Article Text

Abstract
Introduction and purpose Symptomatic acute basilar thrombosis is associated with a high mortality rate. Aggressive endovascular management has led to survival rates of 35–50%. We report the largest series of endovascular reconstruction of occluded dominant vertebral arteries prior to basilar thrombectomy.
Materials and methods A prospective database since August 2010 of all neuroendovascular interventions was mined for patients undergoing basilar artery thrombolysis from which a group with vertebral artery reconstruction was selected. Patient charts were retrospectively reviewed for relevant clinical, technical, and outcome data.
Results From August 2010 to September 2012, six patients were identified who underwent vertebral reconstruction prior to basilar thrombectomy. Patients ranged in age from 42 to 57 years (mean 51 years). Mean time from symptoms until recanalization was approximately 6 h. Angiographic Thrombolysis in Cerebral Infarction IIB reconstitution of the basilar trunk was achieved in all cases. There were no technical complications. Two patients had care withdrawn secondary to massive completed brainstem infarction and poor neurological status post intervention. Three patients are now independent at 12, 14, and 31 months, respectively. One patient, after a follow-up of only 8 months, has achieved a modified Rankin Scale score of 3.
Conclusions Complete vertebral occlusion below a basilar thrombus can be recanalized prior to thrombectomy. In this case series, 100% of the acutely occluded vertebral arteries could be opened using either anterograde or retrograde access. However, basilar thrombosis continues to be a devastating illness, with one-third of the patients in this series dying of progressive infarction despite angiographic patency of the large conduit vessels with technical complications.
- Thrombectomy
- Thrombolysis
- Intervention
- Stroke
Statistics from Altmetric.com
Introduction
Acute basilar thrombosis is associated with >50% major morbidity and mortality, even with aggressive endovascular intervention.1–3 When attempting thrombectomy or thrombolysis of a basilar occlusion, vertebral occlusion can significantly limit the technical options. Dominant vertebral artery occlusion may result in a sub 3 mm artery for the neuroendovascular surgical procedure. With bilateral vertebral occlusion, the posterior communicating artery and pathways through external carotid collaterals are the only potential avenues for intervention. Both the sub 3 mm vertebral artery and the bilateral occlusion are poor choices for mechanical thrombectomy and leave intra-arterial thrombolysis as the only likely option. Although there are reports of both open surgical and endovascular recanalization of completely occluded vertebral arteries, there are no large case series.4–10 In addition, there are currently no publications in the context of basilar occlusion. This report marks the largest case series of recanalization to date for completely occluded vertebral arteries prior to basilar thrombectomy and thrombolysis.
Methods
After institutional review board approval for a minimal risk study, a prospective database from January 2010 to September of 2012 was reviewed for patients undergoing basilar thrombolysis, from which six patients were identified who required vertebral artery recanalization prior to basilar thrombectomy. Overall, during the study time period, 46 patients underwent intra-arterial stroke intervention. Of these 46 patients, 13 (27%) had intervention for acute vertebro-basilar insufficiency. All data were entered into an Excel spreadsheet for review. All images were reviewed for accuracy. Pubmed was reviewed for all published cases in the English language using the following key words: basilar thrombosis, basilar thrombolysis, basilar thrombectomy, vertebral artery occlusion, vertebral artery recanalization, and vertebral artery stenting. The articles were further reviewed to select those relevant to recanalization of completed occluded vertebral arteries. Although a number of different techniques and tools were used in this series, for patients undergoing stenting who are not already taking aspirin and clopidogrel, our protocol involves placement of a nasal/oral gastric tube and loading with 300 mg of clopidogrel and 650 mg of aspirin along with a 90 μg/kg eptifibatide bolus after stent deployment.
Results
The six patients had a mean age of 51 years (range 42–57). Mean time from presentation to recanalization ranged from 3 to 9 h (mean 5.8 h). Two of the patients received tissue plasminogen activator (tPA) according to standard guidelines prior to intra-arterial intervention. Three patients presented with coma. The National Institutes of Stroke Scale (NIHSS) score for the non-comatose patients ranged from 4 to 26 (mean 19). The Penumbra thrombectomy system was used in all cases. In conjunction with the Penumbra device (Penumbra Inc, Alameda, California, USA), Solitaire (Covidien Neurovascular, Irvine, California, USA), tPA, off-label stenting with Neuroform (Stryker Neurovascular, Freemont, California, USA), and the Merci retriever (Concentric, Mountain View, California, USA) were used in varying combinations in three patients (table 1). Once vertebral revascularization was achieved, a guide catheter was brought distal to the stent. Thrombolysis in Cerebral Infarction IIb recanalization of the basilar artery was achieved in all patients; however, some continued to have branch occlusions (table 1). Stents used to recanalize the occluded vertebral arteries included the Palmaz blue (Cordis, Miami, Florida, USA), Precise (Cordis), ION (Boston Scientific, Maple Grove, Minnesota, USA), Vision (Abbott Vascular, Abbott Park, Illinois, USA), and Zilver (Cook Medical, Bloomington, Indiana, USA). Two of the six patients died during their index hospitalization. Of the surviving patients, three are back to work, with modified Rankin Scale (MRS) scores of 1, 1, and 2, respectively. One patient continues to progress well at 8 months of follow-up with an MRS of 3. Follow-up ranged from 8 to 31 months (mean 16 months). MRS averaged 3 but for the four survivors, mean MRS was 2. There were no perforations, iatrogenic vessel dissections, or other technical complications.
Summary of patient demographics and indications
Case example 1
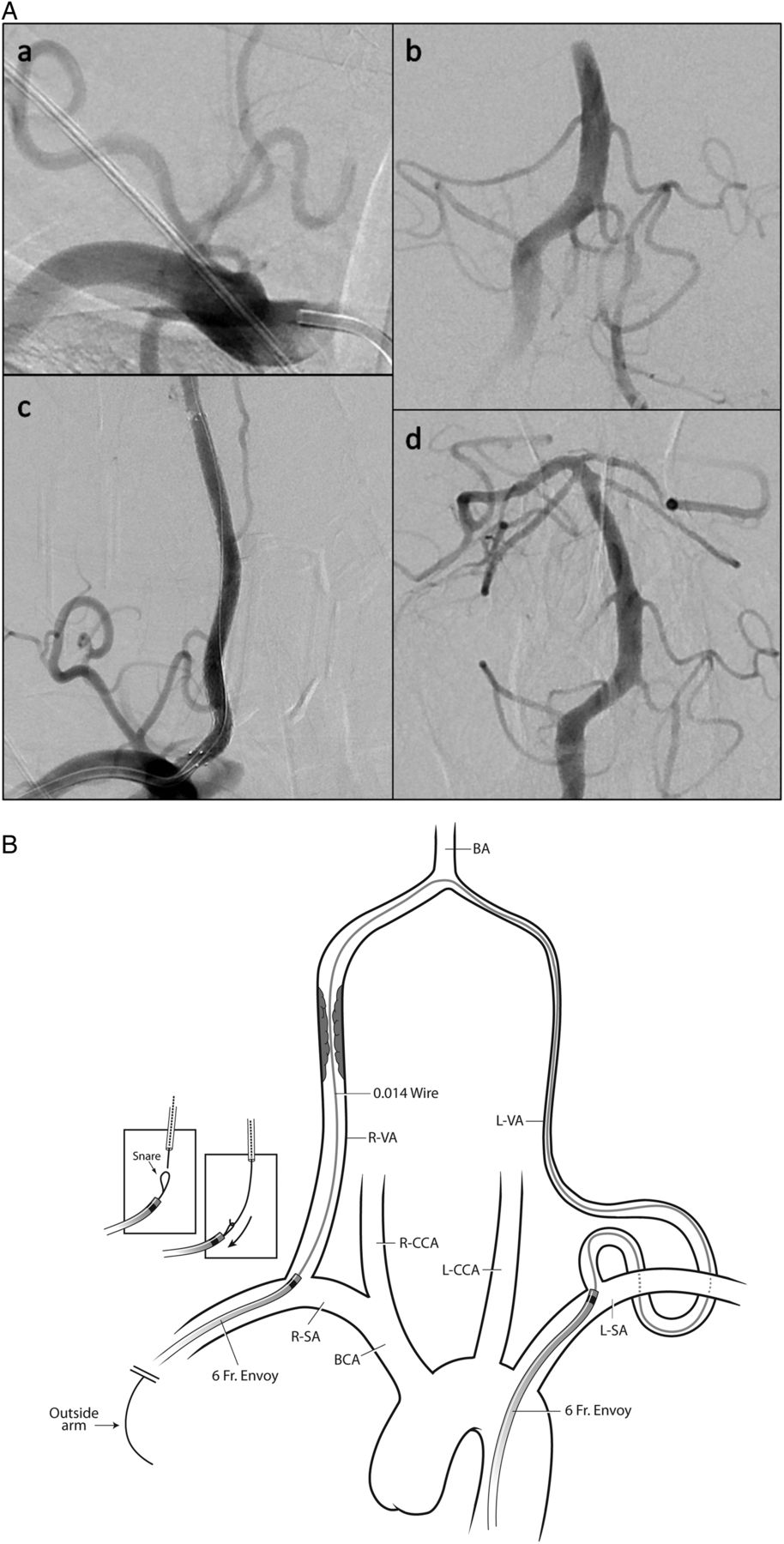
A 54-year-old right-handed patient with a 24 h history of intermittent double vision and vertigo was found on the ground hemiplegic and dysarthric on the morning of admission to the emergency room (figure 1). The patient progressed to being locked-in and was intubated in the emergency room. A CT scan without contrast demonstrated no acute infarct although the basilar artery appeared bright, suggesting a thrombus. Treatment with tPA was begun based on a time of onset of under 3 h from the time the patient was found down at home. CT angiography was obtained, demonstrating basilar thrombosis with a diminutive left vertebral artery with an origin stenosis and a right vertebral occlusion just above the origin. Based on the patient's clinical decline and in discussion with the patient's family, a decision was made to attempt a thrombectomy/lysis.

Case No 1. (A) (a) Dominant right vertebral occlusion below a basilar thrombosis. (b) ION stent 4×20 mm with reconstitution of the vertebral artery. (c) Basilar occlusion. (d) Post Penumbra thrombectomy and infusion of 2 units of alteplase with residual subclavian artery occlusion. (B) Anterograde crossing of a right vertebral occlusion. BA, basilar artery; R-VA, right vertebral artery.
A 6 Fr envoy (Cordis), hooked to a 10 000 unit heparin flush, was brought into the right subclavian artery (SCA) which confirmed the occlusion by angiography. An Excelsior 1018 microcatheter (Stryker Neurovascular), over a Synchro-14 (Boston Scientific, Freemont, California, USA), easily crossed the lesion and confirmed the patency of the V2/V3 segments without thrombus, and an ION 4×20 mm stent was deployed over the stenosis. At this point the patient was given an intra-arterial bolus of eptifibatide 90 μg/kg and loaded with aspirin 650 mg and clopidogrel 300 mg via an oral gastric tube. The Envoy was brought through the stent. The combination of suction thrombectomy with the 0.032 reperfusion catheter (Penumbra Inc) and 2 mg of intra-arterial tPA cleared the thrombus except for the right SCA in the ambient cistern that was not further treated. DynaCT demonstrated no hemorrhage. A post treatment MRI demonstrated scattered infarctions in the SCA distributions bilaterally and in the right pons. The patient progressed to ambulating with a walker prior to dismissal to rehabilitation.
Case example 2
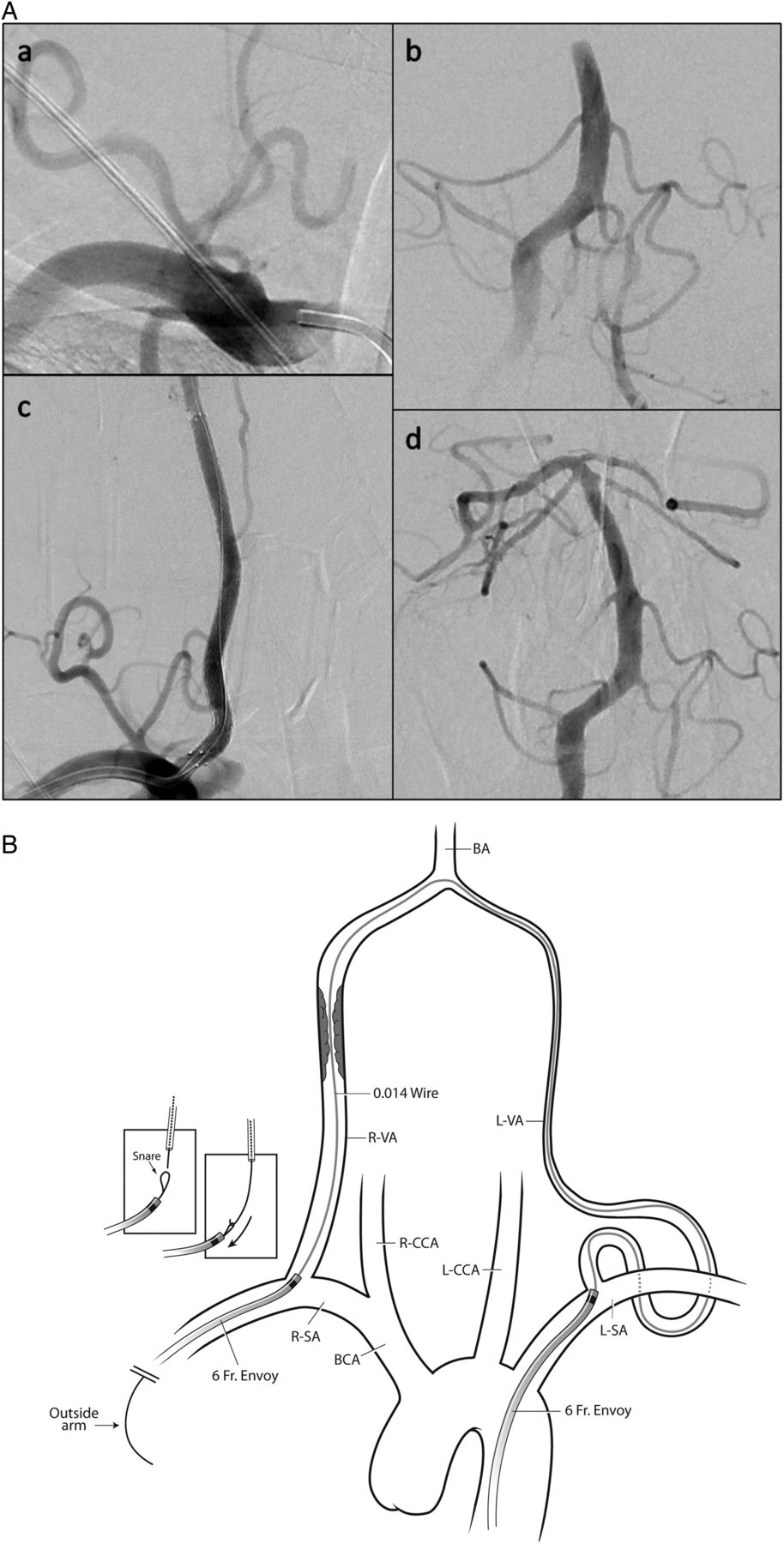
A 42-year-old comatose patient presented to our institution 6 h after initiation of a standard intravenous tPA for a basilar occlusion (Ofigure 2). A CT scan at our institution did not demonstrate hemorrhage or a large completed infarction and the patient was brought emergently to angiography. A 6 Fr 45 cm long sheath was placed and a 6 Fr Envoy was used to access the right SCA where the patient's dominant right vertebral artery was occluded. As the left vertebral artery was small and tortuous, it was not initially accessed. Attempts to access the right vertebral artery transfemorally failed and the right transbrachial artery was gained by a 6 Fr Envoy, which was placed just distal to the occluded vertebral origin. Attempts at direct anterograde transbrachial access to cross the occlusion failed. A Transcend 0.014 exchange length wire (Boston Scientific) with an SL10 catheter was brought over the vertebro-basilar confluens from the left vertebral artery into the right vertebral artery. The occlusion was crossed with some difficulty and the wire then snared out the arm. This was used as a rail for placement of a 6 mm × 80 mm Zilver nitinol stent in the V2 segment which was overlapped with a 6×30 mm Precise down the V1 origin. The overlap was dilated with a 6×20 mm balloon. The brachial Envoy was brought up to C2 and the Penumbra thrombectomy system was used to clear up to the basilar apex. A 4×20 mm Solitaire was then used to clear the right posterior cerebral artery. DynaCT demonstrated no hemorrhage, and post treatment MRI demonstrated right posterior cerebral and bilateral superior cerebellar infarcts. The patient regained consciousness with a mild left hemiparesis, walking with two assists prior to his dismissal to rehabilitation.
{kind=link}
{kind=link}
Case No 2. (A) (a) Right subclavian run demonstrating a vertebral stump that was impossible to cross from the femoral approach. (b) Basilar occlusion. (c) Reconstituted right vertebral artery through a retrograde brachial approach with 6×80 mm Zilver stent and 6×40 mm Precise. (d) Post thrombectomy with both the Penumbra and Solitaire. (B) Retrograde crossing of a right vertebral occlusion when anterograde crossing failed. BA, basilar artery; BCA, brachiocephalic artery; L-CCA, left common carotid artery; L-SA, left subclavian artery; L-VA, left vertebral artery; R-CCA, right common carotid artery; R-SA, right subclavian artery; R-VA, right vertebral artery.
Discussion
Occlusion of the posterior or vertebrobasilar arteries account for approximately 20% of all ischemic strokes, with acute basilar thrombosis being the most devastating ischemic syndrome.11 Early studies with intra-arterial urokinase in this setting resulted in significant morbidity and mortality, even with good angiographic outcome, while giving hope to untreated patients with 80% mortality.1–3 The BASilar artery International Cooperation Study (BASICS) trial has since examined the outcomes in larger groups of patients; however, the heterogeneity of treatment in this registry does not allow for clarity with regard to treatment although older age, greater than 6 h to treatment, and high NIHSS all likely impact outcome.12 ,13 As summarized in the online supplementary table S2, there are 12 case studies that document surgical or endovascular revascularization in the setting of symptomatic vertebral occlusion.4–10 14–16 In 2009, Kole et al followed the treatment of a 56-year-old patient suffering a stroke from complete vertebral artery occlusion.17 Intracranial angioplasty combined with Neuroform stent placement enabled revascularization for the patient. The authors concluded that angioplasty and stenting is an effective treatment for recanalization of occluded vertebral arteries. Similarly, Hassan et al8 documented a 70-year-old patient with acute vertebral artery occlusion and an NIHSS score of 16 on hospital admission. Emergency stenting of the patient's vertebrobasilar system led to successful revascularization. The study indicated that in this patient, stenting revascularized a completely occluded vertebral artery and led to a successful long term outcome. Noorian et al, Dubow et al, and Gupta et al all came to similar conclusions, that emergency stenting of occluded vertebral arteries can yield successful outcomes in certain patients.4 ,9 ,10
The largest clinical case series was conducted by Imai et al.14 The authors retrospectively reviewed the clinical outcomes of patients experiencing acute strokes in either the intracranial vertebral and/or basilar arteries in their large stroke series. Transluminal angioplasty and stenting was performed on 28 patients, of which 16 patients had complete occlusion of the vertebral arteries and 12 patients had severe stenosis of the vertebral arteries. Thirteen patients with occluded vertebral arteries had surgeries classified as ‘technically successful’ but ultimately only three patients were characterized as having a ‘favorable clinical outcome’. Most interestingly, many of these technically successful recanalizations were performed days after presentation. It is likely that the timing of intervention played a large role in the poor outcomes in this series. However, there are reports, such as those by Ogilvy et al, that have reported a patient stented for bilateral vertebral occlusion over a month from occlusion that after stenting had a meaningful clinical improvement.16 In a case series of four patients with symptomatic bilateral vertebral occlusion with only anterograde filling of the basilar artery, Tariq et al reported that all had recurrent events despite treatment with antiplatelet medication and/or anticoagulation.18
There are modern open surgical series of posterior circulation bypass for vertebrobasilar occlusion. Inoue et al detailed nine patients who suffered from acute vertebral artery occlusion and underwent surgical revascularization.7 Seven patients underwent technically successful recanalization, while the remaining two patients died due to irreversible brainstem infarction before surgery attributed to delay in surgery. The study indicated that surgical revascularization for vertebral artery occlusion was a feasible alternative for selected patients.
Chronic occlusions of over 3 months have also been recanalized. A study by Iwata et al reported the treatment of two patients with chronic vertebral artery occlusions (3 months or more) with stenting using the flow reversal technique.6
In this case series, technical recanalization of a dominant vertebral artery was performed without complication in six patients as a useful pathway for both mechanical thrombectomy and chemical thrombolysis in the setting of basilar thrombosis. Suction thrombectomy, stent retriever, Merci, and thrombolysis were all performed without technical complications. Preoperative imaging often demonstrated a ‘flow phenomena’ where the vertebral artery did not fill on CT angiography or MR angiography, but a stump was noted on cerebral angiography and the V2/V3 segments of the vertebral artery refluxed well from the posterior communicating or contralateral vertebral artery. In all patients, once the focal occlusion was stented, a patent path through the V2 and V3 segments was seen.
The major limitations of this study were its retrospective nature and the small patient numbers. However, the patient outcomes tracked favorably compared with historical norms and allowed for the use of all standard intra-arterial therapies in a patient population with a particularly poor prognosis without intervention.
Conclusions
Revascularization of a completely occluded dominant vertebral artery proximal to an occluded basilar artery can be successfully performed. Patients who otherwise would have had a poor choice of intra-arterial treatment options in this small case series tracked well compared with previously published outcomes.
Acknowledgments
The authors would like to thank Paul Dressel for the illustrations and Guissou Dabiri for her editorial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors All the authors contributed in parts to the data query and organization, literature search, and writing of this manuscript.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction