Article Text

Abstract
Background The outcome of acute ischaemic stroke due to tandem vertebrobasilar artery occlusion was poor. Endovascular revascularisation may be a positive approach for acute basilar artery occlusion combined with vertebral ostium stenosis or occlusion. We reported seven patients with acute vertebrobasilar tandem occlusion by using angioplasty or stenting for proximal lesion and thrombectomy for distal occlusion.
Materials and methods Consecutive patients with acute tandem vertebrobasilar artery occlusion at two centres were included in this study. We retrospectively analysed the clinical, technical and functional outcomes of the patients.
Results From March 2016 to March 2017, seven patients were included. The mean age and National Institute of Health Stroke Scale score at admission was 57 years and 22, respectively. A reverse approach was used in five patients. The Thrombolysis in Cerebral Infarction score 2b-3 was acquired in all patients. There were no procedural complications. The modified Rankin Scale score was 1–2 for three patients and 4 for one patient at 3 months. Three patients died at 3 months of follow-up.
Conclusions Endovascular revascularisation may be feasible for acute tandem vertebrobasilar artery occlusion, and more researches are needed.
- basilar artery
- occlusion
- stroke
- tandem occlusion
- thrombectomy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
In patients with isolated acute basilar artery (BA) occlusion, the use of modern thrombectomy devices for recanalisation was a better approach to improve recanalisation rates and clinical outcomes.1–3 At the same time, the clinical outcome of acute occlusion of the ostial vertebral artery (VA) concomitant occlusion of BA was generally extreme poor.4–6 The benefit of the second thrombectomy device has been verified in patients with acute tandem lesions in anterior circulation in Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE) and Revascularization with Solitaire FR device VS. Best Medical Therapy in the Treatment of Acute Stroke due to Anterior Circulation Large Vessel Occlusion Presenting within Eight hours of Symptom onset (REVASCAT) trials.7 8 However, the efficacy of these devices for patients with tandem vertebrobasilar arterial occlusion remains uncertain.
In this paper, we reported seven patients with acute vertebrobasilar artery tandem lesions treated with endovascular revascularisation techniques to achieve successful recanalisation.
Materials and methods
Patients
This is a retrospective study from two stroke centres in Beijing, China. The time interval of this study ranged from March 2016 to March 2017. The clinical data of patients undergoing endovascular revascularisation of acute vertebrobasilar artery tandem occlusion were collected and analysed. The local ethics committee approved the study and informed consent of the patient was obtained.
Endovascular treatment procedure
The procedure of endovascular treatment was performed under general anaesthesia in all patients. A 6 Fr guiding catheter was placed at the proximal subclavian artery. The procedure was performed in all patients using the endovascular revascularisation approach through the occlusive or stenotic vertebral artery (dirty-road path). The microguidewire crossed the lesion of VA occlusion or stenosis. Predilation of the VA lesion was performed using a small balloon and then digital subtraction angiography (DSA) was performed to understand the diameter of the VA. Then reverse approach (mechanical thrombectomy of BA occlusion followed by proximal VA stenting angioplasty) or antegrade approach (proximal VA stenting angioplasty followed by mechanical thrombectomy of BA occlusion) was used to perform endovascular treatment.4 Before stent implantation, 300 mg aspirin and 300 mg clopidogrel were given via a nasal gastric tube immediately. Then tirofiban (glycoprotein IIb/IIIa inhibitor) was given according to the operator’s discretion. Final angiography was performed to exclude reocclusion or thrombosis in the stent after the stent was deployed for 10–20 min. Patients received double antiplatelet agents for 3 months, and then aspirin or clopidogrel was continued alone.
Reverse technique
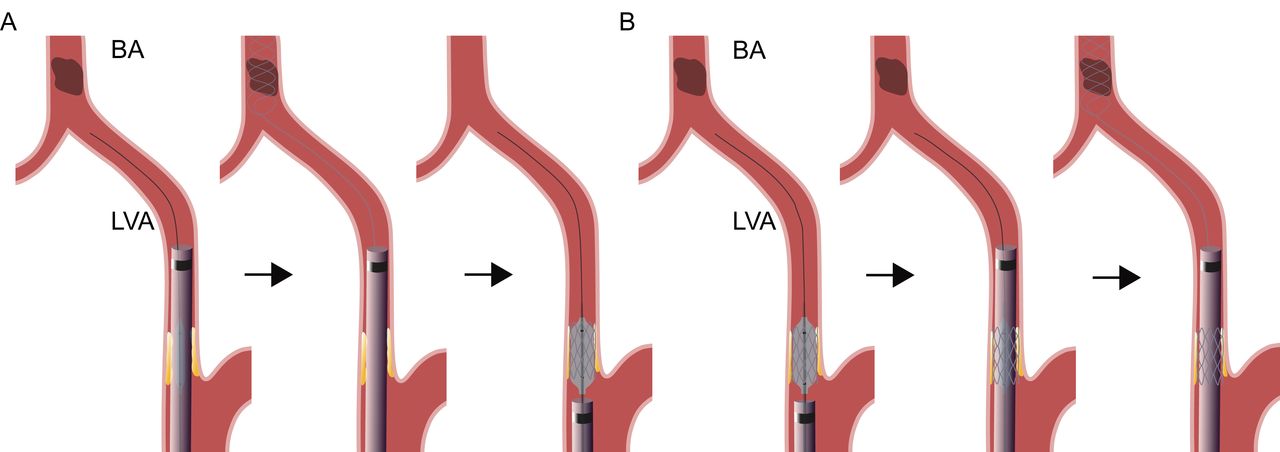
The guiding catheter was then sent to distal of V2 segment through the stenosis segment over the partially reinflated balloon (similar to the triaxial system) under the road map. The microcatheter was then advanced to the distal BA or the largest posterior cerebral artery across the BA occlusion over a microguidewire. Then angiography was performed through the microcatheter to identify the distal thrombus. A stent retriever was deployed at the segment of the BA occlusion through the microcatheter. The stent retriever was unsheathed to fully expand through the clot for 3–7 min. Subsequently, the stent retriever was gently pulled back with aspiration through the guiding catheter. If recanalisation was insufficient, further procedure would be attempted to achieve successful reperfusion of the BA. Thrombolysis in Cerebral Infarction (TICI) 2b-3 was defined as successful recanalisation after mechanical thrombectomy. After successful recanalisation was achieved, the microguidewire was sent to the V2 segment and then the guiding catheter was gently pulled back to the proximal subclavian artery. A balloon-expandable stent was then implanted at the ostial vertebral artery over the microguidewire (figure 1A).

Illustration of the reverse (A) and the antegrade (B) technique for the tandem vertebrobasilar artery occlusion through the occlusive or severe stenotic vertebral artery (dirty-road path). (A) A guiding catheter was advanced to the distal left vertebral artery (LVA) V2 segment through the stenosis segment over the partially reinflated balloon. A stent retriever was deployed at the segment of the basilar artery (BA). After successful recanalisation was achieved, the microguidewire was sent to the V2 segment and then the guiding catheter was gently pulled back to the proximal subclavian artery. A balloon-expandable stent was then implanted at the ostial vertebral artery. (B) A balloon-expandable stent was sent to the ostial vertebral artery over the microguidewire and was implanted at the lesion exactly. The guiding catheter was then navigated to the distal V2 segment through the partially reinflated balloon across the implanted stent gently. Subsequently, the stent-assisted thrombectomy was performed as described above.
Antegrade technique
A balloon-expandable stent was sent to the ostial vertebral artery over the microguidewire and was implanted at the lesion exactly. The guiding catheter was then navigated to the distal V2 segment through the partially reinflated balloon across the implanted stent gently. Subsequently, the stent-assisted thrombectomy was performed as described above (figure 1B).
Results
Seven patients were identified to have acute tandem vertebrobasilar artery occlusions (seven men, mean age 57 years, range 48–66). Mean National Institute of Health Stroke Scale (NIHSS) score at admission was 22 (range 12–28). One patient received tissue plasminogen activator prior to endovascular treatment.
The reverse approach was used in five patients, while antegrade approach was used in two patients. TICI score 2b-3 was acquired in all patients. There were no technical complications. The modified Rankin Scale (mRS) score was 1–2 for three patients and 4 for one patient at 3 months. Three patients died at 3 months of follow-up. The clinical data, treatment strategy and patient clinical outcomes are presented in table 1.
Summary of patient clinical data
Case example 1
A 57-year-old patient with a history of coronary heart disease and diabetes mellitus was transferred to our emergency room due to quadriplegia. The NIHSS score was 12 and posterior circulation Acute Stroke Prognosis Early CT Score (ASPECTS) on diffusion-weighted imaging (DWI) was 8. DWI showed pontine infarction, and MRA revealed BA occlusion. The time from the onset to femoral artery puncture was 402 min.
Cerebral DSA showed the left dominant VA and BA tandem occlusion (figure 2A, D) and the right contralateral non-dominant VA ending in the posterior inferior cerebellar artery (figure 2C). So the left occlusive VA (dirty-road path) was the only access to perform mechanical thrombectomy for BA occlusion.

Case example 1. (A) Left vertebral artery occlusion. (B) A 6 Fr catheter crossing the left vertebral artery through the stent over the partially reinflated balloon. (C) Right non-dominant ending in posterior inferior cerebellar artery. (D) Basilar artery occlusion. (E) Recanalisation of the basilar artery. (F) Final angiography of the left vertebral artery.
A 6 Fr Envoy guiding catheter (Cordis, Miami Lakes, Florida, USA) was placed at the proximal subclavian artery, and the Transcend microguidewire (Boston Scientific, Freemont, California, USA) crossed the lesion of the VA occlusion. Predilation of the VA ostial occlusion was performed using a 2 mm x 15 mm balloon (Boston Scientific), and then the balloon was exchanged with a 4 mm x 18 mm balloon-expandable Apollo stent (MicroPort, Shanghai, China). After the stent was placed, the balloon of the stent was partially reinflated and the 6 Fr guiding catheter was advanced into V2 segment through the stent over the partially reinflated balloon (figure 2B). A microcatheter (Stryker Neurovascular, Freemont, California, USA) was placed at the right posterior cerebral artery over the microguidewire, and then a Trevo stentriever (Stryker Neurovascular) was used to perform mechanical thrombectomy. Follow-up angiography showed complete BA reperfusion (figure 2E) and the final status of the left ostium VA stent (figure 2F). The time from femoral puncture to reperfusion was 90 min. Follow-up CT scan revealed no cerebral haemorrhagic transformation. The mRS was 1 at 3 months.
Case example 2
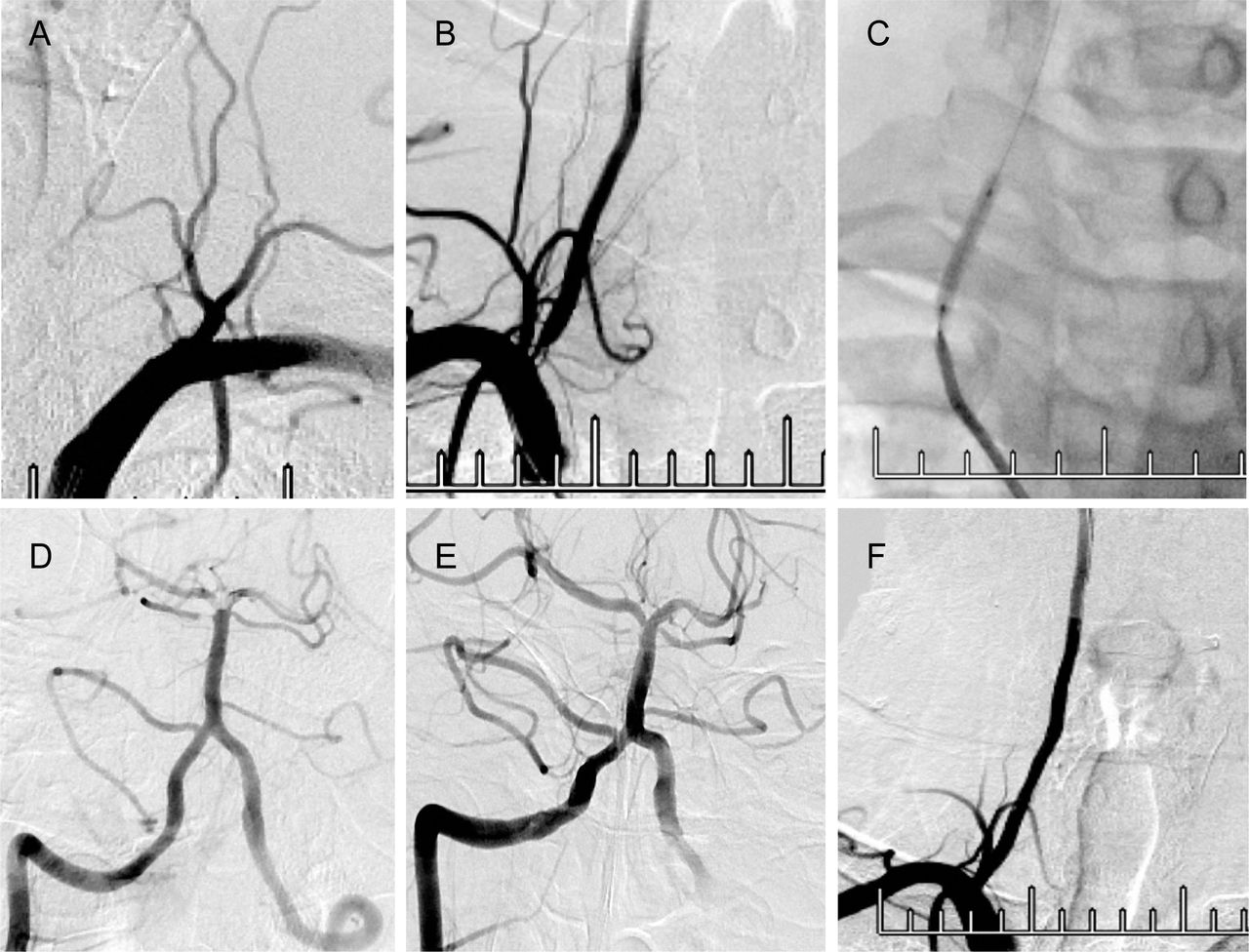
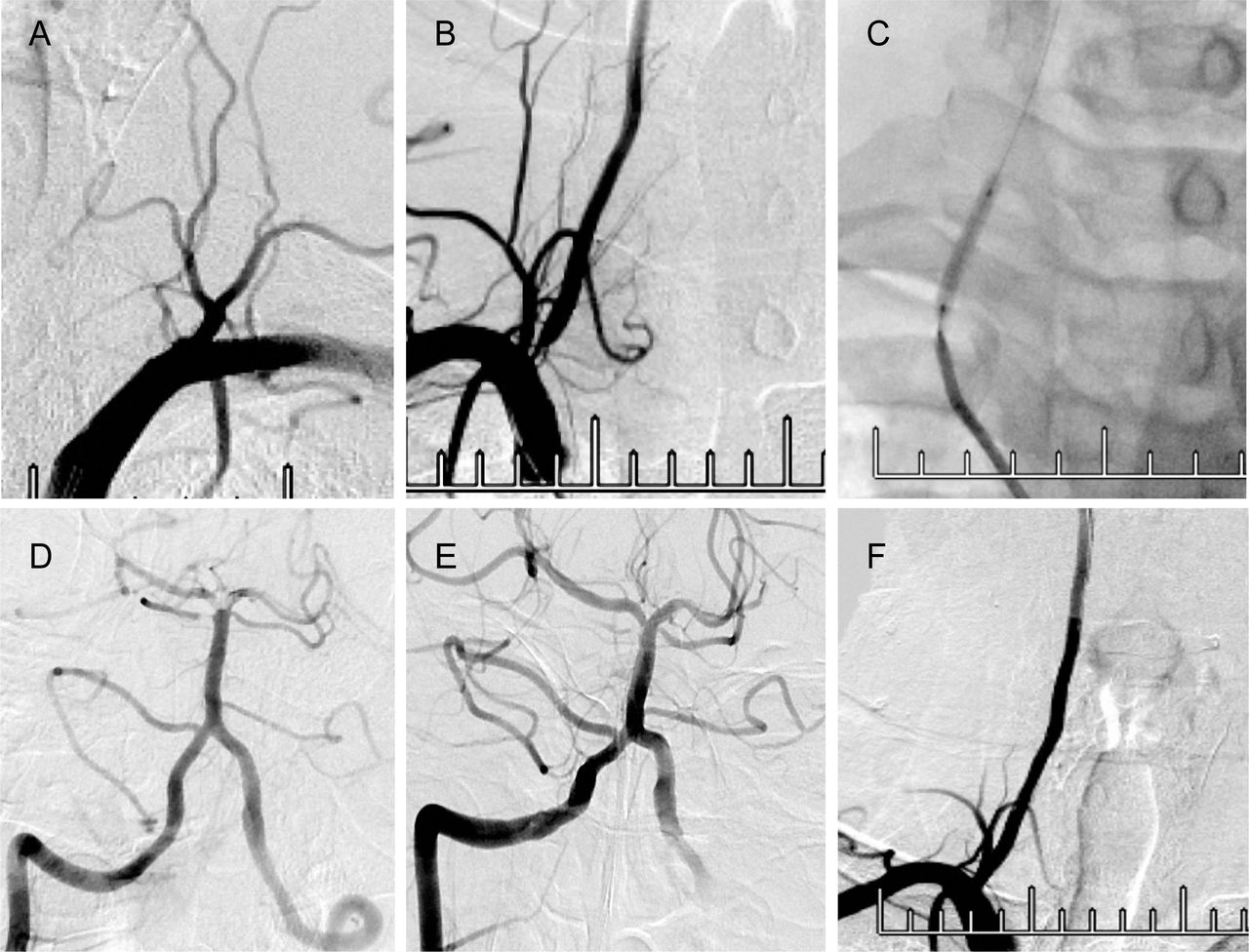
A 58-year-old patient with a history of diabetes mellitus and hypertension was transferred to our hospital due to vertigo and consciousness disturbance. The time from onset to femoral artery puncture was 855 min, and the NIHSS score was 16. The posterior circulation ASPECTS on DWI was 7 and MRA showed distal BA occlusion.
Cerebral DSA showed left VA ostium occlusion (figure 3A), right vertebral artery ostium severe stenosis (figure 3B) and distal BA clot. A 6 Fr guiding catheter (Cordis) was placed at the right subclavian artery and a microguidewire (Abbott, USA) crossed the stenosis segment to the V2 segment. Predilation was performed using a 3.0×20 mm balloon (Boston Scientific) (figure 3C). The guiding catheter was sent to V2 segment through the stenosis segment over the partially reinflated balloon. Angiography showed that the distal BA occluded (figure 3D). A 4 mm x 20 mm Solitaire stentriever (Irvine, California, USA) was used to perform mechanical thrombectomy. Follow-up angiography showed successful recanalisation of the distal BA occlusion (figure 3E). A 4 mm x 15 mm balloon-expandable stent (Boston Scientific) was implanted at the right vertebral artery stenosis (figure 3F). The time from puncture to recanalisation was 77 min. Follow-up CT scan showed no cerebral haemorrhage. The mRS was 2 at 3 months.
{kind=link}
{kind=link}
{kind=link}
Case example 2. (A) Left vertebral artery occlusion. (B) Right vertebral artery ostial severe stenosis. (C) Predilation of the right vertebral artery stenosis. (D) Distal basilar artery clot. (E) Recanalisation of the basilar artery. (F) A stent-assisted angioplasty at the right vertebral artery.
Discussion
In this case series, we reported the endovascular revascularisation for the acute tandem occlusion of vertebrobasilar artery through the occlusive or stenotic road path (dirty-road path).
Ecker et al 6 reported six patients with acute vertebral occlusion below a basilar thrombus were treated with endovascular reconstruction of VA occlusion prior to basilar thrombectomy, and one-third of the patients died due to progressive infarction.
Cohen et al 4 detailed seven patients who suffered from acute tandem vertebrobasilar occlusion and underwent emergent endovascular revascularisation, and two patients died. Though the device and approach for endovascular revascularisation were different, the clinical outcome was similar.
It was more complicated and difficult to perform endovascular revascularisation in the patients with acute tandem vertebrobasilar occlusion than that in the patients with an isolated acute BA occlusion. Generally, in tandem vertebrobasilar artery occlusion, the contralateral VA (clean-road path) was the priority access to perform mechanical thrombectomy of the BA occlusion.4 Cohen et al 4 reported only two patients who underwent thrombectomy through the clean-road path.
In this case series, the contralateral VA of five patients was non-dominant artery and another two patients’ contralateral dominant VA was severe stenosis. So endovascular revascularisation was performed through the occlusive VA in five patients and the contralateral stenotic VA in another two patients.
There was usually no need for the predilation of the senotic VA prior to implanting the stent for reducing the risk of artery embolism.4 9 However, in the case of VA occlusion or extremely severe stenosis, we predilate the lesions with a small balloon, and then angiography was performed to understand the extent and width of the VA before the stent was implanted.
Cohen et al 4 described two techniques (antegrade technique and reverse technique) that were used to perform endovascular revascularisation when the access was dirty-road path. In Cohen et al’s report, five patients underwent endovascular recanalisation through occlusive VA; reverse technique was used for four patients and anterograde technique was used for one patient. They thought there were risks of delaying reperfusion, stent slipping towards the subclavian artery and increasing the difficulty to advance the guiding catheter through the stent.4
However, for the reverse technique, the guiding catheter could not cross the occlusion of VA with severe residual stenosis after primary VA angioplasty or the blood flow was very slow when the guiding catheter advanced into the V2 segment. Finally, there was the risk of re-embolisation when the stent of the ostial VA was implanted.9 In this case series, antegrade technique was used for two patients without stent slipping and deformation; reverse technique was used for five patients without re-embolisation.
For antegrade strategy, how to deliver the guiding catheter to V2 segment through the stent was a technological challenge. A partially reinflated balloon within the stent can help deliver the guiding catheter to the VA.9 In this procedure, the guiding catheter passed through the stent over a partially reinflated balloon when we used the antegrade technique. Because each of these methods has its advantages and disadvantages, it needs careful consideration to choose antegrade or reverse revascularisation technique.
The limitations of this study were the small number of patients, retrospective analysis and selection bias. In addition, this study was not a randomised controlled design. The long-term outcomes of these patients were uncertain.
Conclusions
In this case series, endovascular revascularisation of acute vertebrobasilar artery tandem occlusion through dirty-road path can be performed successfully without technical complications and may be feasible, while more studies are needed.
Footnotes
Contributors All authors provided substantial contributions to the conception and design of the study and drafted the work or revised it and provided the final approval of the manuscript for submission. All authors are agreeable to be accountable for all aspects of the work, including its accuracy or integrity.
Funding This work was supported by the National Natural Science Foundation of China (Contract grant number: 81471390 to N.M., 81371290 to Z.R.M.), Beijing High-level Personnel Funds (Contract grant number: 2013-2-19 to Z.R.M.).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Tiantan Hospital, Capital Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.