Article Text

Abstract
Historically, because of the difficulty of using warfarin safely and effectively, many patients with cardioembolic stroke who should have been anticoagulated were instead given ineffective antiplatelet therapy (or no antithrombotic therapy). With the arrival of new oral anticoagulants that are not significantly more likely than aspirin to cause severe haemorrhage, everything has changed. Because antiplatelet agents are much less effective in preventing cardioembolic stroke, it is now more prudent to anticoagulate patients in whom cardioembolic stroke is strongly suspected. Recent advances include the recognition that intermittent atrial fibrillation is better detected with more prolonged monitoring of the cardiac rhythm, and that percutaneous closure of patent foramen ovale (PFO) may reduce the risk of stroke. However, because in most patients with stroke and PFO the PFO is incidental, this should be reserved for patients in whom paradoxical embolism is likely. A high shunt grade on transcranial Doppler saline studies, and clinical clues to paradoxical embolism, can help in appropriate selection of patients for percutaneous closure. For patients with atrial fibrillation who cannot be anticoagulated, ablation of the left atrial appendage is an emerging option. It is also increasingly recognised that high levels of homocysteine, often due to undiagnosed metabolic deficiency of vitamin B12, markedly increase the risk of stroke in atrial fibrillation, and that B vitamins (folic acid and B12) do prevent stroke by lowering homocysteine. However, with regard to B12, methylcobalamin should probably be used instead of cyanocobalamin. Many important considerations for judicious application of therapies to prevent cardioembolic stroke are discussed.
- cardioembolic
- atrial fibrillation
- anticoagulants
- percutaneous closure of patent foramen ovale
- direct-acting oral anticoagulants
- warfarin
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- cardioembolic
- atrial fibrillation
- anticoagulants
- percutaneous closure of patent foramen ovale
- direct-acting oral anticoagulants
- warfarin
The two most common mistakes I see being made in secondary prevention occur when a patient has a stroke or transient ischaemic attack (TIA) while taking aspirin. The two mistakes are either to double the dose of aspirin, or switch the patient to clopidogrel. These are mistakes on several levels. Low-dose aspirin is more effective than high-dose aspirin,1 probably because only a very low dose of aspirin is necessary to permanently inactivate all the platelets in circulation; this happens because of acetylation of platelet thromboxane, with platelets unable to recover because they lack a nucleus. Endothelial cells, on the other hand, have a nucleus, so can recover from the effect of aspirin by making more prostacyclin, which inhibits platelet aggregation on the endothelium. The higher the dose of aspirin, the longer it takes the endothelium to recover.
Switching aspirin to clopidogrel is a mistake because adding it would be more effective if antiplatelet therapy were indicated, and many patients have a loss-of-function variant of CYP2C9, which is required to convert the prodrug clopidogrel to its active form: ~30% of Europeans, and more than half of Chinese have this variant, and clopidogrel is less efficacious in those patients.2 This problem can be avoided by using ticagrelor.3 (Another article in this series discusses antiplatelet therapy in more detail.)
On a more fundamental level, if a patient has a stroke or TIA while taking aspirin, it should be assumed that antiplatelet therapy may not be what the patient needs: the cause of the stroke needs to be considered, and appropriate therapy given.4 For giant cell arteritis the appropriate therapy is prednisone; for cardioembolic stroke it is anticoagulation.
In the past, the paradigm for anticoagulation in secondary stroke prevention was that anticoagulation would seldom or never be prescribed without convincing evidence that the stroke was cardioembolic, such as detection of atrial fibrillation on an ECG or Holter recording. Much or most of the resistance to using anticoagulation was based on the risk of haemorrhage from warfarin, and the difficulty of controlling warfarin dosing so as to maintain target levels of anticoagulation. Now, everything has changed.
Perhaps the most important change has been the availability of new direct-acting oral anticoagulants (DOAC), which are no more likely than antiplatelet agents to cause severe haemorrhage. Besides the availability of DOACs, several additional important changes have occurred in relation to cardioembolic stroke: the construct of embolic stroke of unknown source (ESUS),5 the recognition that Holter recordings often miss intermittent atrial fibrillation,6 improved detection and risk stratification of patent foramen ovale (PFO) with transcranial Doppler embolus detection,7 the recognition that percutaneous closure of PFO is more beneficial compared with antiplatelet agents, versus anticoagulants, and the recognition that elevated levels of total homocysteine (tHcy), which quadruple the risk of stroke in atrial fibrillation, are commonly due to undiagnosed metabolic deficiency of vitamin B12,8 which should be treated not with cyanocobalamin, but with methylcobalamin.9 (Another article in this series discusses B vitamin therapy to lower homocysteine.)
Diagnosis of cardioembolic stroke
In the past, the concept of ‘cryptogenic stroke’ was used to define strokes not due to known causes such as a known cardiac source of emboli, large artery disease, lacunar strokes due to hypertension or diabetes, or due to other known causes. It was a diagnosis of exclusion, after negative investigations including arterial imaging, brain imaging and cardiac investigations including echocardiography and a Holter recording. In 2014, Hart et al 5 proposed the construct of ESUS, defined as ‘non-lacunar brain infarct without proximal arterial stenosis or cardioembolic sources, with a clear indication for anticoagulation.’
There has long been a problem with the definition of large artery disease, confined to patients with carotid stenosis of 50% or more. Although it may be intuitive that patients without stenosis do not have much plaque, in fact many patients without carotid stenosis of 50% or more have large artery disease, with a high total plaque area (TPA). This is thought to be due to compensatory enlargement of the artery, as described by Glagov et al.10 In 2002, our group reported that among patients attending vascular prevention clinics, carotid plaque burden in the top quartile of TPA of 119 mm2 or higher had a 19.5% 5-year risk of stroke, myocardial infarction or cardiovascular death.11 In 2004, we reported that TPA was a stronger predictor of risk than per cent stenosis in that population,12 and in 2015 we reported that among patients with asymptomatic carotid stenosis, plaque burden was a stronger predictor of risk than per cent stenosis.13 We therefore developed and validated a new stroke subtype classification that incorporated a TPA>119 mm2 into the definition of large artery disease, as well as stenosis >50%.14 Using that classification, we studied secular trends in stroke subtypes among patients referred to my Urgent TIA Clinic. We found that with improved levels of low-density lipoprotein cholesterol and blood pressure at the time of the referral (therefore reflecting changes in practice in the community), large artery disease and small vessel disease declined, and cardioembolic stroke increased, as a proportion of strokes in our referral population.15 Between 2002 and 2005, 22.8% of strokes were cardioembolic and 45.6% were due to large artery disease; between 2009 and 2012, large artery strokes had declined to 26.6% and cardioembolic stroke had increased to 54.3% of referrals. The increase in cardioembolic strokes highlights the importance of the changes that have happened in relation to anticoagulation.
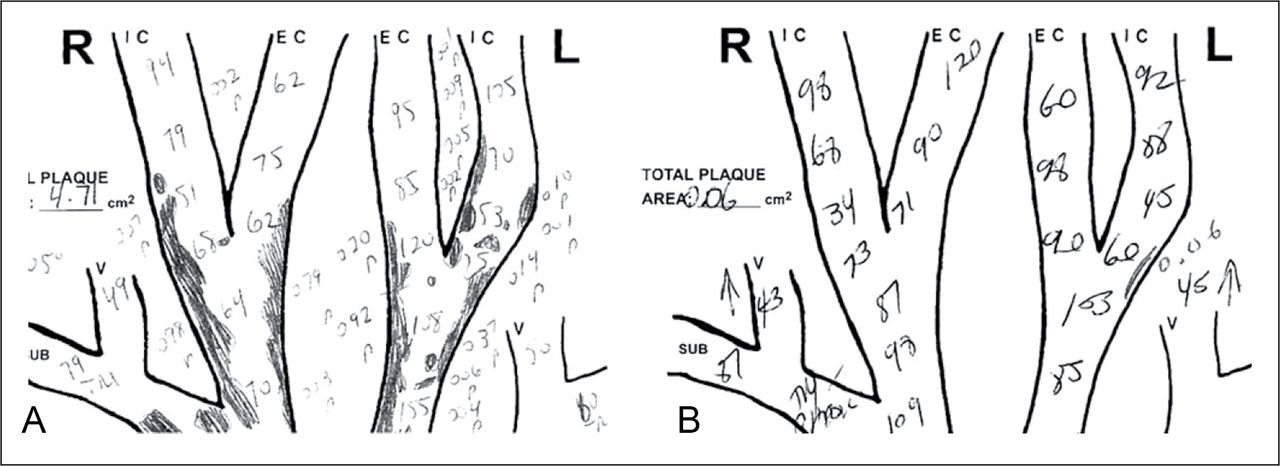
The diagnosis of cardioembolic stroke has two sides to the coin: on the negative side, there is the absence of evidence of another cause of stroke (figure 1). On the positive side, there is evidence of a cardioembolic stroke such as a Holter recording showing intermittent atrial fibrillation, an echocardiogram showing a cardioembolic source such as thrombus in the left atrium, a ventricular aneurysm, ventricular dyskinesia or cardiomyopathy. An additional important consideration is the clinical pattern of cerebral involvement: a patient with cortical ischaemia in multiple vascular territories should be regarded as having a cardioembolic (or aortic atheromatous) source. For example, if a right-handed patient has a left homonymous hemianopsia either simultaneous with or on a separate occasion from an episode of aphasia and weakness of the right arm, this must be regarded as cardioembolic.

Measurement of plaque burden adds to the diagnosis of stroke subtype. (A) Although it may be intuitive that patients without stenosis do not have much plaque, in fact many patients without carotid stenosis of 50% or more have large artery disease, with a high total plaque area (TPA). This is thought to be due to compensatory enlargement of the artery, as described by Glagov et al.10 This composite drawing of carotid plaques from the ultrasound report of a normotensive 79-year-old woman with atherosclerotic stroke shows a very high plaque burden (TPA=4.71 cm2, approximately nine times normal for age and sex); the peak velocities (numbers written into the lumen) show that there was no internal carotid stenosis. (B) In contrast, this composite drawing shows almost no plaque (TPA=0.06 cm2) in a normotensive 72-year-old man with no carotid stenosis and cryptogenic stroke (normal TPA for age and sex would be more than 10 times higher—0.8 cm2). The absence or near absence of plaque in a normotensive patient without diabetes raises the suspicion of a cardioembolic source, dissection or other unusual cause of stroke. L, left; R, right. (Reproduced with permission of Karger from Bogiatzi et al 14).
Because the risk of recurrent stroke is high soon after a cardioembolic event,16 it is more prudent to anticoagulate the patient pending the results of investigations, rather than wait several weeks to anticoagulate the patient after the results are available from an echocardiogram and Holter recording (followed by more prolonged ECG monitoring if the initial Holter is negative).4 Indeed, if there is a strong suspicion of a cardioembolic source, as described above, it is now more prudent to anticoagulate the patient with a DOAC than to persist with antiplatelet therapy. Two trials of this approach in patients with ESUS are in progress.
Importance of anticoagulation for cardioembolic stroke
In considering prevention of cardioembolic stroke, it is crucial to understand that antiplatelet agents are not anticoagulants. Antiplatelet agents prevent formation of white thrombus (platelet aggregates that form in the setting of fast flow, in arteries and perhaps on heart valves). The kind of thrombus that forms in the setting of stasis, such as in the left atrial appendage in atrial fibrillation, in ventricular dyskinesia and in deep veins (leading to paradoxical embolism), is called red thrombus. It results from polymerisation of fibrin, formation of a mesh of long fibrin strands similar to cotton wool, with entrapped red blood cells. To prevent formation of red thrombus it is necessary to use anticoagulants. This is why antiplatelet agents are much less effective than anticoagulants in preventing stroke from atrial fibrillation.
Many physicians are reluctant to prescribe anticoagulants, based on bad experiences with warfarin. Haemorrhage rates are much higher in the real world than in clinical trials, and haemorrhages tend to occur early after initiation of warfarin. Gomes et al reported that among patients with a high risk of stroke from atrial fibrillation, more than 16% had a haemorrhage within 30 days of initiating warfarin.17 This is a serious problem; many studies report that more than half of patients who should be anticoagulated for atrial fibrillation do not receive anticoagulants at all. A higher proportion is not effectively anticoagulated: Gladstone et al 18 reported that among patients with atrial fibrillation and first-ever stroke, after excluding patients with known contraindications to anticoagulation (not to antiplatelet therapy), only 10% were adequately anticoagulated. Some physicians, thinking that antiplatelet therapy is safer than anticoagulation, may consider dual antiplatelet therapy for patients who are reluctant to take warfarin, or in whom it is thought that warfarin is not safe. That approach does not work; Connolly et al reported that adding clopidogrel to aspirin reduced stroke from atrial fibrillation by only 0.67%.19
Probably true contraindication to anticoagulation is less common than many physicians believe. For example, reluctance to prescribe anticoagulation to elderly patients because of fear that the patient may fall is misplaced: anticoagulation is even more beneficial in the elderly than in younger patients,20 and it would take ~295 falls to equal the risk of not taking anticoagulants in atrial fibrillation.21 Most intracerebral haemorrhages can be prevented by effective blood pressure control, and most serious gastrointestinal haemorrhages can be prevented by treating Helicobacter pylori.
Fortunately, with the availability of new DOACs, the decision to anticoagulate for cardioembolic stroke is now much easier. For patients in whom anticoagulation truly seems contraindicated (eg, patients with recurrent intracerebral haemorrhages from amyloid angiopathy), removal or occlusion of the left atrial appendage should be considered. Most thrombi in atrial fibrillation occur in the left atrial appendage.18 The atrial appendage can be removed with closed chest robotic surgery, or occluded with an implant. Left atrial occlusion has become safer in recent years.22
Detection of intermittent atrial fibrillation
Many patients with stroke due to atrial fibrillation have intermittent atrial fibrillation, which may be missed on an ECG or even a Holter recording over 24–48 hours. Gladstone et al 6 studied patients with cryptogenic stroke and a negative Holter recording, who were randomised to either a repeat Holter recording or a 1-month recording with an automated device that detected atrial fibrillation. The repeat Holter detected atrial fibrillation in only 3% of patients, but the longer recording detected it in 16%. Among patients with cryptogenic stroke or TIA with no atrial fibrillation at baseline, a 1-year recording detected atrial fibrillation lasting more than 30 s in 12.4% of patients versus only 2% that were detected in conventional follow-up. Gladstone et al 23 reported that among patients with frequent atrial premature beats, 40% eventually were found to have atrial fibrillation. A question that has not yet been resolved is how much atrial fibrillation justifies anticoagulation. It seems unlikely that a few seconds of atrial fibrillation several times a year would warrant the risk of anticoagulation. On the other hand, intermittent atrial fibrillation tends to progress to persistent atrial fibrillation. This question is an important area for future research.
Paradoxical embolism
In the past, paradoxical embolism was regarded as rare. Because ~25% of the population has a PFO, a high proportion of patients with stroke and a PFO have an incidental PFO (~80%); even among patients with cryptogenic stroke, approximately half of PFOs are incidental.24 It is difficult therefore to determine in a given case if the PFO is incidental or causally related to the stroke.24 Hutchinson and Acheson reported in 1975 (before the widespread availability of echocardiography) that 4% of strokes were attributable to paradoxical embolism.25 In 2008, Ozdemir et al 26 estimated that 5.5% of strokes were attributable to paradoxical embolism, and described a number of clinical clues to the diagnosis. Because paradoxical embolism by definition represents pulmonary embolism, clinical clues include dyspnoea or a Valsalva manoeuvre at the onset of stroke, a history of pulmonary embolism, deep vein thrombosis or varicose veins, a history of prolonged sitting, a history of sleep apnoea (which increases right-left shunting), waking up with stroke or a history of migraine.
The problem of incidental PFO made it difficult to show the benefit of percutaneous closure of PFO, but this problem has finally been settled. Percutaneous closure of PFO is beneficial,27–29 and importantly it is more beneficial compared with antiplatelet therapy than compared with anticoagulation.30 Percutaneous closure of PFO does reduce the risk of stroke; however, selection of patients more likely to benefit is an important issue. Because a paradoxical embolus is a pulmonary embolus, clinical clues to paradoxical embolism include dyspnoea at the onset of stroke, a Valsalva manoeuvre shortly before a stroke, a history of pulmonary embolism, deep vein thrombosis or varicose veins, a history of sleep apnoea (because right-sided pressure is increased during apnoeic episodes) and waking up with stroke (perhaps attributable to sleep apnoea).26 Tobe et al reported that transoesophageal echocardiography (TEE) missed 15% of right-left shunts among patients with PFO detected by transcranial doppler (TCD) saline studies, and of these more than 40% were large shunts (grade III or higher) that predicted a higher risk of recurrent TIA/stroke.7 Figure 2 shows Spencer transcranial Doppler shunt grades in patients with PFO. TCD is more sensitive for detection of PFO than TEE. In part, this is because the bubbles are very obvious, as shown in figure 2, and are accompanied by loud sounds on the speaker of the TCD machine. In addition, sedation during TEE may prevent an adequate Valsalva manoeuvre; anatomical factors that might account for a higher sensitivity of TCD saline studies were discussed by Anzola.31 Larger right-left shunts on TCD were predictive of recurrent stroke.7
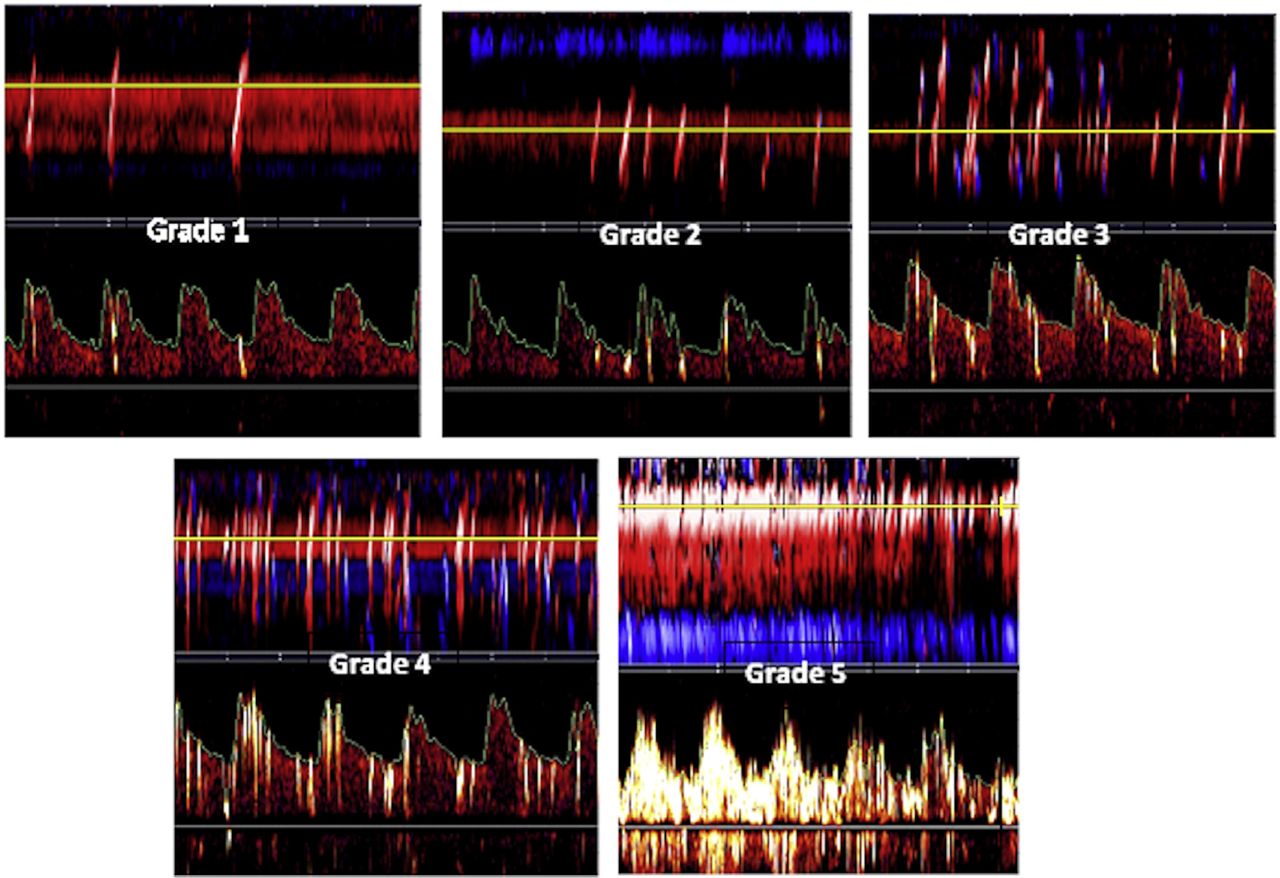
Transcranial Doppler screenshots of Spencer shunt grades are shown for examples of cases missed by transoesophageal echocardiography with sedation. It can be seen that the presence of bubbles in the cerebral arteries is obvious; besides the visual output on the screen, a loud signal is heard from the audio output with each bubble crossing the patent foramen ovale. Grade 0, no microemboli detected; grade 1, 1–10 microemboli; grade 2, 11–30 microemboli; grade 3, 31–100 microemboli; grade 4, 101–300 microemboli; grade 5, >300 microemboli. (Reproduced with permission of Elsevier from Tobe et al 7)
Vitamin B12 deficiency, homocysteine and cardioembolic stroke
High levels of tHcy markedly increase the risk of stroke, particularly among patients with atrial fibrillation. Deficiency of vitamin B12 is much more common than most physicians suppose. This is because a serum total B12 in the reference range does not define the adequacy of functional B12. Only ~6%–20% of serum total B12 is active, so within the ‘normal range’ of serum B12 (~160–600 pmol/L), a large proportion of patients have inadequate metabolically active B12.8 The serum B12 below which plasma levels of tHcy or methylmalonic acid become elevated is ~400 pmol/L.32 33 The combination of a serum B12 in the lower half of the reference range with elevation of plasma methylmalonic acid (or in folate-replete patients, elevated tHcy) is called ‘metabolic B12 deficiency’. Among patients attending my secondary stroke prevention clinics, the prevalence of metabolic B12 deficiency was 10% below age 50, 12% at ages 50–70 and 30% above age 70.34
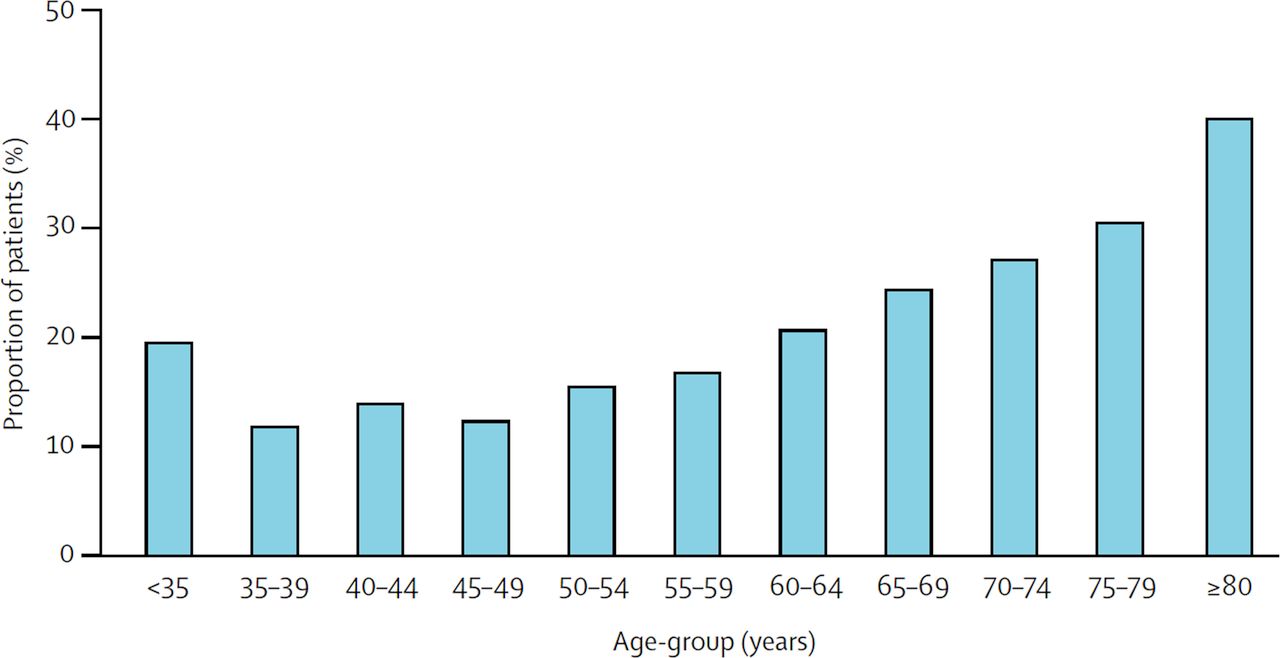
Elevated tHcy quadruples the risk of stroke in atrial fibrillation,35 and above age 80 the most common cause of stroke is atrial fibrillation.36 It is therefore important that among patients with stroke above age 80, more than 40% have an elevated tHcy (figure 3).

Age distribution of increased plasma total homocysteine (≥14 μmol/L) among patients referred to vascular prevention clinics. Among patients attending secondary stroke prevention clinic of JDS at University Hospital in London, Canada, the prevalence of a plasma total homocysteine >14 µmol/L is more than 40% at age 80 and higher: precisely the age group in which atrial fibrillation is the most common cause of stroke. (Reproduced with permission of Elsevier from Spence D. Mechanisms of thrombogenesis in atrial fibrillation. Lancet 2009 Mar 21;373 (9668):1006).
Because metabolic B12 deficiency and elevated tHcy are so common among patients with stroke, all patients with stroke should have their serum B12 and tHcy measured, and appropriately treated.
Treatment with B vitamins to lower levels of tHcy definitely reduces the risk of stroke, but the results of early trials were obscured by harm from cyanocobalamin among patients with impaired renal function.9 (Another article in this issue of the journal provides more detail on this issue.)
Direct oral anticoagulants
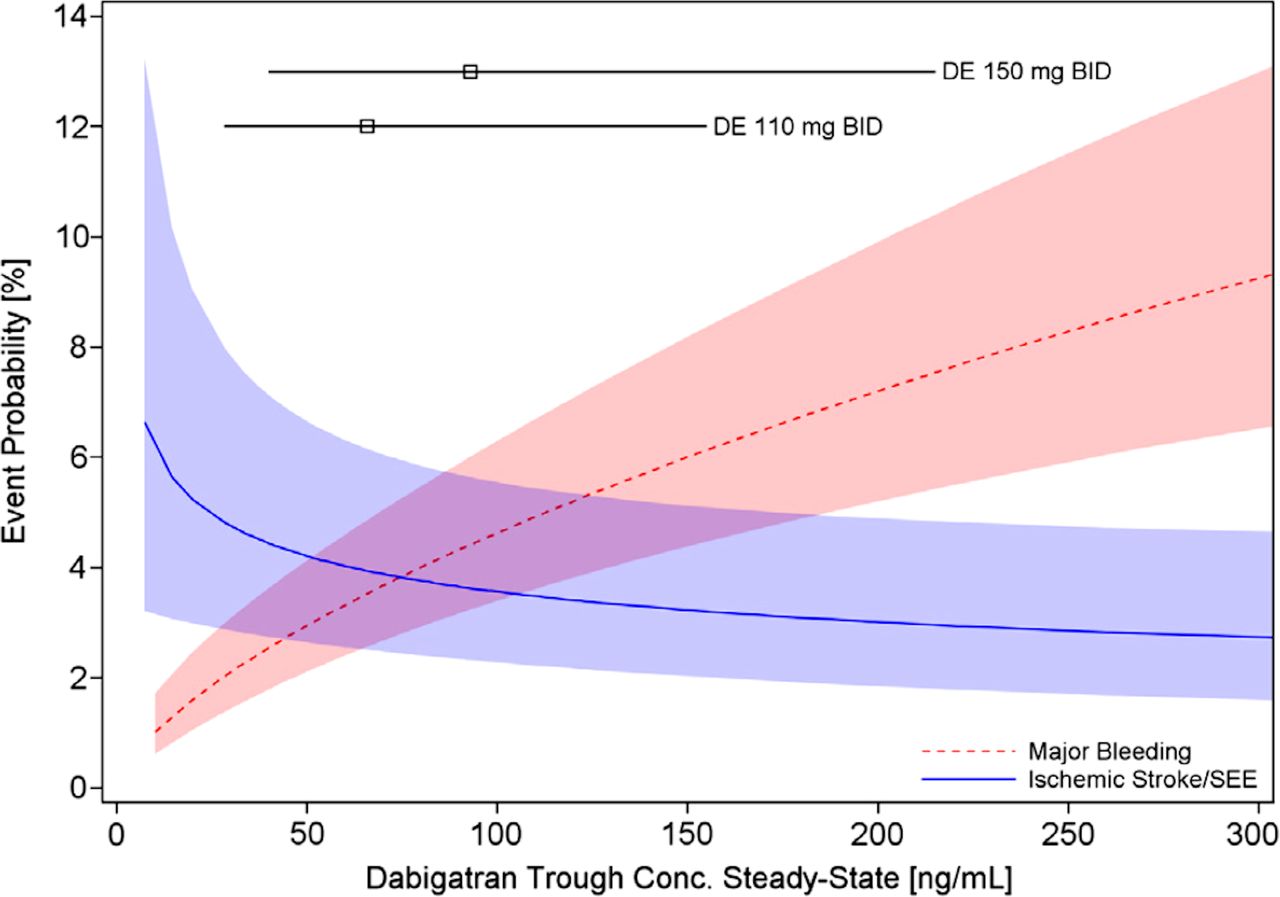
At present, four DOACs are available in North America; their characteristics are shown in table 1. They all are at least as efficacious as warfarin for prevention of stroke in atrial fibrillation, and are safer. Furthermore, for the most part, blood testing is not required as with testing of the international normalised ratio (INR) in patients taking warfarin. A possible exception to this is dabigatran. Dabigatran has the highest proportion of renal elimination of the DOACs. This means that it is problematic in patients with renal impairment, and as renal function declines with age, the elderly, who are the group most likely to have atrial fibrillation, may be at risk of bleeding with dabigatran: among patients with stroke, the average estimated glomerular filtration rate above age 80 is <60 mL/min/1.73 m². Furthermore, dabigatran has the lowest bioavailability at only 6.5%; this means that blood levels will be affected much more by changes in absorption, or by drug interactions. An illustration of this principle is the effect of grapefruit on statin drugs. Plasma levels of atorvastatin (area under the curve, AUC), with a bioavailability of ~50%, are only doubled by grapefruit or grapefruit juice,37 a potent inhibitor of intestinal CYP3A4. In contrast, plasma levels of simvastatin (AUC), with a bioavailability of only 5%, increase 15-fold with grapefruit.38 For these reasons, it may be prudent to measure plasma levels of dabigatran, which has a relatively narrow therapeutic range39 (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probability of major bleeding event and ischaemic stroke/SEE versus trough plasma concentration of dabigatran. Calculated for a 72-year-old male patient with atrial fibrillation with prior stroke and diabetes. Lines and boxes at the top of the panel indicate median dabigatran concentrations in the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) Trial with 10th and 90th percentiles. Conc, one-fourth concentration; DE, one-fourth dabigatran etexilate; SEE, one-fourth systemic embolic event(s). (Reproduced with permission of Elsevier from Reilly et al 39).
Characteristics of direct-acting oral anticoagulants
Another pharmacokinetic consideration may be important. Although rivaroxaban was approved initially for once daily dosing, its half-life is not appreciably longer than that of the other DOACs, which are given twice daily (table 1). It is notable that a recent study with rivaroxaban has used twice daily dosing.40
Perhaps most importantly, it is now clear that DOACs are not significantly more likely than aspirin to cause severe haemorrhage.41 42 This means that the old paradigm is now obsolete. In patients strongly suspected of having cardioembolic stroke, it is no longer safer to use antiplatelet agents than anticoagulants, and since antiplatelet agents are not effective in preventing cardioembolic stroke, it is now more prudent to use DOACs in such patients.4
Warfarin must still be used in some patients: how to minimise risk
In patients with renal failure and those with mechanical prosthetic heart valves it is still necessary to use warfarin. In future, it may be possible to develop safe dosing regimens with DOACs for patients with renal failure; probably apixaban, which is the least dependent on renal elimination, would be a candidate. It is possible that warfarin may be more efficacious in patients with mechanical valves and in a small subgroup of other patients with cardioembolic stroke; warfarin prevents formation of many clotting factors (II, VII, IX and X), in contrast to specific antagonism of selected clotting factors (factor IIa or factor Xa). Atarashi has suggested43 that blockade of factor VII may account for the higher risk of intracranial haemorrhage with warfarin.
Warfarin is difficult to use, and risk of bleeding is high early because of genetic, pharmacokinetic and environmental factors. There are common polymorphisms of both the metabolism of warfarin (CYP2C9) and the sensitivity to a given plasma level of warfarin because of variants of vitamin K epoxide reductase (VORCK1).44 These result in an extremely wide range of dose–response with warfarin; genotyping can improve initial dosing.44 There are many important drug–drug interactions with warfarin.45 Besides drugs that stimulate or inhibit warfarin metabolism via CYP2C9, warfarin is highly protein bound (~95%), so transient increases in INR may be seen when drugs affecting protein binding are added to warfarin therapy. It is impossible to remember all drug interactions, so whenever a new drug is added in a patient taking warfarin, it is necessary to look them up.
Variations in both intake of vitamin K from food, and changes in production of vitamin K by intestinal bacteria also will result in turbulence of the INR. A manoeuvre that may be helpful in reducing INR turbulence is to give a daily small oral dose of vitamin K.46 This would result in requirement for a higher dose of warfarin, but reduce turbulence of the INR.
With the exception of haemorrhages from amyloid angiopathy, virtually all intracerebral haemorrhages can be prevented by effective blood pressure control. In the medical arm of the North American Carotid Endarterectomy Trial, we reduced intracranial haemorrhage (including subarachnoid haemorrhage and haemorrhage from amyloid angiopathy) to 0.5% of strokes by insisting that site physicians increase antihypertensive medication whenever blood pressure was above the targets specified in the protocol.47 (Another article in this issue of the journal addresses control of resistant hypertension.) Most severe gastrointestinal haemorrhages can probably be prevented by diagnosis and treatment of H. pylori.
Conclusion
There is a major problem with underanticoagulation of patients with cardioembolic stroke due historically to difficulties with safe and effective use of warfarin. With the arrival of new oral anticoagulants that are not significantly more likely than aspirin to cause severe haemorrhage, everything has changed. Because antiplatelet agents are much less effective in preventing cardioembolic stroke, it is now more prudent to anticoagulate patients in whom cardioembolic stroke is strongly suspected. There are many important considerations in the judicious use of anticoagulation and other therapies for prevention of stroke.
References
Footnotes
Contributors JDS wrote the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JDS was a site investigator for the CLOSURE, RESPECT and REDUCE trials of percutaneous closure of patent foramen ovale, and received consulting or lecture fees from Bayer, Bristol-Myers Squibb and Pfizer relating to anticoagulation. JDS has also participated in studies of aspirin, clopidogrel and ticagrelor in the past.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Guest chief editor J David Spence