Article Text

Abstract
Background and purpose Clinical features of epileptic seizures after cerebral venous sinus thrombosis (CVST) among Chinese patients are not known, and it is still controversial whether seizures would affect the outcome of CVST.
Methods In a Chinese hospital-based study of consecutive patients with CVST between 2003 and 2015, we described the clinical features of seizures and determined the predictors of seizure onset using multivariable logistic regression analysis. We also compared the in-hospital case-fatality and short-term functional outcome (modified Rankin Scale (mRS) at discharge) in patients with versus without seizures using ordinal regression analysis.
Results Among 151 patients with CVST, 52 (34.4%) presented seizures, of which 42 (80.8%) were generalised seizures. Male gender (OR 6.32, 95% CI 2.06 to 19.35, p=0.001), motor deficits (OR 4.89, 95% CI 1.52 to 15.68, p=0.008), intracerebral haemorrhage (OR 3.93, 95% CI 1.16 to 13.26, p=0.027), cerebral infarction (OR 3.78, 95% CI 1.15 to 12.36, p=0.029) and superior sagittal sinus thrombosis (OR 3.38, 95% CI 91.16 to 9.86, p=0.026) were independent predictors for seizures. The overall in-hospital case-fatality rate was 2.0% (3/151), and 21 (13.9%) had mRS >2 at discharge. Compared with patients without seizures, patients with seizures were more likely to have a worse outcome (p=0.02) at discharge, independent of age, gender, clinical presentation, clot burden and presence of parenchymal lesions.
Conclusions In Chinese Han patients, compared with patients without seizures, patients with seizures after CVST had a worse outcome. Risk factors such as male gender, paresis, parenchymal lesion and superior sagittal sinus thrombosis were independently associated with seizure onset after CVST. Generalised seizure was the main form of seizures after CVST, which was obviously different to seizures after strokes of arterial origin.
- cerebral vein thrombosis
- epileptic seizures
- risk factors
- prognosis
- logistic regression analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Cerebral venous sinus thrombosis (CVST) is a rare type of cerebrovascular disease, affecting approximately 13.2 people per million annually.1 Although CVST accounts for only 0.5%–1% of all strokes in all age groups,2 it is one of the diseases affecting mainly young patients.3 It has been shown that approximately 40% patients with CVST would experience epileptic seizures during the acute phase,4 and 9% patients had residual active epilepsy after 39 months follow-up.4 However, the detailed clinical features of these seizures were less well studied and clinical predictors for seizure onset after CVST are unclear. Although the clinical outcome after CVST has been reported in the Caucasian population,5 data on the outcome in the Chinese Han population are scarce, and there is still conflicting evidence whether seizure onset is associated with poor outcome in patients with CVST.6–9 Therefore, in a Chinese Han population, we aimed to determine the clinical features and predictors of seizure onset in patients with CVST, and to compare the clinical outcome in patients with versus without seizures.
Methods
The records of all consecutive patients with CVST treated at Huashan Hospital, Shanghai between January 2003 and June 2015 were reviewed. Patient demographics, past medical history, clinical features, seizure type, laboratory tests, neuroradiological findings and presence and type of parenchymal lesions (ie, haemorrhage vs venous infarct), and the modified Rankin Score (mRS) at discharge were carefully recorded. Diagnosis of CVST and seizure was based on the criteria of guidelines.3 9–11 All patients had CVST confirmed by magnetic resonance (MR)/MR venography or digital subtraction angiography. Early seizure after CVST was defined as seizures that occurred within 2 weeks from symptom onset (including epileptic attack as the first symptom), in accordance with the definition used in the VENOPORT study.7 The sinus clot burden was quantified by a CVST scoring system, assigning 1 point for each sinus; the superior sagittal sinus (SSS) was divided into thirds with 1 point assigned for each third. Occlusion of each internal cerebral vein and the vein of Galen was assigned 1 point, respectively.12
The study was approved by the Institutional Review Board of Huashan Hospital (KY2015176).
Descriptive statistics were performed to analyse the patients with CVST with and without seizures. For continuous variables, means, SD, medians and ranges were calculated. For categorical variables, numbers and percentages for each category were tabulated.
We compared the demographics, past medical history, clinical features, neuroradiological findings and the CVST score in patients with versus without seizures using student’s t-test for continuous variable and χ2 test/Fisher’s exact test for categorical variables. All variables associated with seizures were then entered into a logistic-regression analysis backward model and ORs with 95% CIs were calculated. We compared the mRS at discharge between patients with versus without seizures using the ordinal regression analysis, adjusting for prognostic factors suggested in other studies: age, gender, clinical presentation (clinical symptoms, consciousness and mental disorders), CVST score and presence of parenchymal lesions.5 13 14 We also compared the possible effect of antiepileptic drug use (AED) on mRS at discharge stratified by seizure status using χ2 test.
A significant difference was set at p<0.05. All analyses were conducted with SPSS V.13.0 for Windows.
Results
Baseline characteristics
One hundred and fifty-one patients (64.9% male) were included in the study, with a median age of 37 years (IQR, 26–45 years). One hundred and twenty-four (82.1%) patients were younger than 50 years. Patients were divided into two groups: (1) patients with seizures (n=52, 34.4%) and (2) patients without seizures (n=99, 65.6%). Baseline characteristics of these two groups are listed in table 1.
Baseline characters of patients with and without seizures
Among the 52 patients who had seizures, the median time from CVST onset to seizure presentation was 3.5 days (IQR 0–10). Fifteen (28.8%) patients presented with seizures as the first symptom. Thirty-nine (75%) patients had early seizures within 2 weeks from CVST onset, 43 (82.7%) had seizures within 3 weeks. As for seizure type, 7 (13.5%) patients had only focal seizures, 6 (11.5%) experienced focal seizures and secondary generalised seizures, 36 (69.2%) suffered generalised seizures and status epilepticus was observed in 3 (5.8%) patients.
Risk factors associated with seizures
As shown in table 1, patients with seizures were more likely to be male, more often presented with confusion, headache or motor deficits, and more frequently had parenchymal lesions on brain imaging, especially for intracerebral haemorrhage. Older age (>37 years) and infectious cause, however, were less frequently observed in patients with seizures.
In a multivariable analysis (table 2), male gender (OR 6.32, 95% CI 2.06 to 19.35, p=0.001), motor deficits (OR 4.89, 95% CI 1.52 to 15.68, p=0.008), intracerebral haemorrhage on brain imaging (OR 3.93, 95% CI 1.16 to 13.26, p=0.027), infarct on brain imaging (OR 3.78, 95% CI 1.15 to 12.36, p=0.029), SSS thrombosis (OR 3.38, 95% CI 1.16 to 9.86, p=0.026) were independently associated with seizures after CVST, while older age (>37 years) (OR 0.16, 95% CI 0.06 to 0.48, p=0.001), strait sinus thrombosis (OR 0.07, 95% CI 0.01 to 0.32, p=0.001), infectious cause (OR 0.12, 95% CI 0.03 to 0.52, p=0.005) and hematonosis or malignancy (OR 0.19, 95% CI 0.05 to 0.74, p=0.017) were negatively associated with seizures.
Multivariable analyses of risk factors associated with seizures
Outcome of seizures and the effect of AEDs
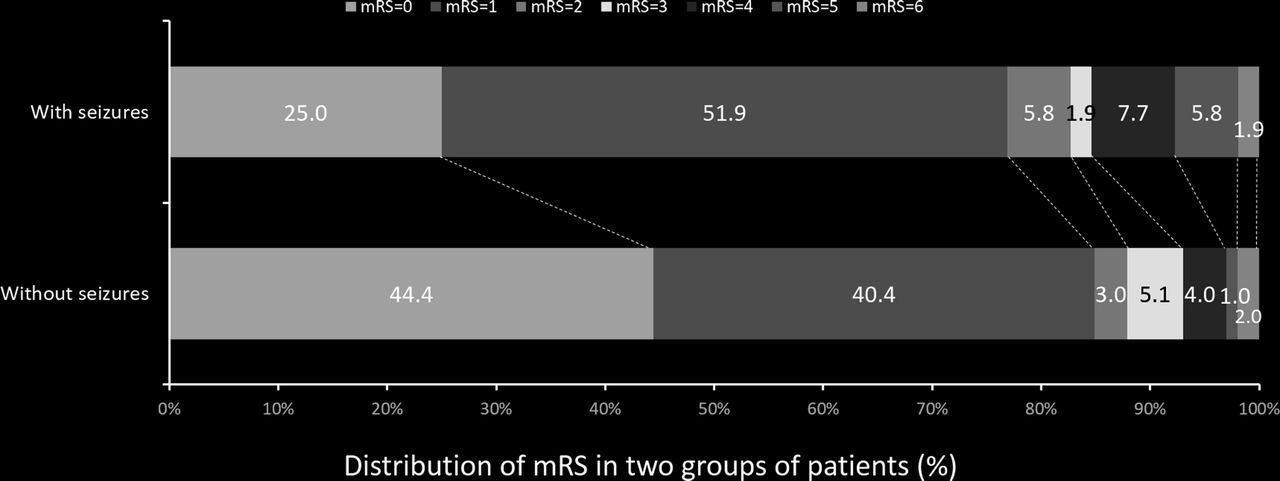
The average time for hospitalisation was 22±15 days, with no difference in patients with versus without seizures (23 days with seizures vs 22 days without seizures, p=0.62). Two (1.3%) patients died due to transtentorial herniation and one (0.6%) had sudden death presumably due to pulmonary embolism. Compared with patients without seizures, patients with seizures were more likely to have a worse clinical outcome (p=0.02, figure 1). The trend remained consistent after adjusting for age, gender, clinical presentation, CVST score and presence of parenchymal lesions (p=0.047).
{kind=link}
Compared modified Rankin Scale (mRS) at discharge between patients with and without seizures.
AEDs were prescribed to 38 patients, 33 (63.5%) with seizures, 5 (5%) without seizures. Fourteen (26.9%) patients with seizures used two or more type of AEDs. Seizure was controlled in most patients at the time of discharge except for one patient (1.9%) who suffered malignant tumour. Clinical outcome did not differ significantly between patients treated with AEDs versus those not treated with AEDs both for patients with seizures and those without seizures (with seizures p=0.55, without seizures p=1.00, table 3).
AEDs did not change the outcome at discharge
Discussion
In this hospital-based study of Chinese patients with CVST, we showed generalised seizure was the main form of seizures after CVST, and male gender, motor deficits, parenchymal lesions or SSS thrombosis were independent predictors of seizure onset. Although the overall in-hospital case-fatality was low, patients with seizures after CVST had a worse outcome.
In our study, we found that 82.1% cases were younger than 50 years and the median age (37 years) was similar as reported by the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT, median age 37 years)6 and the VENOPORT studies (median age 38 years),7 which confirmed that CVST mainly affects young patients both in the East and West.
We found that 34.4% of the patients with CVST had epileptic seizures, which was in accordance with most previous studies (nearly 40%).6 14 However, few previous studies reported the details about the subtypes of seizures. The VENOPORT study only reported the subtypes of seizures in eight patients.7 We found that seizures were focal in 13.5% patients, generalised in 69.2% and 11.5% of the patients experienced both types. Therefore, it appeared that generalised seizure was the main form of seizures (80.7%) after CVST, which was obviously different to seizures after strokes of arterial origin, which were predominantly partial seizures.15
Although the majority of the patients with seizures had good seizure control at discharge in our study, we showed that the discharge mRS was significantly different between the two groups, with the group with seizures doing much worse, indicating that seizures might worsen patients’ neurological function, at least in the short-term. This is supported by the ISCVT cohort, which showed that seizure onset was an independent predictor of death within 30 days after symptom onset.16 Some studies also illustrated that seizures could cause neurological and systemic deterioration, status epilepticus and death.7 16–18 Interestingly, the in-hospital case-fatality was 2% in our study, which was lower than reported both in ISCVT (4.3% at discharge) and in another large national sample (4.4%),19 suggesting that the outcome might be better in Chinese than Caucasian population.
Similar to previous studies, we also found that male gender, motor deficits, intracerebral haemorrhage, infarct and SSS thrombosis were independently associated with seizures,5 7 17 possibly relating to the injury that involved the cortical layer. However, in addition to the known risk factors, we also had some interesting findings. We found that older age, straight sinus thrombosis and causes such as infection, hematonosis or malignancies were negatively associated with seizures. We speculated that the possible reason for the lower risk of seizures in older patients could be related to the decreasing excitability of the cortex with ageing. Straight sinus thrombosis mainly affects the bilateral thalamus, and the acute damage may result in the blockage of outer information to the cortex, while less likely to affect the risk of seizures. None of the seven patients with CVST with involvement of the deep venous system had seizures in the VENOPORT study also supported our findings.7
The most difference between our study and the others was the sex ratio. Male patients were much more frequent (women:men=1:1.85) in our study, whereas female patients were more frequently seen (women:men=3:1) in other studies.20 We think there are three possible reasons. First, this could be due to an inclusion bias towards more complex CVST cases in this single academic centre hospital-based study. It was easy to identify female patients with gender-specific risk factors, but male patients were more difficult to diagnose. So those cases that defied diagnosis were transferred to our hospital. Second, Chinese Han female rarely take oral contraceptive pills, which is one of the main causes of CVST in women in the ISCVT study and some other series. Third, there might be some genuine ethnic difference between the East and the West. A research from Tiantan Hospital and Xuanwu Hospital in China had also suggested that male patients were more than female (women: men=1:1.3).21 Chinese largest case series about CVST (163 patients) showed that women: men=1:0.91.22 Those results indicated that the sex ratio of CVST in China is different from that of the European and American groups.
The strength of the study lies in that it is of moderate sample size and was nested in a Chinese Han population. Moreover, all cases included were newly diagnosed with detailed clinical information. Furthermore, we used central and single-blinded imaging assessment to reduce the inducement bias. However, there are also some limitations. First, cases were not free from selection bias because it was a single-centre study. The lack of female patients with oral contraceptive or pregnancy/puerperium could lead to the Berkson’s bias. Second, not all patients had electroencephalogram recordings to identify all subclinical epilepsy. Therefore, we could not assess the role of prophylactic AEDs in these patients. Limited to the imaging technique, we did not study lone cortical veins thrombosis, which was another suggested predictor of seizures onset.
In conclusion, seizures after CVST was associated with worse outcome at discharge. Given that male gender, motor deficits, parenchymal lesions or SSS thrombosis were independently associated with seizures after CVST, they could be potentially used as a selection criteria for prophylactic AEDs use in patients with CVST. Prospective cohort studies are needed to confirm these findings.
References
Footnotes
Contributors HD contributed to study design, literature search, data collection, data analysis, data interpretation and manuscript preparation. YX contributed to study design, literature search, data collection, data analysis, data interpretation and manuscript preparation. LL contributed to data analysis and data interpretation. HC contributed to data collection and data analysis. YT contributed to data collection and data analysis. QD contributed to study design, data interpretation and manuscript preparation. MC contributed to study design, data interpretation and manuscript preparation.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Institutional Review Board of Huashan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data of our study is under analysing and prepared for another submission. Thus, it is not available now. If any researcher has questions, they can contact with the first author HD (hyding2001@163.com).