Article Text

Abstract
Background and purpose Leukoaraiosis (LA) is defined as ischemic white matter lesions associated with increased stroke risk and poor post-stroke outcomes. These lesions are likely the result of diffuse angiopathic changes affecting the cerebral small vessels. We investigated whether pre-existing LA burden is associated with outcomes in patients with large cerebral artery occlusion undergoing intra-arterial therapy (IAT) for acute ischemic stroke (AIS).
Methods We analyzed consecutive AIS subjects undergoing IAT from the institutional Get With The Guidelines-Stroke database enrolled between January 1, 2007 and June 30, 2009, who had National Institutes of Health Stroke Scale scores of ≥8, baseline diffusion weighted imaging volume ≤100 mL, and evidence of proximal artery occlusion (PAO) on pre-IAT computed tomography angiography (CTA). LA volume (LAv) was assessed on fluid attenuated inversion recovery MRI using a validated semi-automated protocol. We used CTA for collateral grade, post-IAT angiogram for recanalization status (Thrombolysis in Cerebral Infarction score ≥2b), and the 24 h head CT for symptomatic intracranial hemorrhage. Logistic regression was used to determine independent predictors of 90 day post-stroke good functional outcome (modified Rankin Scale score ≤2) and mortality.
Results Increasing LAv independently reduced the odds of good collateral grade (OR 0.85, 95% CI 0.73 to 0.98). Good functional outcome was independently predicted by intravenous tissue plasminogen activator use (OR 12.86, 95% CI 2.20 to 76.28), and recanalization status (OR 6.94, 95% CI 1.56 to 30.86). Mortality was independently associated with recanalization status (OR 0.08, 95% CI 0.01 to 0.51), age (OR 1.08, 95% CI 1.01 to 1.15), and antecedent use of hypoglycemic agents (OR 6.55, 95% CI 1.58 to 54.01).
Conclusions Severity of LA is linked to poor collateral grade in AIS patients undergoing IAT for PAO; however, greater LAv appears not to be a contraindication for acute intervention.
Statistics from Altmetric.com
Introduction
While intravenous (IV) thrombolysis (tissue plasminogen activator (tPA)) has been firmly established as the standard of care for acute ischemic stroke (AIS), the role of endovascular intra-arterial therapies (IAT) remains under intense scrutiny for definitive evidence of clinical benefit.1–3
The best approach to endovascular treatment, including patient selection strategies, optimum device selection, and outcome definitions, are being debated.4–8 In addition to operator experience, and device effectiveness, patient selection is considered one of the most important questions in IAT therapy for AIS. Effective systems to predict favorable outcomes after IAT are currently pursued by many.9 Among well known risk factors for poor stroke outcomes9 such as older age, elevated blood glucose, history of hypertension, diabetes mellitus, and/or atrial fibrillation, initial stroke severity, measured as National Institutes of Health Stroke Scale (NIHSS) score, and neuroimaging markers, such as infarct size, have been also associated with poor outcomes after IAT.7 ,10
Severity of leukoaraiosis (LA), a radiographic finding that corresponds to white matter lesions of ischemic origin, has been linked to poor outcomes after AIS, including those cases receiving thrombolysis.11–14 Pre-existing burden of LA has been previously shown to independently predict worse tissue11 and clinical12 post-stroke outcomes. Whether the mechanisms of worsening in these patients are related to hemorrhagic transformation following thrombolysis—either systemic or intra-arterial—remains unclear, given that some previous reports indicated increased risk of symptomatic intracranial hemorrhage in patients with advanced LA.14 ,15
Another potential explanation of worse outcomes after IAT in these subjects might be the link between severe LA and poor collateral flow. Insufficient collateralization is a known predictor of poor outcomes after AIS due to proximal cerebral artery occlusions (PAO).16 ,17 We hypothesized that increasing burden of LA is a radiographic marker of globally impaired cerebral circulation that manifests in diffuse small cerebral vasculopathy, which in turn leads to limited recruitment of the collaterals in the setting of PAO. To test this hypothesis, we sought to evaluate the association between severity of LA and functional outcomes in AIS patients undergoing IAT for PAO. A secondary analysis was performed on the relationship between LA and recruitment of the leptomeningeal collaterals.
Methods
Study subjects
This was a retrospective analysis of prospectively collected data on all consecutive patients >18 years of age, who presented directly to our emergency department between January 1, 2007 and December 31, 2011 with a diagnosis of AIS, evidence of PAO on acute computed tomography angiography (CTA), and who underwent IAT based on our institutional protocol.18 Patients were selected as ‘likely to benefit’ for IAT based on: (1) MRI and CT brain imaging ≤6 h from last known well time, (2) initial NIHSS score ≥8 (or evidence of moderate–severe aphasia), (3) baseline infarct volume of ≤100 mL, and (4) evidence of PAO in the anterior circulation (internal carotid artery, or middle cerebral artery M1 or proximal M2 occlusion) on CTA.18 Of 95 AIS patients who underwent IAT based on this protocol, 73 had MRI available for volumetric assessment of LA and were included in this analysis.
Patient characteristics, clinical presentation, acute treatments, including IV tPA and IAT, as well as contraindications or warnings, were documented in the institutional Get With The Guidelines (GWTG)-Stroke database, and the reason for withholding acute treatments were abstracted from medical records by a trained abstracter. All patients underwent clinical evaluation by a neurologist, acute diagnostic neuroimaging, and laboratory testing on arrival to the emergency department. All elements of the study were approved by the local institutional review board.
Neuroimaging analysis
LA volume
Severity of LA was assessed using a previously published semi-automated volumetric analysis method with high inter-rater reliability.13 MRI were acquired on 1.5 T Signa scanners (GE Medical Systems, Milwaukee, Wisconsin, USA), and all scans were converted to analyze format using MRIcro software (University of Nottingham School of Psychology, Nottingham, UK, http://www.mricro.com). Computer assisted determination of LA volume (LAv) included: (a) creating LA maps using axial T2 fluid attenuated inversion recovery sequences, (b) aligning these maps with the corresponding diffusion weighted imaging (DWI) sequences for exclusion of acute ischemia, edema, and chronic territorial infarcts, and (c) calculating the total LAv by doubling the LAv in the hemisphere unaffected by the stroke and adjusted for head size, as previously described.13 All images in this study were assessed by two investigators (NSR and KF) prospectively, with the sample intraclass correlation coefficient for LAv of 0.97, and blinded to patient CTA characteristics, recanalization status, and clinical outcomes.
Infarct volume
Acute infarcts were outlined on DWI MRI using analyze 10.0 (AnalyzeDirect, Overland Park, Kansas, USA), and DWI volume (DWIv) was calculated in milliliters. In cases with significant cerebral edema, volume increases from swelling were accounted for by excluding infarcted tissue that extended across the midline or produced ventricular effacement (compared with pretreatment ventricular configuration). Edema producing sulcal effacement was not excluded. Readers (AJY or ZC) were blinded to the study outcomes.7
Collateral grade
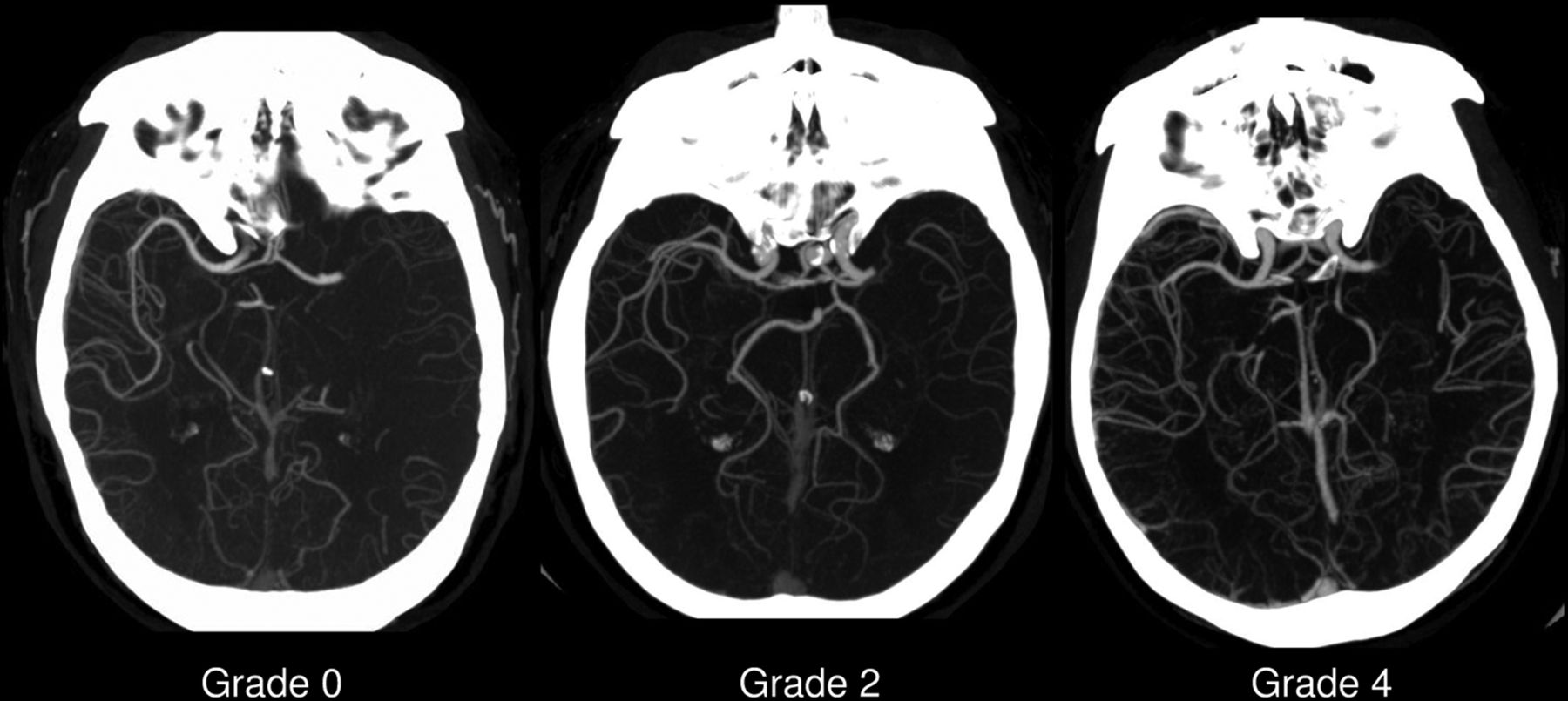
Collateral circulation was graded based on a five point previously published scale,19 which compares collateral flow in the infarcted middle cerebral artery territory with the contralateral territory: 0=no collaterals in >50% of an M2 territory; 1=decreased collaterals in >50% of an M2 territory; 2=decreased collaterals in <50% of an M2 territory; 3=equal collateral circulation on the infarcted side; and 4=greater collateral circulation on the infarcted side (figure 1). Collateral grading was conducted by a trained investigator (D-VG) and validated by an experienced neuroradiologist (AJY).19 Collateral grade was dichotomized as good (4, 3, 2) versus poor (0, 1).19
{kind=link}
Collateral grade on reconstruction of CT angiogram images.
Study outcomes and outcome definitions
The on-call neurointerventional team performed IAT according to their standard practice during the time of the study, using IA tPA infusion, as well as the Penumbra system (Penumbra Inc, Alameda, California, USA) and MERCI devices (Concentric Medical, Mountain View, California, USA). Successful recanalization was defined as post-interventional flow at Thrombolysis in Cerebral Infarction (TICI) 2b or better on the TICI scale.4
All IAT patients underwent 90 day clinical outcome assessment using the modified Rankin Scale (mRS) score. Clinical outcomes were defined as good (mRS≤2) versus poor (mRS>2).20 Mortality was recorded at hospital discharge and at the 90 day follow-up.
Statistical analysis
Continuous variables were analyzed using the Student's t test or the Wilcoxon rank sum test, as appropriate. Fisher's exact test was used to analyze proportions. Categorical variables were analyzed using χ2 analysis. Spearman's rank correlation coefficients were used for correlation analyses. Univariate and multivariable logistic regression analyses were performed to evaluate predictors of good collateral grade, good clinical outcome, and mortality. All variables associated with a specific outcome in univariate regression analysis at a prespecified nominal p value of 0.2 or less were included in the multivariable analyses of this outcome. Significance level was set at p<0.05 for all analyses (SAS V. 9.2 for Windows, SAS Institute Inc, Cary, North Carolina, USA).
Results
Baseline characteristics of the 73 subjects included in this analysis are presented in table 1. This particular cohort was similar in demographics, stroke severity, and comorbidity profile to previously reported cohorts of AIS patients undergoing IAT.2 ,4 ,7 ,10
Patient characteristics and outcomes among acute ischemic stroke patients undergoing intra-arterial therapy (n=73)
In univariate analysis, the odds of good collateral grade decreased with increasing NIHSS score (OR 0.83, 95% CI 0.72 to 0.95), admission glucose level (OR 0.98, 95% CI 0.97 to 0.99), DWIv (OR 0.94, 95% CI 0.88 to 0.99), and decreasing LAv (OR 0.90, 95% CI 0.82 to 0.99). Of these, NIHSS (OR 0.79, 95% CI 0.65 to 0.93) and LAv (OR 0.85, 95% CI 0.73 to 0.98) remained significant in multivariable analysis (table 2).
Outcome predictors among acute ischemic stroke patients undergoing intra-arterial therapy (n=73)
Recanalization status was associated with good functional outcome (OR 2.94, 95% CI 1.63 to 15.34) whereas hypertension (OR 0.30, 95% CI 0.10 to 0.89), LAv (OR 0.88, 95% CI 0.77 to 0.99), and NIHSS (OR 0.83, 95% CI 0.76 to 0.99) decreased the odds of good outcome. In multivariable analysis, only IV tPA use (OR 12.86, 95% CI 2.20 to 76.28) and recanalization (OR 6.94, 95% CI 1.562 to 30.86) were independent predictors of good functional outcome (table 2). Recanalization also reduced the odds of mortality (univariate OR 0.09, 95% CI 0.02 to 0.41; multivariate OR 0.08, 95% CI 0.01 to 0.51) whereas older age (univariate OR 1.06, 95% CI 1.01 to 1.11, multivariate OR 1.08, 95% CI 1.01 to 1.15) and antecedent use of hypoglycemic agent (univariate OR 6.55, 95% CI 1.79 to 23.95, multivariate OR 9.23, 95% CI 1.58 to 54.01) independently increased its odds (table 2).
Discussion
Our findings demonstrate that in AIS patients who are carefully selected for IAT based on previously published criteria,18 recanalization, and IV tPA use, but not severity of LA, are independently associated with good long term functional outcomes. Furthermore, recanalization significantly reduced the odds of mortality in this patient population. When adjusted for known clinical and radiographic determinants of IAT outcomes,2 ,9 ,21 models including LAv showed no increased risk of hemorrhage, and no independent effect on functional outcome or mortality in this study.
Our data demonstrate that good collateral grade is independently associated with reduced LAv. This finding supports the underlying hypothesis that increasing burden of LA is a marker of global cerebrovascular dysfunction, which may manifest as limited recruitment of pial collaterals in the setting of PAO leading to acute ischemia. Furthermore, it clarifies the relationship between LA and collaterals in AIS, compared with earlier studies. The previously reported lack of association between the two22 used a semiquantitative assessment of LA severity, as opposed to volumetric analysis, which we used in this study. Furthermore, their analysis included distal middle cerebral artery and posterior circulation AIS, a subset of stroke patients distinct from the one we addressed in this analysis. Furthermore, our data are in line with the findings of detrimental effect of aging on leptomeningeal collaterals in AIS23: given the robust association between age and severity of LA, collateral recruitment may well mediate the link between the two. Finally, the association between LAv and poor collaterals may further explain the predisposition for infarct growth in patients with greater LAv,12 ,13 and the opposite phenomenon of protection from infarct growth in patients with AIS and increased collateral circulation.16 ,24 LA may indeed be a marker for poor perfusion, affecting specifically the distal white matter regions. However, increased LAv does not appear to be a contraindication for treatment for AIS, as successful recanalization, starting with IV tPA, increases the chance of a good outcome in our analysis.
In our cohort, the significant predictors of good functional outcome were IV tPA use, recanalization, and presenting NIHSS. This is consistent with a number of other studies, showing that recanalization is a primary determinant in acute stroke outcome in IAT.9 ,21 Our TICI 2b recanalization rate of 43.8% was in line with those reported in the Interventional Management of Stroke-3 trials, and our cohort represents a similar era in reperfusion technology.2 Our study was not powered or directed to address the question of whether IAT provided additional benefit over IV tPA alone.
The significant predictors of death in this study were failed recanalization, increasing age, and antecedent use of hypoglycemic agents, with a cohort mortality rate of 27.5%. In this patient subset, the history of glucose lowering drug use was most likely a variable that identified the subset of diabetics with advanced disease; therefore, increased odds of mortality in this group is not unexpected. Advancing age and severe stroke have been previously linked to mortality,25 ,26 as was failure to recanalize.4 We propose that failure to recanalize is linked to mortality based on worse final stroke volume and symptoms after AIS. However, it is difficult to isolate the cause of mortality in AIS because of factors including goals of care, infectious and cardiac complications, and neurological complications related to the infarct.
In our sample, the time to intervention was a maximum of 6 h 6 min, with a mean of 2 h 46 min. Within the 6 h window, we found time to recanalization was not a significant predictor of outcomes. Time to intervention is traditionally linked to the degree of brain injury, causing a decreased likelihood of recovery and increased risk of hemorrhage. However, this is being challenged by the paradigm that a neurologic dysfunction may indicate ‘stunned’ but viable, as well as infarcted, tissue and that the progress of injury is heterogeneous.4 In a review of the MERCI and Multi-MERCI experiences, the time to reperfusion may not be a significant predictor, as long as it falls within an 8 h time window.5 Whether the time window can be extended further and the role of imaging in determining eligibility for IAT is the subject of ongoing studies.
Our study has several limitations, including those related to the retrospective study design. However, the neuroimaging assessment of LAv was done prospectively and in a blinded fashion to patient characteristics and outcomes, both clinical and radiographic. Secondly, subjects in our study were consecutive and selected for IAT based on an institutional protocol and presumed ‘likely to benefit’ from IAT. Given that the protocol criteria were developed based on the observational and prospective evidence historically available at the time of protocol implementation, the subject selection for IAT may differ from other sites. Nevertheless, this protocol allows for screening out high risk IAT candidates through a stringent selection process, excluding infarct volume >100 mL, and using NIHSS ≥8 as a substitute for a perfusion mismatch, assuming that a poor examination localizing to areas not yet infarcted on DWI is an indicator of salvageable tissue. Additionally, this protocol does not utilize LAv severity or age, as its surrogate marker, for patient selection. The strength of this study is in its systematic approach to ascertainment of the clinical and neuroimaging patient characteristics of the patient cohort, including the validated volumetric LA assessment method.
Conclusion
In AIS patients undergoing IAT, only recanalization and IV tPA were independently associated with good functional outcomes. Severity of LA was linked to poor collateral grade; however, increased LAv does not appear to be a contraindication for acute interventions in AIS.
References
Footnotes
-
Contributors D-VG, AJY, KF, ZC, LHS, TL-M, and NSR participated in gathering the data, and drafting and revising the manuscript. D-VG and NSR provided the data collection and statistical analysis. KF and NSR provided image analysis for leukoaraiosis. AJY, ZC, and TL-M collected the data from the intra-arterial therapy radiographic outcomes.
-
Funding This work was in part supported by NIH NINDS grants K23NS064052 and R01NS082285 (to NSR).
-
Competing interests NSR reports grants from NIH NINDS K23NS064052 and R01NS082285 during the conduct of the study, which also supported the work of KF for this manuscript. AJY reports grants from Penumbra Incand Remedy Pharmaceuticals during the conduct of the study. LHS reports personal fees from advising for stroke systems development for the Massachusetts Department of Public Health, outside the submitted work; serves as chair of AHA GWTG Stroke Clinical Workgroup (unpaid); as well as receiving support from NIH grant U10 NS08672901.
-
Ethics approval The study was approved by the local institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.