Article Text

Abstract
The benefits and safety of intravenous recombinant tissue plasminogen activator (IV-tPA) for patients with mild ischaemic stroke (MIS) are still unclear. The objective of this meta-analysis was to evaluate the efficacy and safety of IV-tPA as treatment for patients with MIS. We performed a systematic literature search across MEDLINE, Embase, Central, Global Health and Cumulative Index to Nursing and Allied Health Literature (CINAHL) , from inception to 10 November 2016, to identify all related studies. Where possible, data were pooled for meta-analysis with odds ratio (OR) and corresponding 95% confidence interval (CI) using the fixed-effects model. MIS was defined as having National Institutes of Health Stroke Scale score of ≤6. We included seven studies with a total of 1591 patients based on the prespecified inclusion and exclusion criteria. The meta-analysis indicated a high odds of excellent functional outcome based on the modified Rankin Scale or Oxfordshire Handicap Score 0–1 (OR=1.43; 95% CI 1.14 to 1.79; P=0.002, I2=35%) in patients treated with IV-tPA compared with those not treated with IV-tPA (74.8% vs 67.6%). There was a high risk of symptomatic intracranial haemorrhage (sICH) with IV-tPA treatment (OR=10.13; 95% CI 1.93 to 53.02; P=0.006, I2=0%) (1.9% vs 0.0%) but not mortality (OR=0.78; 95% CI 0.43 to 1.43; P=0.43, I2=0%) (2.4% vs 2.9%). Treatment with IV-tPA was associated with better functional outcome but not mortality among patients with MIS, although there was an increased risk of sICH. Randomised trials are warranted to confirm these findings.
- mild ischemic stroke
- thrombolysis
- efficacy
- safety
- meta-analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Intravenous administration of recombinant tissue plasminogen activator (IV-tPA) remains the only Food and Drug Administration-approved thrombolysis therapy for patients with acute ischaemic stroke within 4.5 hours after symptom onset. Mild ischaemic stroke (MIS) is common1–3 and is associated with disability.4–6 However, whether patients with MIS can benefit from IV-tPA treatment remains unclear. The latest American Heart Association/American Stroke Association guidelines recommend that IV-tPA treatment may be considered for patients with MIS (class IIb; level of evidence C)7; however, no recommendations were found in European, Japan and Canadian guidelines.8–10
Existing literature exploring the use of thrombolysis in MIS is controversial.11–22 Some studies have shown IV-tPA treatment is associated with excellent outcome,11–17while other studies found no benefit from IV-tPA therapy.18–22 These inconsistent results may be due to differences in sample size, study design, study population or confounding among studies. Three meta-analyses published in 2014 had investigated IV-tPA treatment in patients with MIS.15 17 22 However, in these analyses, a limited number of studies were included, the risk of symptomatic intracranial haemorrhage (sICH) was not compared, and the results were conflicting. Hence, we systematically evaluated currently available studies to evaluate the efficacy and safety of IV-tPA treatment in patients with MIS.
Methods
Databases and sources
We identified all published studies assessing the efficacy and safety of thrombolysis for mild stroke using MEDLINE, Embase, Central, Global Health and Cumulative Index to Nursing and Allied Health Literature (CINAHL). The search terms were ‘mild OR minor OR mini OR warning’ AND ‘stroke OR cerebrovascular disease’ AND ‘thrombolysis OR thrombolytic OR alteplase OR rtPA OR urokinase’; a comprehensive search strategy can be found in the online supplementary file. The search strategy was developed without any language restriction.
Supplementary file 1
Study selection
Two reviewers (SY and AS) performed the study selection independently, with disagreements resolved through discussions and by consulting a third reviewer (XW), if necessary. Studies were considered potentially eligible for this systematic review if they met the following inclusion criteria: (1) diagnostic criteria for MIS (National Institutes of Health Stroke Scale (NIHSS) score of ≤6); (2) the study recorded baseline characteristics information, including study type, first author(s), study locations, study period, numbers of total and subgroup subjects, mean age, proportion of male subjects and NIHSS; (3) the study compared the efficacy and safety of patients with MIS treated with IV-tPA and those not treated with IV-tPA; (4) sufficient data of excellent functional outcome (modified Rankin Scale (mRS) 0–1 or Oxfordshire Handicap Score (OHS) 0–1), sICH and mortality at 3 or 6 months were provided; and (5) onset to needle time was ≤4.5 hours. The following were the exclusion criteria: (1) no comparison group, (2) excellent outcome on hospital discharge, (3) reviews and commentary papers, and (4) studies reporting incomplete data for mentioned subgroups and unavailable data even after exploring the online supplementary materials or contacting the authors.
Data extraction
Two reviewers (SY and AS) independently extracted the data and compared the results. The characteristics of studies and patients, the diagnostic criteria for MIS, the time from onset to treatment, and the primary outcome (excellent functional outcome defined as mRS 0–1 or OHS 0–1 at 3 or 6 months) and secondary outcomes (incidence of sICH and mortality at 3 or 6 months) were extracted. We contacted the authors to obtain further data for one study.11
Quality assessment
The quality of study was assessed using the Newcastle-Ottawa Quality Assessment Scale for cohort studies.23 This scale, recommended by the Cochrane Non-Randomized Studies Methods Working Group, is composed of eight items that assess patient selection, study comparability and outcome. Two investigators (SY and WT) performed quality assessment independently, and disagreements were resolved by XW (online supplementary table 1).
Data synthesis and analysis
We evaluated the heterogeneity among included studies using the I2test. In the present study, I2 values exceeding 50% were considered as an indicator of significant heterogeneity. Fixed-effect models were used to estimate the odds ratio(OR) and 95% confidence interval(CI) if heterogeneity is <50%; otherwise, random-effect model was used. Begg’s funnel plot was used to assess the potential for publication bias. We considered P values less than 0.05 to be statistically significant. We conducted the meta-analysis using the Cochrane RevMan V.5.3 software and Meta-Analyst (V.3.13beta; Tufts Medical Center).24
Results
Characteristics of included studies
Among 3818 references obtained by our search strategy, 7 studies (1591 patients) satisfied the eligibility criteria and were included in the final analyses (figure 1). These included five prospective cohort studies and two post-hoc analyses from large clinical trials. The IV-tPA treatment group consisted of 801 patients and the non-treatment group included 790 patients. The baseline characteristics of the included studies are shown in table 1. The mean age of participants ranged from 66 to 82 years, and the mean baseline NIHSS score ranged from 2 to 4. The onset to treatment time was recorded in all the studies as less than or equal to 4.5 hours.

Flow chart of literature screening and selection process. tPA, tissue plasminogen activator.
Characteristics of studies included in the review
ICH, intracranial haemorrhage; mRS, modified Rankin Scale; NA,no data available; NIHSS, National Institutes of Health Stroke Scale; OHS, Oxfordshire Handicap Score; sICH, symptomatic intracranial haemorrhage.
Excellent functional outcome
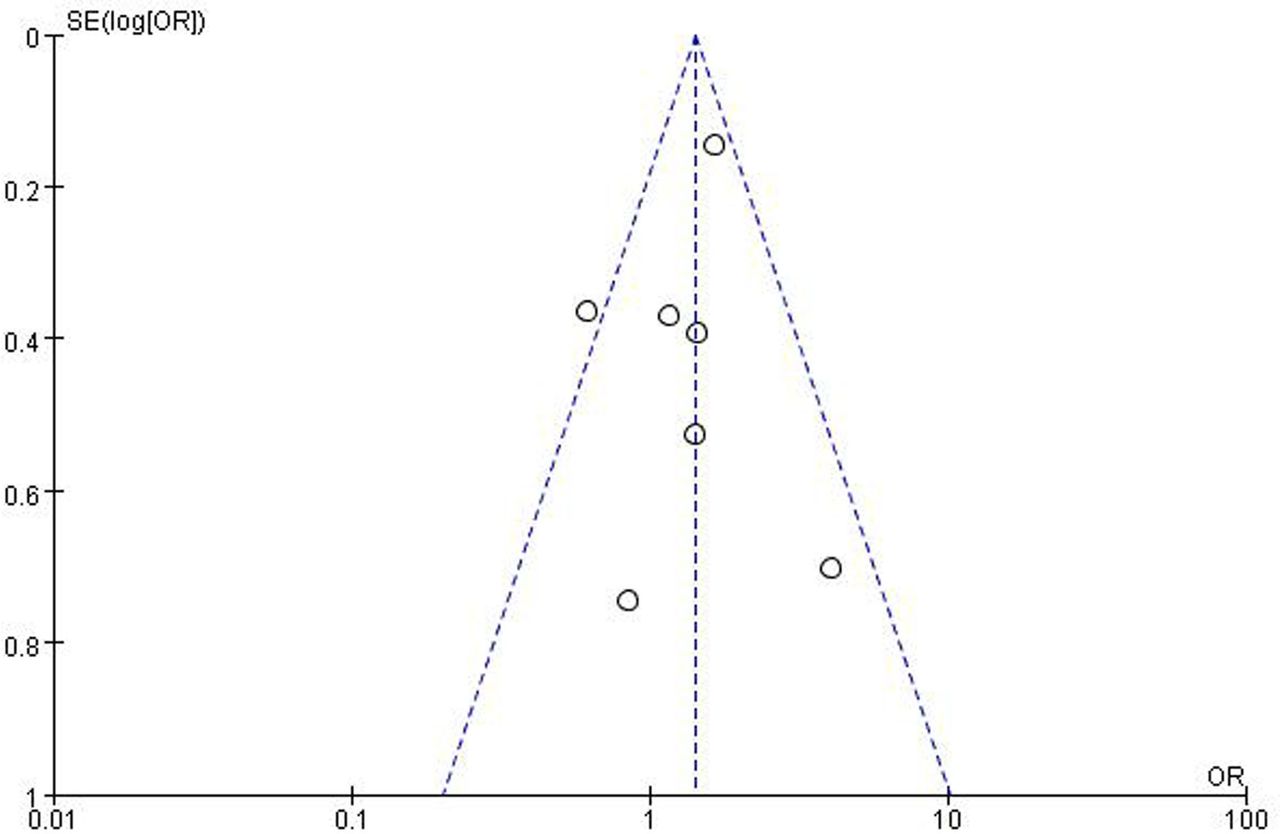
All of the included studies report the percentage of mRS 0–1 or OHS 0–1 at 3 or 6 months. There are 599 (74.8%) patients with excellent functional outcome among 801 patients treated with IV-tPA and 534 (67.6%) patients in the control group without IV-tPA treatment. The meta-analysis indicated a high odds of excellent outcome (OR=1.43; 95% CI 1.14 to 1.79; P=0.002, I2=35%) in patients with MIS treated with IV-tPA compared with those without IV-tPA treatment (figure 2), and no publication bias was observed through the Begg’s funnel plot (figure 3).
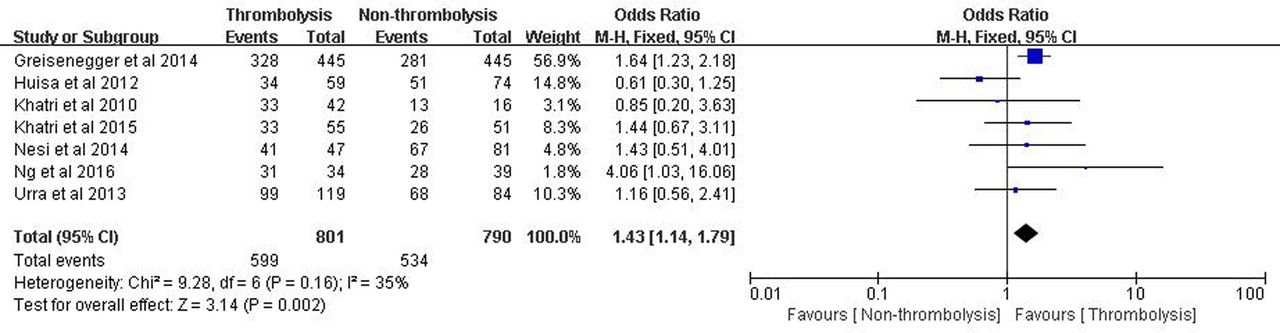
Forest plot for excellent outcome of IV-tPA-treated MIS compared with those without IV-tPA treatment. IV-tPA, intravenous recombinant tissue plasminogen activator; M-H, Mantel-Haenszel; MIS, mild ischaemic stroke.

Funnel plot for publication bias for excellent outcome of intravenous recombinant tissue plasminogen activator-treated mild ischaemic stroke.
Safety outcome
All of the included studies reported on sICH in both comparison groups. In three studies, 15 (1.9%) patients treated with IV-tPA developed sICH, while no sICH was found in the non-treatment group. The meta-analysis demonstrated a significantly higher odds of sICH (OR=10.13; 95% CI 1.93 to 53.02; P=0.006, I2=0%) in patients treated with IV-tPA in comparison with those without IV-tPA treatment (figure 4). Only three studies reported sICH and the publication bias was not observed through Begg’s funnel plot (online supplementary figure 1).

Forest plot for symptomatic intracranial haemorrhage of IV-tPA-treated mild ischaemic stroke compared with those without IV-tPA treatment. IV-tPA, intravenous recombinant tissue plasminogen activator; M-H, Mantel-Haenszel.
Mortality in patients treated with IV-tPA was 2.4% (n=19), compared with 2.9% (n=23) in the non-treatment group. The meta-analysis did not identify a significant difference in the odds of mortality (OR=0.78; 95% CI 0.43 to 1.43; P=0.43, I2=0%) between the two groups (figure 5). No publication bias was observed through Begg’s funnel plot (online supplementary figure 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for mortality of IV-tPA-treated mild ischaemic stroke compared with those without IV-tPA treatment. IV-tPA, intravenous recombinant tissue plasminogen activator; M-H, Mantel-Haenszel .
Discussion
The current meta-analysis of the seven included studies found that IV-tPA was associated with excellent functional outcomes at 3 or 6 months following MIS with significantly increased risk of sICH. No significant difference was observed in mortality between patients receiving and not receiving IV-tPA therapy.
MIS is common; about half of ischaemic strokes in the USA1 and approximately 30% new ischaemic strokes in China are MIS.2 3 MIS is also associated with significant disability and poor functional outcomes.4–6 Previous investigations have found that 28.3% of patients were not discharged home following MIS,4 and 29.0% of them had significant functional disability at 3 months (mRS ≥2),6 which may be due to intracranial occlusion, lacunar progression and stroke recurrence.5 25–27 Currently, approximately 29%–32% of patients with MIS are excluded from IV-tPA therapy due to concerns about sICH.4 28 However, given the considerable long-term morbidity associated with MIS, the role of IV-tPA therapy needed to be closely assessed.
Existing literature regarding the efficacy of IV-tPA therapy in MIS were conflicting.11–22 Our meta-analysis suggests that patients treated with IV-tPA were more likely to have excellent functional outcome compared with the non-treatment group, which confirms findings of previous meta-analyses from randomised trials.17 In this meta-analysis, 237 (67.8%) patients with MIS (NIHSS ≤5) in the IV-tPA group and 189 (58.9%) patients in the control group showed excellent outcome at 3–6 months, and IV-tPA treatment was associated with a 1.48-fold increase in the odds of excellent outcome.17 Different baseline characteristics, including baseline NIHSS score and onset to needle time, may have been the underlying reasons for the no benefit found in patients with MIS treated with IV-tPA in some studies. The Huisa et al 18 study indicated that patients with MIS treated with IV-tPA had similar outcomes as patients not receiving IV-tPA treatment. In this study, the mean baseline NIHSS score was 3.4 in patients treated with IV-tPA and significantly higher than untreated patients (the mean baseline NIHSS score is 1.9).18 Data from the main paper of the Third International Stroke Trial-3, in which the onset to needle time in some patients is more than 4.5 hours, suggested IV-tPA treatment had no benefits for patients with MIS.29 However, if restricted patients met the standard treatment criteria, including randomisation within 3 hours, IV-tPA treatment has a significant benefit for patients with MIS.14
The risk of haemorrhage is one of the major reasons that patients with MIS are excluded from IV-tPA treatment. In our meta-analysis, 15 (1.9%) patients developed sICH, and all of these patients received IV-tPA therapy. Our results were in line with previous studies5 30 31 showing that the risk of sICH was low for patients with MIS treated with IV-tPA, although higher in comparison with the non-treatment group. A meta-analysis of 12 trials reported that the risk of sICH in all patients with stroke was 7.7%.30 The incidence of sICH based on stroke severity was compared in a cohort study that found the risk of haemorrhage was about 2% in patients with MIS and 8.1% in patients with a baseline NIHSS score of more than 6.31 Moreover, we found that in all 15 patients with sICH reported in three studies, defined as any ICH with NIHSS score increase of ≥1,11 18 21 haemorrhage was not serious and may not be associated with disability and mortality. The mortality rate of IV-tPA-treated patients (2.4%) and non-tPA-treated patients (2.9%) was similar, which suggested IV-tPA treatment did not affect mortality. Our meta-analysis, along with previous studies, suggests the overall risk of sICH is low and does not contribute to disability or mortality in patients with MIS treated with IV-tPA. The results of our meta-analysis support the need for ongoing randomised trials to further investigate the role of IV-tPA therapy in MIS. The TNK–Tissue-Type Plasminogen Activator Evaluation for Minor Ischemic Stroke With Proven Occlusion-2 (TEMPO-2) and A Study of the Efficacy and Safety of Activase (Alteplase) in Patients With Mild Stroke (PRISMS) are two ongoing randomised, placebo-controlled trials evaluating the efficacy, and particularly the safety, of IV-tPA or Tenecteplase -tissue-type plasminogen activator in patients with MIS (http://clinicaltrials.gov/).
There were some limitations to our meta-analysis. First, most of the studies included fairly small number of subjects, together with potential bias arising from the non-randomised nature of observational studies. This bias could not be compensated for satisfactorily, and the unadjusted results from observational studies remain less conclusive even when the data from post-hoc analyses of large randomised controlled trial are combined. Second, we could not report the results based on adjusted OR as four of the included studies did not report these data. Third, the definition of sICH was different among included studies.
Conclusion
In conclusion, our meta-analysis found that patients with MIS treated with IV-tPA had improved functional outcome compared with patients without IV-tPA treatment. Although IV-tPA treatment increased the risk of sICH, this risk is low and did not affect mortality. Our results suggest IV-tPA treatment is beneficial and relatively safe in patients with MIS, and there is a need for further randomised clinical trials to confirm these findings.
References
Footnotes
Contributors YC, XW and C-FL conceived this meta-analysis and revised the manuscript. XW searched the database. SY and AS collected and extracted the data. SY and WT conducted statistical analysis. SY and QH drafted this manuscript.
Funding This work was supported in part by grants from the National Natural Science Foundation of China (81471195), Suzhou Clinical Research Center of Neurological Disease (Szzx201503) and Jiangsu Provincial Medical Key Discipline Project, The Second Affiliated Hospital of Soochow University Preponderant Clinic Discipline Group Project Funding (XKQ2015002). This was also partly supported by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Presented at Part of this article was presented at the Asia Pacific Stroke Conference 2017 (Cerebrovasc Dis 2017;44(suppl 1):1–52).