhage on MRI) are at increased stroke risk and should be considered for prophylactic CEA or CAS.16 68 The 2017 guidelines by the European Society for Vascular Surgery recommend that in average surgical risk patients with a 60%–99% ACS, CEA (Class IIa; Level of Evidence: B) or CAS (Class IIb; Level of Evidence: B) should be considered for intervention in the presence of one or more imaging characteristics that may be associated with an increased risk of late ipsilateral stroke (table 4), provided documented perioperative stroke/death rates are <3% and the patient’s life expectancy exceeds 5 years.16
Clinical/imaging features associated with an increased risk of late stroke in patients with 50%–99% asymptomatic carotid stenosis treated medically in the 2017 European Society for Vascular Surgery carotid guidelines16
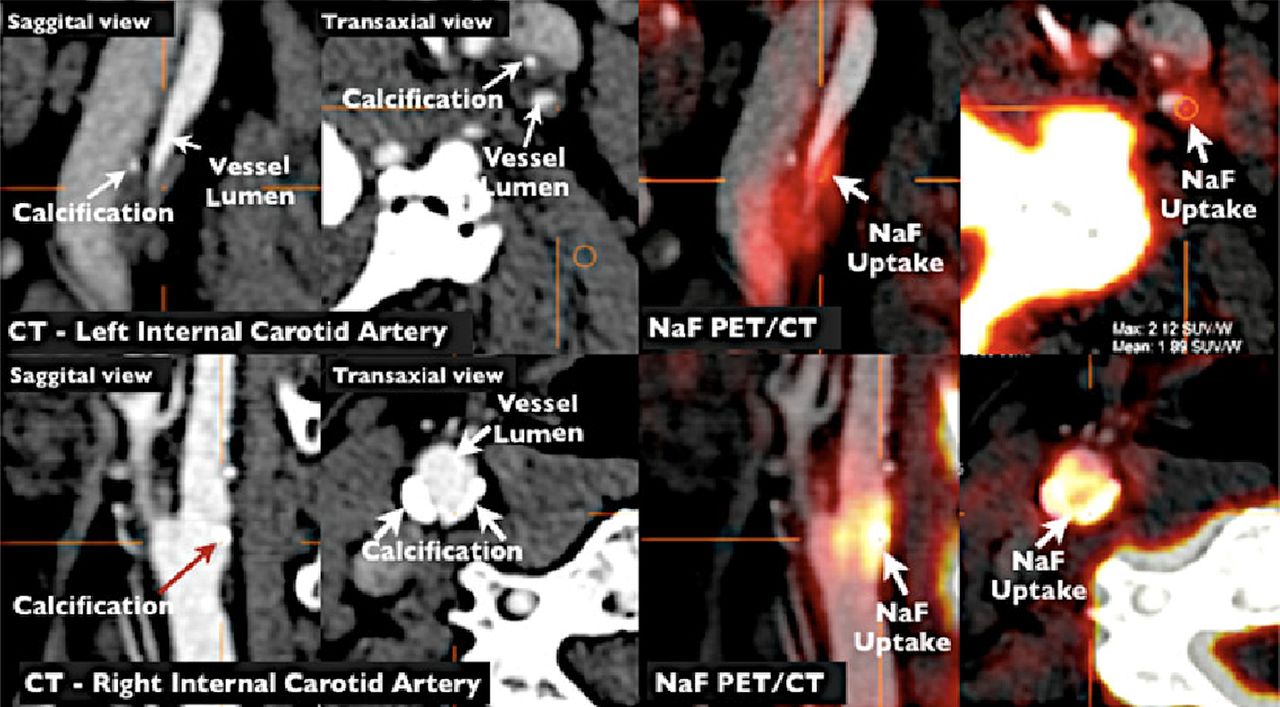
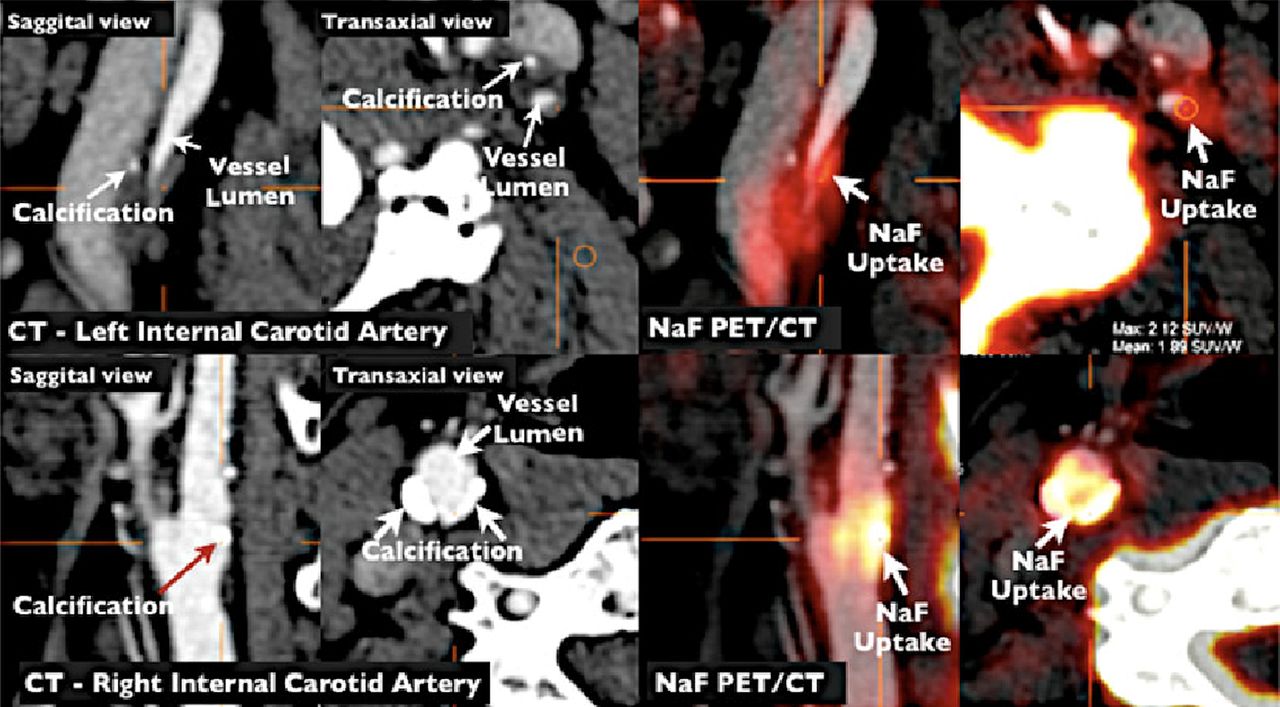
This is a new recommendation taking into account the increased stroke risk of these patients with ACS managed with BMT alone. Further research on the above (and other) possible predictors of ischaemic stroke in patients with ACS such as plaque texture,65 plaque neovascularity69 70 and plaque inflammation or active calcification (figure 4) on PET/CT71 is essential in order to appropriately select for carotid revascularisation procedures the few patients with ACS who could benefit from these procedures. Two ongoing trials comparing BMT with CEA or CAS are under way; when those studies have been completed, we will have better evidence about the role of intervention versus medical therapy in ACS.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Imaging of active calcification by PET/CT with [18]F Sodium Fluoride. NaF PET/CT imaging of left and right internal carotid arteries of active calcification in a 72-year-old symptomatic patient evaluated at the University of Ottawa Heart Institute. Upper row: evidence of NaF uptake with a small foci of calcification on CT in the left internal carotid symptomatic culprit vessel. There is a mismatch between the region of NaF uptake and calcification on CT. Lower row: evidence of calcium nodules with matched NaF uptake at the right internal carotid artery. PET, positron emission tomography. (Reproduced by permission of the Journal of Nuclear Cardiology from: Cocker MS, Mc Ardle B, Spence JD, et al. Imaging atherosclerosis with hybrid [(18)F]fluorodeoxyglucose positron emission tomography/CT imaging: What Leonardo da Vinci could not see. J Nucl Cardiol 2012;19:1211–25.)
References
Footnotes
Contributors KIP wrote the first draft. FJV and JDS made revisions.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Guest chief editor J David Spence