Article Text

Abstract
Introduction ABCD2 risk score and cerebral microemboli detected by transcranial Doppler (TCD) have been separately shown to the predict risk of recurrent acute stroke. We studied whether ABCD2 risk score predicts cerebral microemboli in patients with hyper-acute symptomatic carotid artery stenosis.
Participants and methods We studied 206 patients presenting within 2 weeks of transient ischaemic attack or minor stroke and found to have critical carotid artery stenosis (≥50%). 86 patients (age 70±1 (SEM: years), 58 men, 83 Caucasian) had evidence of microemboli; 72 (84%) of these underwent carotid endarterectomy (CEA). 120 patients (age 72±1 years, 91 men, 113 Caucasian) did not have microemboli detected; 102 (85%) of these underwent CEA. Data were analysed using X 2 and Mann–Whitney U tests and receiver operating characteristic (ROC) curves.
Results 140/206 (68%: 95% CI 61.63 to 74.37) patients with hyper-acute symptomatic critical carotid stenosis had an ABCD2 risk score ≥4. There was no significant difference in the NICE red flag criterion for early assessment (ABCD2 risk score ≥4) for patients with cerebral microemboli versus those without microemboli (59/86 vs 81/120 patients: OR 1.05 ABCD2 risk score ≥4 (95% CI 0.58 to 1.90, p=0.867)). The ABCD2 risk score was <4 in 27 of 86 (31%: 95% CI 21 to 41) embolising patients and in 39 of 120 (31%: 95% CI 23 to 39) without cerebral microemboli. After adjusting for pre-neurological event antiplatelet treatment (APT), area under the curve (AUC) of ROC for ABCD2 risk score showed no prediction of cerebral microemboli (no pre-event APT, n=57: AUC 0.45 (95% CI 0.29 to 0.60, p=0.531); pre-event APT, n=147: AUC 0.51 (95% CI 0.42 to 0.60, p=0.804)).
Conclusions The ABCD2 score did not predict the presence of cerebral microemboli or carotid disease in over one-quarter of patients with symptomatic critical carotid artery stenosis. On the basis of NICE guidelines (refer early if ABCD2 ≥4), assessment of high stroke risk based on ABCD2 scoring may lead to inappropriate delay in urgent treatment in many patients.
- Platelets
- Stroke
- microemboli
- transcranial doppler
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The risk of recurrent stroke following first transient ischaemic attack (TIA) or minor stroke is highest during the first 7–14 days.1 On the basis of evidence that the benefit of surgery is greatest if performed within 2 weeks after the last ischaemic event,2 the major NICE clinical guideline recommends that patients with symptomatic carotid artery stenosis have urgent endarterectomy within 2 weeks.3
Transcranial Doppler (TCD)-detected microemboli have provided direct evidence of thromboembolism as the main mechanism of symptomatic carotid artery disease.4 TCD-detected cerebral microembolic signals (MES) predict short-term stroke risk in patients with symptomatic carotid stenosis.5–9
The ABCD2 risk prognostic scoring system10 predicts who is likely to be at increased risk of suffering a recurrent early stroke following onset of an initial stroke/TIA,10 irrespective of the mechanism for acute stroke or TIA. The ABCD2 risk score is based on standard cardiovascular risk factors, including history of diabetes, in addition to clinical features of carotid disease. Several major clinical guidelines3 ,11 recommend that patients with an ABCD2 risk score ≥4 should be assessed within 24 hours and those with an ABCD2 risk score <4 should be evaluated within a week of symptoms onset.
ABCD2 risk score and the presence of cerebral microemboli predict risk of early recurrence of stroke. The association between ABCD2 risk score and cerebral microemboli has not been studied. We therefore aimed to explore whether the ABCD2 risk score predicts the presence of cerebral microemboli in patients with hyper-acute symptomatic critical carotid artery stenosis.
Participants and methods
We determined ABCD2 scores in 206 patients (age 70±1 (SEM) years, men 149, Caucasian 196) with acutely symptomatic critical carotid artery stenosis. A total of 102 patients were from our Carotid Registry of patients who had undergone carotid endarterectomy (CEA) between January 2002 and December 2010.12 A further 104 consecutive patients were recruited between January 2011 and May 2013 within a new prospective observational study of patients presenting with acutely symptomatic critical carotid artery stenosis. In this report, we define the hyper-acute period as within 2 weeks of stroke or TIA.13
Inclusion and exclusion criteria
All patients had presented within 2 weeks of symptoms of acute non-disabling stroke (Modified Rankin Scale (mRS) ≤2) or TIA. All had haemodynamically significant carotid artery stenosis of at least 50%14 measured by carotid duplex scan based on NASCET criteria as recommended by Vascular Society and the Society of Vascular Technology of Great Britain and Ireland.15 Since 2002, it has been the policy in our centre for all patients with hyper-acute symptomatic TIA or stroke to have a TCD examination to detect cerebral microemboli, as this cohort of patients merits more aggressive treatment to prevent recurrent stroke.16
We excluded patients with atrial fibrillation, because this confers risk of an additional non-carotid source of emboli. We also excluded patients with a prosthetic heart valve, because of the recognised effect of these valves to generate gaseous and other embolic signals.17 We also excluded patients who had had a major stroke or presented more than 2 weeks after the onset of symptoms.
Assessment of the ABCD2 risk score
ABCD2 scores9 were available in all patients recruited for the prospective observational study from 2011 to 2013. Seven patients from the Carotid Surgery Registry from the period of 2002 and 2005 were excluded from the analysis due to lack of data pertinent to the ABCD2 risk score calculation.
TCD recording
TCD monitoring18 was performed (PC Dop 842; SciMed, Bristol, UK) with a 2 MHz probe focused on the middle cerebral artery ipsilateral to the stenotic carotid artery. The TCD signal was assessed by an experienced vascular scientist. The middle cerebral artery (MCA) was identified by placing the probe above the zygomatic arch and just in front of the ear. A head-frame was used to secure a constant angle of insonation during the TCD monitoring. Doppler signals were obtained within the depth range of 55–64 mm and time-averaged mean velocity in the region of 55±12 cm/s. We used a single channel and a filter set to a low threshold to capture all possible signals. The recorded ultrasonographic images were then assessed to differentiate artefact from microemboli, based on criteria of the International Consensus Group on microembolus detection.18 MES were identified as unidirectional, short duration signals (range 10–100 ms) with intensity threshold above 6 dB, accompanied by characteristic audible clicks and occurring randomly throughout the cardiac cycle.18 ,19 Monitoring was performed for 60 min after carotid duplex assessment.
Microembolic signals
On the basis of Markus et al,7 we used a dichotomous outcome to classify patients with microembolic TIA or stroke, according to MES presence rather than rate or number of MES.
Ethics
The new prospective observational study was approved by the NHS Ethics Committee (MREC number 10/H1206/77) and Research & Development Department (R&D C1080610). All patients included in the new prospective observational study were consented. For the Registry data, institutional approval was granted; the Research & Development Department at University Hospital Coventry and Warwickshire NHS Trust (host institution) confirmed that regional Research Ethics Committee (REC) review was not required under the harmonised Governance Arrangement for REC (GAfREC) for research because this study was considered part of service evaluation (audit). Therefore, patients’ consent was not required.
Statistical analyses
In view of differences among patients in antiplatelet treatment (APT) prior to their acute neurological events, we analysed the data in two stages. Initially, we studied microembolic and non-microembolic cohorts together. Then, taking into account the influence of APT on cerebral microemboli,20 we analysed the data separately for patients with or without pre-neurological event antiplatelet or statin treatment.
Statistical analyses were conducted using SPSS V.19 (Chicago, Illinois, USA).
Parametric data are expressed as mean and SEM. Non-parametric data are expressed as median and IQR. Non-parametric unpaired data were analysed using the Mann–Whitney U test for two group comparisons. Categorical variables were analysed using the χ2 test or Fisher's exact test. Spearman's rank correlation coefficient was used to assess the strength of relationship between microemboli and ABCD2 risk score. The association between microemboli and ABCD2 risk scores was also analysed using receiver operating characteristic (ROC) curves. A p value of <0.05 was considered significant.
Sample size calculation
We set an area under the curve (AUC) of 0.5 or below as the cut-off point for ABCD2 score not predicting the presence of microemboli. For the whole group, the study had 80% power at the 5% level in a two-tailed test to detect at least 0.69 as AUC for ROC (71 participants per group).
Results
Clinical features
We included 206 patients (age 70±1 year, 149 men, 196 Caucasians) in this study. A total of 86 patients (age 70±1, 58 men, 83 Caucasians) had evidence of microemboli; 72 (84%) of these underwent CEA. A single patient had a TIA, one patient developed myocardial infarction and one embolising patient died due to renal failure 30 days after CEA.
A total of 120 patients (age 72±1 years, 91 men, 113 Caucasians) did not have microemboli detected; 102 (85%) of these underwent CEA. APT had been prescribed to 67 of 86 (78%) patients with microemboli, and to 82 of 120 (68%) patients without microemboli (p=0.130, X 2) prior to the index neurological event. The complications in the 30 days after CEA were TIA in two patients, stroke in three patients and death in three non-embolising patients (sepsis and haemorrhagic strokes).
Family history of vascular disease was more common in the non-embolising group (42 (35%)) than in those who had microemboli following non-disabling stroke/TIA (19(22%); OR 1.5 (95% CI 0.98 to 2.2); p=0.045, table 1). Peripheral arterial disease was also more common in the non-embolising group (21(18%)) compared with those who had microemboli associated with stroke or TIA (7(8%); OR 1.8 (95% CI 0.95 to 3.6), p=0.038, tables 1 and 2). The microembolic stroke/TIA cohort had a slightly higher level of total cholesterol (4.9±0.2 mmol/L) than controls (4.5±0.1 mmol/L; p=0.01, MW; table 2). Carotid ultrasound imaging revealed no difference in degree of carotid artery stenosis between those with versus those without microemboli (microemboli: 80±1% vs controls: 79±1%; p=0.845, MW test).
Demographic and clinical profile in patients with hyper-acute symptomatic carotid stenosis: 120 without microemboli and 86 with microemboli
Blood pressure and preoperative laboratory values in patients with hyper-acute symptomatic carotid stenosis: 120 without microemboli and 86 with microemboli
ABCD2 risk score
Of 206 patients 140 (68%: 95% CI 62% to 74%) patients with hyper-acute symptomatic critical carotid stenosis had an ABCD2 risk score ≥4. The ABCD2 risk score was ≥4 in 59 of 86 (69%: 95% CI 59% to 79%) embolising patients and in 81 of 120 (68%: 95% CI 60 to 76) without cerebral microemboli. There was no significant difference in the NICE criterion for early assessment (ABCD2 risk score ≥4) for patients with cerebral microemboli versus those without microemboli (59/86 vs 81/120 patients: OR 1.05 (95% CI 0.58 to 1.90, p=0.867)).
Of 206 patients, 66 (32%: 95% CI 26 to 38) patients with hyper-acute symptomatic critical carotid stenosis had an ABCD2 risk score <4. The ABCD2 risk score was <4 in 27 of 86 (31%: 95% CI 21 to 41) embolising patients and in 39 of 120 (31%: 95% CI 23 to 39) without cerebral microemboli.
There was no significant ABCD2 score difference between these two cohorts (non-embolising group, n=120: ABCD2 score 4 (IQR 3–5) versus embolising group, n=86: 4 (IQR 3–5), p=0.855 MW test). There was no significant ABCD2 score difference between Registry patients and prospective cohort study patients (Registry, n=102: ABCD2 score 4(IQR 3–5) versus prospective cohort study, n=104: 4(IQR 3–5), p=0.661 MW test).
ROC for ABCD2 score to predict the presence of microemboli
All 206 patients were included into this analysis: 120 patients without and 86 patients with microemboli. The ROC for ABCD2 risk scores showed no significant prediction of microemboli (AUC 0.49, 95% CI 0.41 to 0.57, p=0.860; figure 1).

ROC for ABCD2 risk scores against the presence of microemboli in patients (n=206) with hyper-acute symptomatic carotid stenosis (AUC 0.49, 95% CI 0.41 to 0.57, p=0.860). AUC, area under the curve; ROC, receiver operating characteristic.
Patients without APT before the neurological event
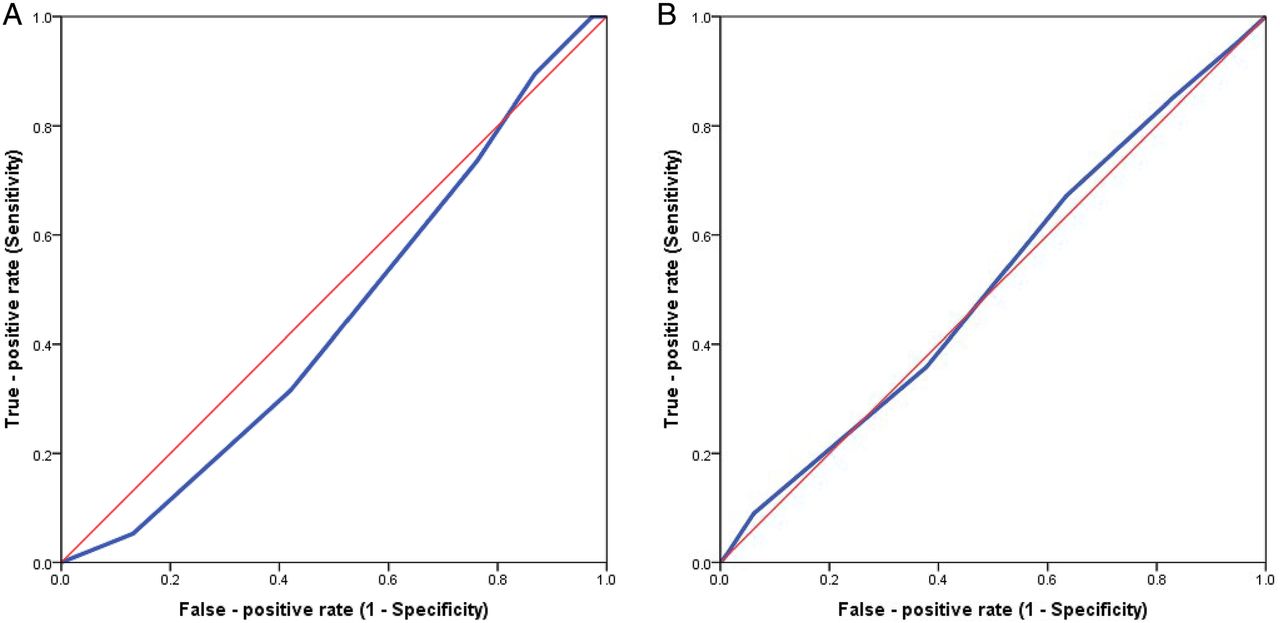
A total of 57 patients were included in this analysis, 19 of whom had evidence of microemboli and 38 patients no evidence of microemboli. The ROC for ABCD2 risk score showed no prediction of microemboli (AUC 0.45 (95% CI 0.30 to 0.60), p=0.531; figure 2A).
{kind=link}
{kind=link}
(A) ROC for ABCD2 risk scores against the presence of microemboli in patients (n=57) without APT pre-neurological event (AUC 0.45 (95% CI 0.30 to 0.60), p=0.531). (B) ROC for ABCD2 risk scores against the presence of microemboli in patients (n=149) with APT pre-neurological event (AUC 0.51 (95% CI 0.43 to 0.60), p=0.531). APT, antiplatelet treatment; AUC, area under the curve; ROC, receiver operating characteristic.
Patient with APT before the neurological event
A total of 149 patients were included in this analysis, 67 of whom had evidence of microemboli and 82 patients had no evidence of microemboli. The ROC for ABCD2 risk score showed no prediction of microemboli (AUC 0.51 (95% CI 0.42 to 0.60), p=0.804: figure 2B).
Patients without statin treatment before the neurological event
A total of 72 patients were included in this analysis, 31 of whom had evidence of microemboli and 41 had no evidence of microemboli. The ROC for ABCD2 risk score showed no prediction of microemboli (AUC 0.48 (95% CI 0.34 to 0.61), p=0.716).
Patient with statin treatment before the neurological event
A total of 134 patients were included in this analysis, 55 of whom had evidence of microemboli and 79 patients had no evidence of microemboli. The ROC for ABCD2 risk score showed no prediction of microemboli (AUC 0.50 (95% CI 0.40 to 0.60), p=0.980).
Discussion
In our study, the ABCD2 risk score was unable to identify patients with cerebral microemboli associated with symptomatic critical carotid artery stenosis. To the best of our knowledge, this is the first report to explore the possible links between ABCD2 risk score and cerebral microemboli in patients with hyper-acute symptomatic critical carotid artery stenosis. Taken together with previous reports,5–9 our study provides important evidence that the occurrence of cerebral microemboli, predictors of stroke risk, is dissociated from the results for the ABCD2 risk score.
In our study, around one-third of the patients with hyper-acute symptomatic carotid disease with or without microemboli would not have been triaged effectively for urgent management using the ABCD2 risk score alone. Furthermore, almost a third of the patients with microemboli with ABCD2 risk score <4 would not have been assessed within 24 hours if NICE guidelines had been followed.
Of note in our study, vascular complications were lower in patients with MES. This is likely to be due to reverse causality, as in our centre patients with microemboli were assigned to receive more aggressive APT compared to those in whom microemboli were not detected.16 ,21
Currently, the association between ABCD2 risk score and severity of structural carotid artery disease is unclear. This is an important issue to clarify as Ois et al 22 reported that patients presenting with symptomatic critical carotid artery stenosis incur a 17% risk of recurrent stroke at 72 hours, increasing to 22% at 7 days.22 While Amarenco et al 23 and Walker et al 24 did not find an association between ABCD2 risk score and carotid artery disease, Schrock et al,25 Sheehan et al 26 and Koton and Rothwell27 suggested that high ABCD2 risk score may identify patients with significant carotid artery disease. However, Amarenco et al 23 reported that an ABCD2 risk score < 4 would miss 9% (62/679) of patients with symptomatic critical carotid artery stenosis.
The inadequacy of ABCD2 risk score alone for stratification of high risk of a recurrent event after a stroke or TIA has been recognised by Merwick et al 28 in an international multicentre observational study based on pooled data from Europe and North America. Merwick et al 28 expanded the standard ABCD2 risk score to the ABCD3-I risk score by including the presence of ≥2 TIA within 7 days, critical carotid artery stenosis and acute diffusion-weighted imaging hyperintensity lesion. ABCD3-I risk scores were found to be better at stratifying stroke risk than ABCD2 risk score in patients who had stroke/TIA. In a more recent validation study in Japan, the ABCD3-I risk score was found to be better at stratifying stroke risk than ABCD2 risk score in patients who had stroke or TIA.29 This finding should be expected as patients with recent symptomatic carotid stenosis and diffusion-weighted imaging were at least threefold higher risk of stroke.28 However, diffusion-weighted imaging and carotid imaging are only available at the secondary care level, so this defeats the initial purpose of applying the ABCD2 risk score for triage in the community. With additional carotid stenosis in the risk score means that the carotid imaging should generally be performed in all TIA/minor ischaemic patients who had stroke as soon as possible. This is potentially problematic in clinical settings with limited access to carotid imaging (whether the patient is admitted or not). Another limitation of studies by Merwick et al 28 and Kiyohara et al 29 was that only 12% and 20% of patients, respectively, had carotid disease in their studies.
Our study has major policy implications. In particular, we have shown that the ABCD2 risk score, a widely used and relied on score to guide stroke management, is seriously flawed in failing to detect many patients who had high-risk carotid disease with or without microemboli. The presence of microemboli is already a well-established predictor of stroke,6 and treatment to suppress microemboli has been shown to reduce the rate of recurrent stroke.20 It would therefore not have been ethical to deprive patients identified as having microemboli from early active treatment.
Conclusions
Thus, on the basis of ABCD2 risk score alone, a significant minority of patients with hyper-acute symptomatic carotid stenosis with or without cerebral microemboli would be likely to be overlooked in triage for more urgent assessment and thus exposed to delays in treatment to preventable recurrent stroke.
References
Footnotes
CEH and CHEI are joint senior authors.
Contributors MS and DRJS conceived the study. All authors were responsible for the design and execution of the study. MS was responsible for data collection and data analysis. DRJS, CEH and CHEI are guarantors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The prospective observational study was approved by the NHS Ethics Committee (MREC number 10/H1206/77) and Research & Development Department (R&D C1080610).
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.