Article Text

Abstract
Background The optimal treatment for patients with symptomatic severe intracranial atherosclerotic disease is not well established. Angioplasty and stenting have been attempted, with controversial results, mainly attributed to perioperative complications and a high incidence of restenosis or in-stent restenosis. Drug-coated balloons (DCBs) have shown encouraging results for coronary and peripheral artery disease, without convincing data for intracranial vasculature.
Objectives To assess the feasibility, clinical and angiographic outcomes of DCBs for patients with intracranial de novo atherosclerotic disease.
Methods Between September 2016 and September 2017, details of 30 patients with 31 arteries treated with DCBs for symptomatic severe intracranial atherosclerotic disease (≥70% stenosis or chronic total occlusion) were retrospectively collected in our centre. All lesions were predilated with conventional balloons. Periprocedural complications and clinical and vascular imaging follow-up outcomes were analysed.
Results All arteries were successfully dilated with DCBs and 29 (93.5%) arteries achieved good antegrade perfusion, with remedial stenting for two arteries. Two patients presented with new ischemic stroke after the procedure. Over a mean follow-up of 9.8±2.6 months, no patient had recurrent ischemic symptoms. Repeat vascular imaging was performed at 7.0±1.1 months, with cerebral angiography in 24 patients (25 arteries) and MR angiography in six patients (six arteries). Only one (3.2%) artery presented with angiographic asymptomatic restenosis.
Conclusions This study suggests that DCB dilatation may be a safe and effective alternative for intracranial de novo atherosclerotic disease.
- angiography
- atherosclerosis
- balloon
- stroke
Statistics from Altmetric.com
Introduction
Intracranial atherosclerosis is a major cause of cerebral ischemic stroke, especially in Chinese patients, and is associated with a high risk of recurrent stroke.1–4 Angioplasty and stenting have been attempted for patients refractory to medication. However, since the Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial5 6 and the Vitesse Intracranial Stent Study for Ischemic Therapy (VISSIT) trial7 demonstrated the negative results of using stents for patients with symptomatic intracranial stenosis, there is still no acknowledged treatment for this patient group. The discouraging results were mainly attributed to perioperative complications and a high incidence of restenosis or in-stent restenosis (ISR), which is thought to be caused by intimal hyperplasia. Previous studies have shown that the incidence of ISR is high and is associated with an increased risk of recurrent ischemic events.8 9 In the SAMMPRIS trial, the 1–3 year incidence of symptomatic ISR was approximately 9.6–14.0%, which accounted for most non-procedural cerebral infarctions10 and was much more intractable to further endovascular treatment.
In recent years, drug-coated balloons (DCBs), coated with antiproliferative drugs, have been well recognized for their ability to inhibit intimal hyperplasia.11 During DCB dilatation, the drug can penetrate into the vessel wall. Previous studies have shown that DCB dilatation can effectively prevent and treat ISR and shows promise in newly formed lesions of coronary and peripheral small arteries.12–15 The restenosis rate was much lower than that with conventional balloon dilatation and stenting.16 Recent research suggested that a paclitaxel DCB is a viable alternative to drug-eluting stents,17 with the added advantage of avoiding a permanent implant. The new advent of Neuro Elutax DCB further increased the feasibility of using a DCB in intracranial arteries.18 However, the application of a DCB has not been systematically explored for intracranial de novo atherosclerosis disease. Therefore, we report our initial experience using DCBs for symptomatic severe intracranial de novo atherosclerotic stenosis or chronic total occlusion with clinical and angiographic follow-up outcomes.
Materials and methods
Study population
We retrospectively reviewed our prospective stroke intervention database to identify patients who had been treated with DCBs for symptomatic, severe (stenosis degree ≥70% or chronic total occlusion) intracranial atherosclerotic disease between September 2016 and September 2017. All patients had a recurrent transient ischemic attack (TIA) or ischemic stroke after standard medical therapy with a combination of antithrombotic agents and risk control. Patients suspected of having Moyamoya disease, vasculitis, dissection, or emboligenic heart disease were not included. The degree of stenosis was initially assessed by non-invasive CT angiography or magnetic resonance angiography (MRA) and finally confirmed by digital subtraction angiography (DSA). All patients or their authorized family members were explicitly told about the risks and benefits of endovascular treatment, including stent implantation and balloon dilatation, and gave informed consent to the off-label use of the coronary DCB. The procedure was approved by our institutional review board.
Preprocedural medical management
All patients were given individual standard medical treatment and lifestyle interventions, including antihypertensive agents, antidiabetic drugs, and statins. Dual antiplatelet treatment (DAPT) with 100 mg aspirin and 75 mg clopidogrel was routinely maintained for at least 5 days before intervention.
Intervention technique
The endovascular procedures were performed under general anaesthesia using a 6F or 8F guiding catheter. Intravenous heparin boluses were given to maintain the activated clotting time between 250 s and 300 s during the procedure. Stenosis grades were determined according to the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) study.3 The vessel pathway was comprehensively assessed before intervention. The lesion was traversed with a coaxial assembly of an Excelsior SL-10 soft microcatheter (Stryker Neurovascular, Cork, Ireland) and Synchro2 microguidewire (Stryker Neurovascular, Utah, USA). For those with an excessively tortuous vessel pathway, a distal access catheter (Concentric Medical, California, USA) was applied. All lesions were initially predilated with a conventional balloon (Gateway balloon, Boston Scientific, Minnesota, USA), which was supposed to facilitate the advancement of the more rigid DCB over the lesion.19 20 A paclitaxel-coated coronary DCB (SeQuent Please, B. Braun, Berlin, Germany) was used in this study. The diameter of the DCB was selected to correspond to about 80–100% of the diameter of the normal vessel, and was 0.5–1 mm larger than a conventional balloon. A DCB was needed to cover the whole lesion and was slowly inflated at nominal pressure for 60 s to allow for the transition of paclitaxel from the balloon surface into the vessel wall. After deflation and withdrawal of the DCB, an angiogram was reperformed to evaluate the lumen and to exclude vessel dissection, perforation, or distal embolization. The intervention ended with a residual stenosis ≤50% and stable antegrade perfusion (2b/3), which was evaluated by the modified Thrombolysis in Cerebral Infarction scale. If the residual stenosis was >50% and the antegrade perfusion was unstable, remedial stenting implantation was performed. Other complications were resolved according to the interventionist’s discretion.
Postprocedural management
After the procedure, patients were routinely sent to the neurological intensive care unit for continuous observation and blood pressure monitoring to keep the systolic blood pressure <130 mm Hg. Complete neurologic examination, including assessment of the National Institutes of Health Stroke Scale score, was performed by the neurologist within 24 hours after the procedure. Clinical events including any stroke, TIA, or death were documented. DAPT with aspirin 100 mg and clopidogrel 75 mg/day was maintained for 3 months for patients with only DCB dilatation and 6 months for patients with remedial stenting implantation.
Data collection and follow-up outcome
Demographic, clinical, angiographic, and procedural data were collected. All patients were followed up clinically at 1 month, 3 months, 6 months, 1 year, and yearly thereafter. They were scheduled to return for a vascular imaging examination at 6 months. Cerebral angiography was preferred, but MRA was also accepted for patients refusing angiography. Angiographic restenosis was defined as a diameter of the stenosis of >50% of the DCB-dilated target artery segment. Disagreements were resolved by consensus. Symptomatic restenosis was defined as angiographic restenosis associated with ischemic symptoms of the offending vessel territory.
Statistical analysis
Descriptive statistics were used in this study. Continuous variables are expressed as the mean±SE or as the median with IQR. Categorical variables are expressed as numbers and percentages. The Shapiro-Wilk test was used to test the distribution of the variables for normality. Statistical analysis was performed using SPSS version 19.0 for Windows (SPSS Inc, Chicago, Illinois, USA).
Results
Patient demographics
Baseline clinical characteristics of the 30 patients are listed in table 1. The mean age was 57.4±8.3 years, with male predominance (24, 80.0%). The primary medical history of these patients included hypertension (23, 76.7%), hyperlipidaemia (12, 40.0%), diabetes mellitus (10, 33.3%), and coronary artery disease (6, 20.0%). Half of the patients (15, 50%) were current smokers.
Baseline clinical characteristics (n=30)
Angiographic and procedural characteristics
Thirty-one arteries were treated with DCBs, including 12 (38.7%) middle cerebral arteries, 17 (54.8%) basilar arteries, and 2 (6.5%) intradural vertebral arteries. Nineteen (61.3%) arteries exhibited severe stenosis (82.1±8.9%), and 12 (38.7%) arteries exhibited chronic total occlusion. All DCBs were successfully delivered to the lesions and dilated. Good antegrade perfusion was achieved in 29 (93.5%) arteries with 20% (IQR 10–40%)) residual stenosis. Another two (6.5%) arteries received remedial stent implantation owing to residual stenosis >50% and unstable antegrade perfusion after DCB dilatation. Vessel dissection occurred in two (6.5%) patients, without remedial stent implantation because of no flow limitation. No perforation, distal embolization, or other device-related complications occurred during the procedure. The details are listed in table 2.
Angiographic and procedural characteristics (n=31)
In-hospital and follow-up outcomes
As shown in table 3, two patients presented with a new minor ischemic stroke, including dizziness and unilateral limb weakness, in the hospital after the procedure. Both patients had newly formed basilar artery lesions and were neurologically independent with conservative medical therapy before discharge. No death occurred. During the 9.8±2.6 month clinical follow-up period, there were no recurrent cerebral ischemic events, including TIA or stroke. During the 7.0±1.1 month vessel imaging follow-up period, cerebral angiography was obtained for 24 patients for 25 arteries (figure 1). The other six patients with six arteries were assessed by MRA. Only one (3.2%) artery was found to exhibit angiographic restenosis of approximately 80%. Because no recurrent symptoms could be documented, the artery was temporarily left without further vessel revascularization. Vessel dissections of two patients were completely healed. There was no ISR for the two patients with bailout stent implantation (figure 2).

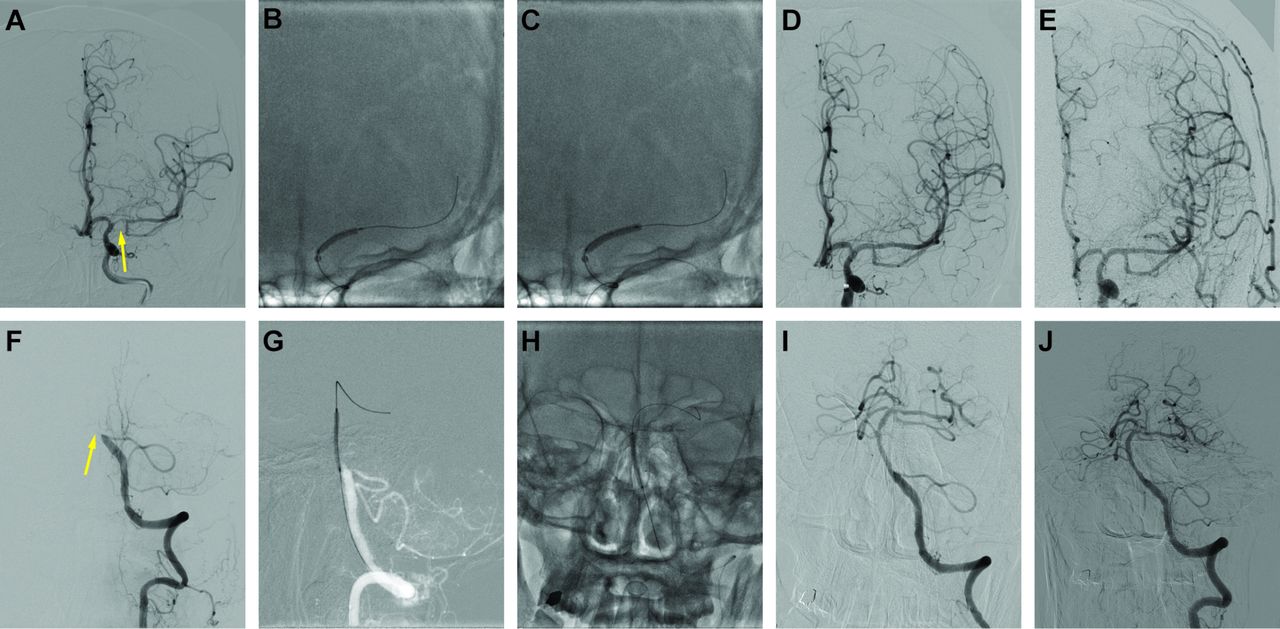
Example of drug-coated balloon (DCB) dilatation for intracranial atherosclerotic disease and follow-up. Images (A–E) show the cerebral angiography results, during the procedure and follow-up, of DCB dilatation for a patient with severe stenosis of the left middle cerebral artery. (A) Severe left middle cerebral artery stenosis (arrow). (B) Predilatation with a conventional balloon. (C) DCB dilatation after predilatation. (D) Angiographic result after the procedure. (E) Angiographic result at 6.0 months' follow-up. Images (F–J) show the cerebral angiography results of DCB dilatation for a patient with chronic total occlusion of the basilar artery during the procedure and follow-up. (F) Chronic total occlusion of the basilar artery (arrow). (G) Predilatation with a conventional balloon. (H) DCB dilatation after predilatation. (I) Angiographic result after the procedure. (J) Angiographic result at 8.5 months' follow-up.

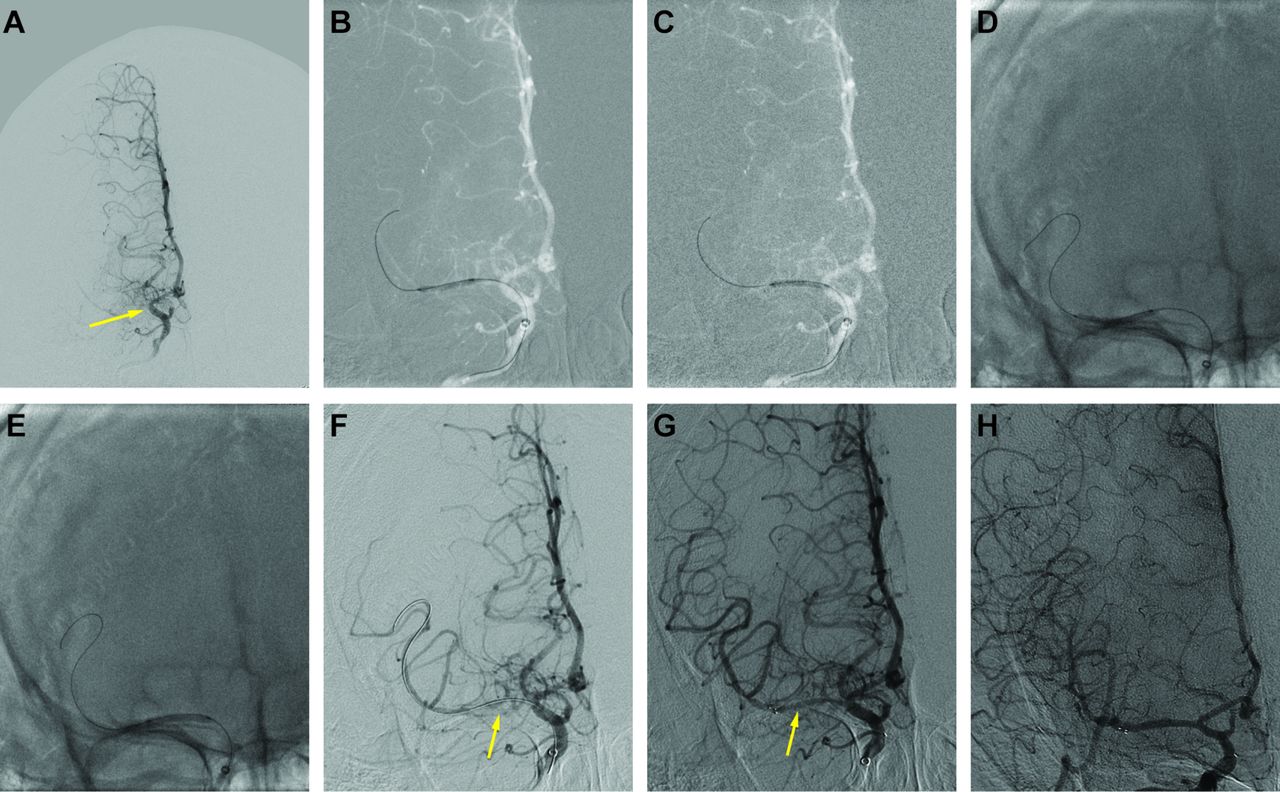
Example of remedial stent implantation after drug-coated balloon (DCB) dilatation and follow-up. The images (A–H) show the cerebral angiography results of remedial stent implantation after DCB dilatation for a patient with chronic total occlusion of the right middle cerebral artery during the procedure and follow-up. (A) Chronic total occlusion of the right middle cerebral artery (arrow). (B,C) Predilatation with conventional balloons for the distal and proximal lesions. (D,E) DCB dilatation for the distal and proximal lesions after predilatation. (F) Angiographic result after DCB dilatation with residual stenosis >50% and poor antegrade perfusion (arrow). (G) Angiographic result after remedial stent implantation (arrow). (H) Angiographic result at 6.3 months' follow-up.
Clinical and imaging outcomes in-hospital and during follow-up
Discussion
In this study, 31 intracranial arteries were successfully dilated with DCBs for symptomatic de novo severe stenosis or chronic total occlusion. During follow-up, no patient had recurrent clinical ischemic symptoms and only one artery was found to have asymptomatic angiographic restenosis. We preliminarily demonstrated the feasibility and efficacy of DCB dilatation for symptomatic intracranial de novo atherosclerotic disease.
Intracranial atherosclerosis is an independent risk factor for cerebral ischemic stroke. Because of the high incidence of ISR and other perioperative complications of angioplasty and stenting, the optimal treatment for this patient group is still in question.9 10 The ISR rate may be as high as 32% for bare metal stents, which accounts for 39% of recurrent ischemic symptoms.21 Therefore, promising treatment options for symptomatic intracranial atherosclerotic disease, with a minimum risk of restenosis or ISR, is mandatory.
With the growth in interventional devices, the DCB was developed and has been increasingly recognized and recommended for endovascular treatment. As it is coated with paclitaxel, the DCB can effectively inhibit intimal hyperplasia and reduce the risk of restenosis.12 Previous studies have demonstrated the low risk of restenosis and ISR in coronary and peripheral arteries. For intracranial vasculature, most studies have focused on the prevention and treatment of ISR. Recently, Gruber et al reported eight patients treated with Neuro Elutax SV DCBs for intracranial symptomatic high-grade atherosclerotic stenosis and preliminarily demonstrated their superiority to stenting.18
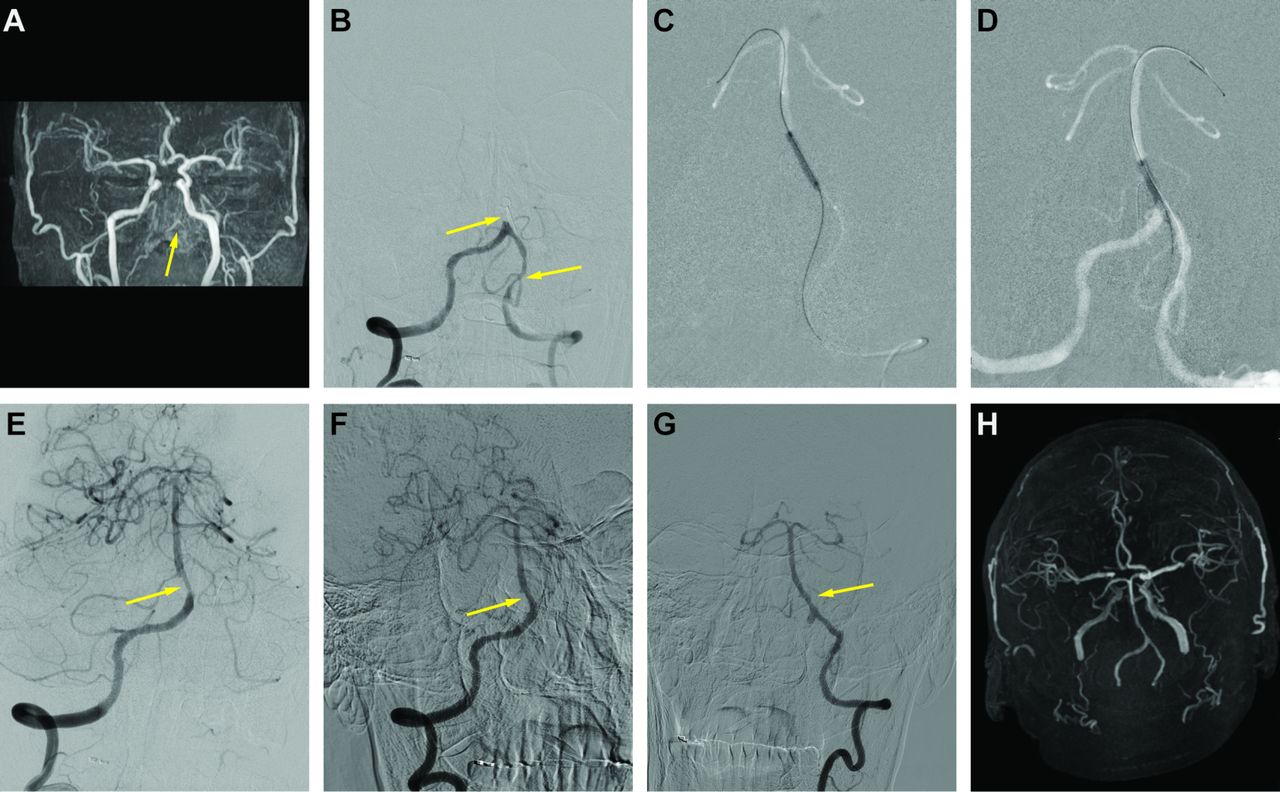
In our study, 31 arteries were treated with DCBs, and 29 arteries achieved good lumen patency and antegrade flow without remedial stenting. During follow-up, no recurrent cerebral ischemic events occurred, and only one artery presented with asymptomatic angiographic restenosis. These results are similar to those of previous reports. Moreover, without a mechanical scaffold, using a DCB removes the technical burden of treating ISR and allows patients to receive non-invasive magnetic resonance examination. In our study, as for coronary artery disease,8 the DCB seems to play a significant role in vascular remodeling and patency improvement for intracranial arteries. As shown in figure 3, residual stenosis of approximately 50% of the basilar artery was found after DCB dilatation. Because of the stable antegrade perfusion, no stent was implanted. At approximately 8.0 months' follow-up, the lumen was almost normal without significant residual stenosis.

{kind=link}
{kind=link}
{kind=link}
Example of the effect of vascular remodeling after drug-coated balloon (DCB) dilatation. Images (A–H) show the results of DCB dilatation for a patient with chronic total occlusion of the basilar artery and stenosis of the left intradural vertebral artery during the procedure and follow-up. (A) MR angiography shows poor development of the bilateral vertebral and basilar arteries (arrow). (B) Cerebral angiography shows chronic total occlusion of the basilar artery and severe stenosis of the left intradural vertebral artery (arrows). (C) Predilatation with a conventional balloon. (D) DCB dilatation after predilatation. (E) Angiographic result after DCB dilatation with residual stenosis ≈50%, but stable antegrade perfusion (arrow). (F,G) Angiographic results shows that at the 8.0-month follow-up the lumen of basilar artery was larger than that at postprocedure (arrow). (H) MR angiography result at 8.0 months' follow-up.
DAPT is routinely given after endovascular treatment. Maintenance of DAPT is recommended for at least 6–12 months for patients after stent implantation. This would potentially increase the risk of haemorrhage. However, according to guidelines, it has been proved that DAPT can be taken for just 1–3 months after DCB treatment,20 22 which would decrease the risk of haemorrhage and benefit those planning to receive other surgical treatment.
In our study, the available DCBs were initially designed for coronary arteries. Therefore, they might have been somewhat rigid and of an unsuitable size for intracranial arteries. Thus, it is important to prepare the lesion with adequate predilatation. Moreover, evaluation of the vessel path is of great importance. In our study, the distal access catheter was used for patients with an excessively tortuous vessel pathway, which might have accounted for the higher arrival rate of DCBs compared with a previous report.19 Two patients required remedial stent implantations for residual stenosis >50% after DCB dilatation. Both patients had good clinical and angiographic follow-up outcomes. Two patients with basilar artery stenosis presented with new ischemic symptoms after the procedure. The stroke was thought to be associated with small perforating artery occlusion, which is not uncommon during endovascular treatment of the basilar artery. Fortunately, the two patients recovered well with conservative treatment before discharge.
Our study has several limitations. First, this was an observational study with a limited number of patients. Second, because there was no implantation in the endovascular treatment, MRA follow-up was performed in some patients, a detail that may partly jeopardize the consistency. Third, the follow-up time was short, so the effect needs to be re-evaluated with long-term follow-up.
Conclusions
In conclusion, this single-centre series study shows that the use of DCBs may be feasible and safe for the treatment of symptomatic severe intracranial atherosclerotic disease. Further prospective randomized studies with larger patient numbers are mandatory to establish the clinical efficacy and indications.
References
Footnotes
JH and JZ contributed equally.
Contributors Study concepts and design: JH, JuZ, XZ, JiZ, and YS. Statistical analysis: WZ, MZ. Manuscript composition: JuZ, XZ, LS, and WW. Manuscript revision: JH, JuZ, and YS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.