Article Text

Abstract
Background The number of mobile stroke programmes has increased with evidence, showing they expedite intravenous thrombolysis. Outstanding questions include whether time savings extend to patients eligible for endovascular therapy and impact clinical outcomes.
Objective Our mobile stroke unit (MSU), based at an academic medical centre in upstate New York, launched in October 2018. We reviewed prospective observational data sets over 26 months to identify MSU and non-MSU emergency medical service (EMS) patients who underwent intravenous thrombolysis or endovascular thrombectomy for comparison of angiographic and clinical outcomes.
Results Over 568 days in service, the MSU was dispatched 1489 times (2.6/day) and transported 300 patients (20% of dispatches). Intravenous tissue plasminogen activator (tPA) was administered to 57 MSU patients and the average time from 911 call-to-tPA was 42.5 min (±9.2), while EMS transported 73 patients who received tPA at 99.4 min (±35.7) (p<0.001). Seven MSU patients (12%) received tPA from 3.5 hours to 4.5 hours since last known well and would likely have been outside the window with EMS care. Endovascular thrombectomy was performed on 21 MSU patients with an average 911 call-to-groin puncture time of 99.9 min (±18.1), while EMS transported 54 patients who underwent endovascular thrombectomy (ET) at 133.0 min (±37.0) (p=0.0002). There was no difference between MSU and traditional EMS in modified Rankin score at 90-day clinic follow-up for patients undergoing intravenous thrombolysis or endovascular thrombectomy, whether assessed as a dichotomous or ordinal variable.
Conclusions Mobile stroke care expedited both intravenous thrombolysis and endovascular thrombectomy. There is an ongoing need to show improved functional outcomes with MSU care.
- thrombolytic therapy
- thrombectomy
- stroke
Data availability statement
Data are available upon reasonable request. Deidentified participant data are available upon reasonable request to matthew_bender@urmc.rochester.edu.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Fassbender et al introduced the concept of a mobile stroke unit (MSU) in 2003, the essential components of which remain standard ambulance equipment, a CT scanner, point-of-care laboratory equipment, telemedicine capabilities and the ability to administer tissue plasminogen activator (tPA).1 A literature has since proliferated demonstrating the safety and efficiency of remote telestroke neurology processes, including physical examination,2 imaging technology3 and treatment decision-making.4
Multiple programmes have shown mobile stroke care expedites intravenous thrombolysis.5–14 There is mixed evidence that MSU facilitate endovascular thrombectomy for patients with large vessel occlusion.5 9 15 The impact of mobile stroke on clinical outcomes is unclear, since most MSU studies do not report clinical outcomes.7–9 11–13 A Berlin-based group is the exception, in 2021 showing that 51% of MSU patients as compared with 42% of emergency medical service (EMS) patients achieved modified rankin scale (mRS) 0–1 at 3-month follow-up (p=0.001),5 updating their own earlier negative result.16
Our MSU launched in October 2018 to serve the Rochester, New York region. Given the gaps in the existing literature on mobile stroke, we sought in this first report from our programme to address two questions, which were whether intravenous tPA time savings translate into improved clinical outcomes for patients and whether mobile stroke care can benefit stroke patients eligible for endovascular therapy.
Aims/hypothesis
We hypothesised that the MSU was associated with faster times for both intravenous and intra-arterial thrombolysis and that this reduction in time-to-treatment would lead to improved long-term functional outcomes.
Methods
MSU protocol
As detailed elsewhere,17 our MSU operates 8 hours per day on week days and is dispatched along with a separate EMS unit for all 911 calls identified as suspected stroke (card 28) as defined by the Medical Priority Dispatch System (V.13.1, International Academies of Emergency Dispatch, Salt Lake City, Utah). The MSU is staffed by a specially trained registered nurse (RN) and CT technologist provided by our healthcare system and by a paramedic and emergency medical technician provided by the local ambulance service.
A teleneurologist listens to the initial patient evaluation via audiolink with the MSU RN during initial assessment. Patients with focal neurological deficits <24 hours old or with resolved transient ischaemic attack (TIA) are accepted onto the MSU. Ineligible patients are transferred by EMS. Once the patient arrives onto the MSU, the teleneurologist performs a National Institutes of Health Stroke Scale (NIHSS) via live video. Head CT is then obtained and reviewed by the teleneurologist to determine intravenous tPA eligibility.
Patients with signs and symptoms of a large vessel occlusion with symptom onset <24 hours are transported to one of the two regional comprehensive stroke centres. In these cases, the MSU provided prearrival notification to the interventional team to facilitate advanced preparation for possible emergency treatment. CT angiography (CTA) was introduced on the MSU after the dates of this analysis. A minority of cases (<5%) were transported to out-of-network facilities and these data are not included.
Study design
This study was a retrospective analysis of prospectively maintained databases of (a) all MSU calls for service and (b) Get With the Guidelines data over 26 months from October 2018 through December 2020. The study protocol was approved by our institutional review board. MSU patients were compared with patients transported by traditional EMS during MSU hours of operation. Data collected include patient demographics, clinical presentation, MSU event times, imaging, medical and procedural interventions and clinical outcomes.
Outcomes
The primary measure of safety was rates of symptomatic intracranial haemorrhage, assessed by clinical examination deterioration and head CT or MRI obtained 24 hours after intravenous tPA administration. Patients were routinely started on antiplatelet or anticoagulant therapy as determined by presumptive stroke aetiology, per institution’s evidence-based clinical practice guidelines. This protocolised management of patients by the inpatient neurology team did not differ with respect to MSU versus EMS triage mechanism. Patients were scheduled for 30-day and 90-day outpatient follow-up. Functional outcomes were evaluated at these intervals according to the mRS. In rare cases, functional outcomes were documented based on telephone assessment or outpatient assessment by other services at our institution.
Statistical analysis
Data are presented as mean and SD for continuous variables and as frequency for categorical variables. Univariate analysis was carried out using unpaired t tests and χ2 tests. Clinical outcomes were assessed as a dichotomous variable (with good considered as mRS 0–1 or 0–2) and as an ordinal variable with the Mann-Whitney U test. A threshold of p<0.05 was used to determine significance. Statistical analysis was performed using Stata V.14.2.
Results
Patient population
Over 568 days in operation, the MSU was dispatched 1489 times (2.6/day) and transported 300 patients (20% of dispatches). Patients transported by MSU had an average age of 70 years and were 49% women. Patients were identified as 61% white, 30% black, 6% Hispanic and 3% other race/ethnicities. Patients transported by MSU had an average presenting NIHSS of 8. The geographic distribution of EMS patients who received intravenous tPA or intra-arterial therapy was more widely spread than MSU patients (figure 1) with an average drive time of 23.2 min (±12.8) and 15.7 min (±5.6), respectively (p=0.0001).

Geographic distribution by zip code of patients receiving intravenous tPA or undergoing endovascular thrombectomy triaged by EMS (left) versus MSU (right). EMS, emergency medical service; MSU, mobile stroke unit; tPA, tissue plasminogen activator.
Safety
A cerebrovascular diagnosis was assigned at discharge for 66% of patients transported by MSU. A diagnosis of stroke or TIA was made for 90% of patients who received intravenous tPA; mimics included complex migraine and brain tumour. The rate of symptomatic intracranial haemorrhage after tPA administration was similar for MSU versus EMS (5.3% vs 2.7%, p=0.458).
Efficacy
Intravenous tPA was administered to 57 MSU patients and the average time from 911 call-to-tPA was 42.5 min (±9.2). Over the same period of time, traditional EMS transported 73 patients who received tPA with an 911 call-to-tPA time of 99.4 min (±35.7) (p<0.0001). Rates of ‘golden hour’ thrombolysis or tPA initiation within 60 min of last known well were 33.3% for MSU patients and 2.7% for EMS-transported patients. Among MSU patients, 7/57 (12.2%) patients received tPA in their ‘final hour’ of eligibility 3.5–4.5 hours since last known well and 4/57 (7.0%) were between 3.0 hours and 3.5 hours; the proportions for EMS patients were 17.8% and 5.5%, respectively. Door-to-needle times were 22.5 (±8.4) min and 56.1 min (±34.4) for MSU and EMS patients, respectively (p<0.0001).
For patients with premorbid mRS 0–1, the proportion who achieved mRS 0–1 at 90-day clinic follow-up was 69% for MSU and 57% for EMS (p=0.202). For patients with premorbid mRS 0–2, 75% of MSU and 61% of EMS (p=0.107) were mRS 0–2 at 90-day clinic follow-up. The distribution of mRS outcomes for patients with premorbid mRS 0–2 who received intravenous tPA is shown in figure 2. For patients with premorbid mRS 0–2 who received intravenous tPA, median mRS at 90-day follow-up was 1 for MSU and 1 for EMS while mean was 1.71 and 2.05, respectively. Mann-Whitney U test for ordinal shift (or equivalence of median) did not show a significant difference between EMS and MSU (p=0.382).

Average time from emergency alert to tPA administration for patients triaged by mobile stroke unit versus traditional EMS services (p<0.0001, left). Distribution of modified Rankin Scale at 90-day clinic follow-up for patients with premorbid mRS 0–2 (p=0.107 for dichotomous assessment of fraction 0–2 and p=0.382 for ordinal shift, right). EMS, emergency medical service; MSU, mobile stroke unit; tPA, tissue plasminogen activator.
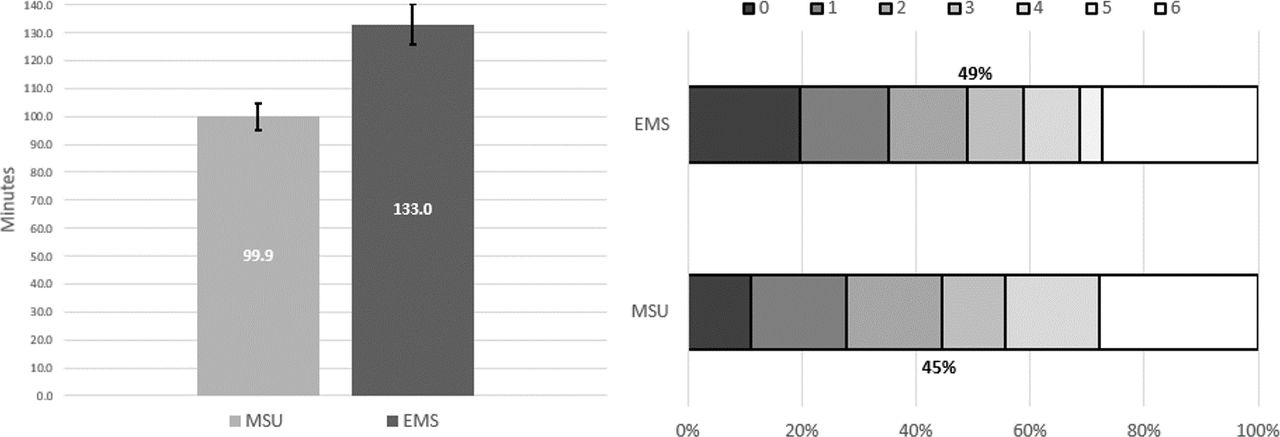
Endovascular thrombectomy was performed on 21 MSU patients with an average 911 call-to-groin puncture time of 99.9 min (±18.1). During the same interval, EMS transported 54 patients who underwent endovascular thrombectomy (ET) with an 911 call-to-groin puncture time of 133.0 min (±37.0) (p=0.0002). Door-to-groin times were 78.8 (±13.4) min and 86.2 min (±35.5) for MSU and EMS patients, respectively (p=0.369). All patients undergoing ET had CTA performed in our hospital.
There was no difference in clinical outcomes at 90-day follow-up between EMS and MSU patients who underwent endovascular thrombectomy, whether tested as a dichotomous variable for mRS 0–1 (41% EMS vs 30% MSU, p=0.406) or mRS 0–2 (49% EMS vs 45% MSU, p=0.738). For patients with premorbid mRS 0–2 who underwent ET, median mRS at 90-day follow-up was 3 for MSU and 3 for EMS while mean was 3.17 and 2.96, respectively (Mann-Whitney U test and p value 0.676) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Average time from emergency alert to groin access for patients triaged by mobile stroke unit vs traditional EMS services (p=0.0002, left). Distribution of modified Rankin Scale at 90-day clinic follow-up for patients with premorbid mRS 0–2 (p=0.738 for dichotomous assessment of fraction 0–2 and p=0.624 for ordinal shift, right). EMS, emergency medical service; MSU, mobile stroke unit.
Discussion
This single-institution retrospective study shows significantly faster intravenous thrombolysis times for patients treated by our MSU as compared with traditional EMS. We also show that MSU care expedites endovascular thrombectomy even without onboard CTA capability. Rates of functional independence at 3 months for MSU patients receiving intravenous tPA were higher than those patients transported by EMS, although this differences did not reach statistical significance.
Our experience corroborates other evidence showing a reduced interval between emergency alert and intravenous tPA administration for patients transported by MSU compared with traditional EMS services. Groups from Germany,5–7 Norway,8 Australia9 and multiple programmes in the USA10–14 have all demonstrated time savings in alert: tPA associated with MSU care. Our 911 call-to-tPA time for MSU patients of 42.5 min falls at the lower end of the range of these studies from 38 min to 62 min and our time for EMS patients of 99.4 min is in the upper part of the range from 65 min to 106 min.
Much attention has focused on mobile stroke’s ability to increase ‘golden hour thrombolysis’ or patients receiving tPA within 60 min of last known well. In this study, ‘golden hour thrombolysis’ was achieved by 33% of MSU patients and 3% of EMS, mirroring the Berlin MSU (31% vs 5% EMS).18 Less attention has been focused on the patients MSU brings inside the tPA window that are not likely to have been eligible with EMS transport. In this study, there was a 58 min disparity in 911 call-to-tPA times between MSU and EMS. Among MSU patients, 12% received tPA from 3.5 hours to 4.5 hours since last known well and 7% were between 3.0 hours and 3.5 hours. These might be called ‘final hour’ patients and represent 10%–20% of MSU tPA cases.
The vast majority of MSU studies do not report functional outcomes.7–9 11–13 Among those that do, Ebinger et al originally published equivocal functional outcomes in a cohort of patients receiving intravenous tPA between 2011 and 2015 that consisted of 305 MSU patients treated at an average alert:tPA interval of 48 min compared with 353 conventionially triaged patients at an interval of 82 min (p<0.0005). There was no significant difference in the prespecified primary outcome, which was 3-month mRS of 0–1 (53% vs 47%, respectively, p=0.14). Some secondary outcomes favoured MSU care (mRS 0%–3 83% vs 74%, p=0.004), while others were negative (ordinal analysis of the entire mRS range, p=0.10).16
Ebinger et al subsequently published an updated experience from 2017 to 2020, demonstrating improved functional outcomes associated with MSU care.5 The study compared 794 MSU and 749 EMS patients with a stroke dispatch code and no contraindication to intravenous thrombolysis or embolectomy. At 3-month follow-up, mRS of 0 or 1 was achieved by 51% vs 42% of MSU and EMS patients, respectively (p=0.001). The newfound significance was due to study design: including all transported patients better captures and reflects the higher proportion eligible for therapy with faster MSU care. The authors acknowledged the need to replicate their results in other MSU programmes.
We observed a trend towards improved functional outcomes with 75% of MSU tPA patients achieving 90-day mRS 0–2 compared with 61% of EMS tPA patients (p=0.107). Our findings represent a higher proportion of patients achieving functional independence than is typical for intravenous tPA. In a meta-analysis of 12 trials and 7012 patients, Wardlaw et al reported mRS 0–2 at final follow-up for 46% of patients who received intravenous tPA within 6 hours of last known well.19 The Berlin group reported 3-month mRS 0–2 in 63% of MSU patients receiving intravenous tPA.16 Although there are multiple confounders, earlier administration of tPA associated with MSU care may explain these improved functional outcomes.
Previous work has demonstrated equivalence of telestroke neurology processes,20 including physical examination,2 head CT acquisition and interpretation3 and treatment decision-making4 when compared with conventional, in-person evaluation. Accordingly, tPA administration to stroke mimics and symptomatic haemorrhage rates remain important safety parameters of any mobile stroke programme. In this experience, a final diagnosis of stroke or TIA was given to 90% of MSU patients who received tPA, similar to the few series21 that report this number. Post-tPA parenchymal imaging was obtained on all patients and showed symptomatic intracranial haemorrhage in 5%. This was not statistically different than for EMS/ED patients who received tPA (3%) and was similar to other mobile stroke programmes.21 In meta-analyses, the rates of symptomatic ICH after intravenous thrombolysis have been reported to be 3.3%.22
The evidence that MSU care facilitates endovascular thrombectomy is mixed. Three prior studies compared arterial puncture times for MSU and EMS patients with conflicting observations. Ebinger et al actually observed a prolonged time to arterial puncture for MSU patients: 137 min in 103 MSU patients and 125 min in 113 conventional ambulance patients.5 The authors noted that despite availability of CTA onboard the MSU, vessel imaging was repeated on hospital arrival at interventionists’ request to capture aortic arch and great vessel anatomy. Zhao et al reported 41 ET performed on MSU patients and 140 cases transported by traditional ambulance from 2017 to 2018 with average dispatch-to-arterial puncture times of 119.5 and 170 min, respectively (p<0.001). This disparity could have been an artefact of inappropriate triage, however, as the control cohort included both direct presentation and interhospital transfers.9 The Benefits of Stroke Treatment Delivered Using a Mobile Stroke Unite (BEST-MSU) group consisting of three MSU sites in Houston, Memphis and Denver, shared a series of 94 MSU ET versus 67 EMS ET cases over 4 years from 2014 to 2018 and showed a small time savings associated with MSU care. Door-to-groin time was 89 min for MSU patients versus 99 min for EMS (p=0.01).15 Door-to-puncture is not an ideal metric for mobile stroke, however, as it may obscure prolonged dispatch of a specialty ambulance. Importantly, given the time required to obtain scans, rates of noninvasive vascular imaging (75%–77%) and perfusion imaging (31%–35%) were similar in both the MSU and EMS BEST-MSU cohorts.
We demonstrated time savings from alert to groin puncture for MSU patients undergoing endovascular thrombectomy versus EMS patients. We did not have CTA capability onboard the MSU during our enrollment period, so both EMS and MSU patients required routine CTA on hospital arrival. We believe strongly that time savings were largely attributable to early notification and preparation of the operating room staff. The introduction of CTA on-board the MSU may increase its efficiency with endovascular thrombectomy.
Significant socioeconomic disparities exist in stroke treatment, both intravenous thrombolysis and endovascular thrombectomy. Higher socioeconomic status is associated with shorter time to intravenous tPA administration and lower in-hospital mortality.23 Mechanical thrombectomy utilisation is higher among privately insured and white patients as compared with minorities.24 Given the existing disparities, it is imperative that outreach programmes, like a MSU, are equitably distributed across the community they serve. In our community, the zip codes with the lowest median household income are predominantly located in the city of Rochester. Our MSU is busiest in these areas. Looking at the 10 zip codes in the Rochester metro area with the lowest median household income, these accounted for 40% of MSU patients receiving tPA or ET as compared with 13% of EMS patients.
A particular limitation of this study is the disparate geographies from which MSU and EMS patients originated. As mentioned in the Methods section, our MSU was initially piloted within Rochester city limits. Our primary outcome measure was time from alert to tPA start or groin puncture. This metric includes time from dispatch to scene arrival (likely higher for the MSU than local EMS) and drive time from the scene to our medical centre. This observation is presumed to be similar to most other MSU studies, either because EMS and MSU alternate responsibility for identical catchments10 18 or because earlier time periods were used as a control.9 21 We calculated the drive time from the zip code whence each patient originated to our medical centre. For MSU patients, this averaged 16 min as compared with 23 min for EMS. This 7 min difference comprised a fraction of the reduction associated with MSU care in both 911 call-totPA (57 min) and 911 call-to-puncture (33 min) times. Door-to-tPA or groin does not reflect the full spectrum of stroke care but does control for remote geographies and was significantly lower for MSU patients receiving intravenous thrombolysis although not endovascular thrombectomy.
Conclusions
Mobile stroke care in our community was associated with faster 911 call-to-tPA and 911 call-to-groin times for both intravenous and intra-arterial thrombolysis. Emerging evidence from larger studies now exists that faster MSU treatment times result in improved outcomes, which we saw in patients receiving intravenous tPA.
Data availability statement
Data are available upon reasonable request. Deidentified participant data are available upon reasonable request to matthew_bender@urmc.rochester.edu.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by URMC RSRBSTUDY00006021Consent was waived by our institutional review board.
References
Footnotes
Contributors All authors were involved in conception of the mobile stroke unit and data acquisition; all critically revised the manuscript and approved its final version; all agreed to accountability for the work’s integrity. The underlying data were verified by MTB, DP and WAB. MTB drafted the manuscript. MTB and WAB performed data analysis. MTB is the guarantor of study integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.