- Le-Bao Yu1,2,3,4,
- Wei Yan5,
- Qian Zhang1,2,3,4,
- Ji-Zong Zhao1,2,3,4,
- Yan Zhang1,2,3,4,
- Rong Wang1,2,3,4,
- Jun-Shi Shao1,2,3,4,
- Dong Zhang1,2,3,4
- 1Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
- 2China National Clinical Research Center for Neurological Diseases (NCRC-ND), Beijing, China
- 3Center of Stroke, Beijing Institute for Brain Disorders, Beijing, China
- 4Beijing Key Laboratory of Translational Medicine for Cerebrovascular Disease, Beijing, China
- 5Department of Neurosurgery, Beijing Mi Yun Hospital, Capital Medical University, Beijing, China
- Correspondence to Professor Dong Zhang; zhangdong0660{at}163.com
- Received 2 April 2017
- Revised 10 May 2017
- Accepted 30 May 2017
Abstract
Objective Few studies have reported the surgical treatment of carotid in-stent restenosis (ISR), more data and longer follow-up are needed. We describe the surgical treatment of ISR by standard carotid endarterectomy (CEA) with stent removal, including long-term follow-up in 10 patients from our centre.
Methods Ten patients from our centre who underwent CEA with stent removal for ISR were retrospectively analysed, including nine symptomatic and one asymptomatic ISR of at least 70% with mean age 67.3, the median time between carotid artery stenting and CEA was 17 months (range, 2–54 months).
Results Standard CEA with stent removal was performed in all 10 patients without much technical difficulty (9 male and 1 female, mean age 67.3). Two cases were performed in hybrid operation room. There were a total of three complications that happened in three patients (30%) respectively. An asymptomatic dissecting aneurysm was formed on the petrous internal carotid artery in one patient who was followed up without intervention. In the second case, dissection occurred in the arterial wall distal to the site of the stent after stent removal revealed by intraoperative angiography, and another stent was implanted. The patient sustained temporary hypoglossal nerve dysfunction postoperatively. The third patient suffered cerebral hyperperfusion with complete recovery when discharged. No neurological complications occurred in other seven patients. After follow-up of 25 months (range, 11–54 months), one patient died of rectal cancer without ischaemic attack and restenosis 4 years postoperation; in one patient occurred recurrent symptomatic restenosis (90%) 1 year later; all other patients remained asymptomatic and without recurrent restenosis (>50%) by follow-up carotid ultrasound or CT angiography.
Conclusion It seems that CEA with stent removal is a reasonable choice, by experienced hand, for symptomatic ISR with higher but acceptable complications. The indication of stent removal for asymptomatic ISR needs further observation.
- Carotid endarterectomy (CEA)
- In-stent restenosis (ISR)
- Carotid artery stenting (CAS)
- Stent removal
Introduction
Studies have demonstrated the effectiveness of carotid artery stenting (CAS) and carotid endarterectomy (CEA) for the treatment of carotid stenosis in the prevention of stroke.1–3 High rate of in-stent restenosis (ISR) after CAS has been reported to vary between 5% and 11%,4 5 with the steady increasing cases in CAS, cases of ISR are also increasing in recent years.6–8 Different treatment options including CEA, repeated CAS, percutaneous transluminal angioplasty (PTA) with drug-coated balloons (DCBs) or drug-eluting stents (DES) are available for treatment of ISR, but the optimal technique is not determined.9 10 Most studies generally consist of case reports or small case series, and generally obtain short-term follow-up.11 To the best of our knowledge, until now a total of 39 patients who underwent CEA with stent removal have been reported, no case has been reported recently since 2013.10 12 So, in this study, our experiences in surgical treatment of 10 patients with ISR who underwent CEA with stent removal with long-term follow-up in our centre were reported.
Methods
Patients
We retrospectively analysed 10 patients who visited the department of neurosurgery in our hospital between September 2012 and November 2016 because of ISR after CAS. Preoperative examination including digital subtraction angiography (DSA) and CT angiography (CTA) (DSA for eight patients, CTA for two patients) of neck arteries was performed in all patients. The clinical data such as age, gender, arterial hypertension, hyperlipidaemia, diabetes mellitus, heart disease, degree and location of initial stenosis and the status of the contralateral side, preoperative symptom and history of transient ischaemic attack (TIA) or stroke were studied.
Surgical treatment
Standard CEA with total removal of the stent was performed in all 10 patients by the same neurosurgeon Dr Zhang. The use of antiplatelet medication was not stopped before surgery. Intraoperative electrophysiological monitoring was performed, shunt tube was not used in all cases. The hypoglossal nerve was protected and the carotid bifurcation was completely exposed in order to place clamps proximally and distally. A 3–10 cm length arteriotomy was performed over the stent. The length of the arteriotomy depended on the length and the location of the implanted stent. In all cases, the stent was removed as one single complex with intimal hyperplasia, endarterectomy was done in the usual way without much difficulty. The artery was stitched up in a routine way without patch angioplasty.
Follow-up
Aspirin therapy (300 mg) was administrated per day in 1 week after surgery then long-term aspirin therapy (100 mg) after being discharged. CTA scan was performed within 1 week after surgery in all cases. Carotid ultrasound or CTA was repeated at 3 and 6 months and then yearly.
Results
Clinical characteristics of patients
In total, 10 patients (9 male and 1 female, mean age 67.3) with ISR were treated by CEA with stent removal. Of these, nine patients had hypertension, three patients had hyperlipidaemia, three patients had diabetes mellitus and four patients suffered heart disease (one coronary heart disease and three arrhythmias). All of these underlying chronic diseases were under control after giving medical administration and operations were safe after overall assessment of these risk factors. The patients were suggested of standard medical administration to control their chronic diseases during the follow-up. Nine patients had a symptomatic restenosis, including an ischaemic stroke in one, repetitive TIAs in eight, and one patient had asymptomatic haemodynamically significant restenosis. The rate of ISR in all cases was >70%, comprising contralateral occlusion in two and contralateral severe stenosis in one. The median time of recurrent symptoms after CAS was 6.5 months (range, 1–51 months). The detailed demographics for these cases are provided in table 1.
Baseline and clinical characteristics of patients
Surgical and follow-up results
The median time between CAS and CEA was 17 months (range, 2–54 months). Standard CEA was carried out in all patients, a 3–10 cm length arteriotomy was performed over the stent, the stents of all patients were removed as one single complex. No shunt tube and vascular patch were used in any cases. Carotid was opened with normal blood flow after stent removal in most patients, except for one patient where obstruction has happened in the carotid distal portion. A dissection in the arterial wall distal to the site of the stent was demonstrated by intraoperative angiography. As the operation was done in the hybrid operation room (OR), a stent was implanted immediately after angiography. The patient sustained hypoglossal nerve dysfunction while in complete recovery 7 days after surgery and was discharged in good health. An asymptomatic dissecting aneurysm was formed on the petrous internal carotid artery (ICA) in another patient who was followed up without intervention. The operative course of other patients was uneventful. One patient suffered cerebral hyperperfusion presenting with agitation and cognitive disorder in the first day after surgery while in complete recovery when discharged.
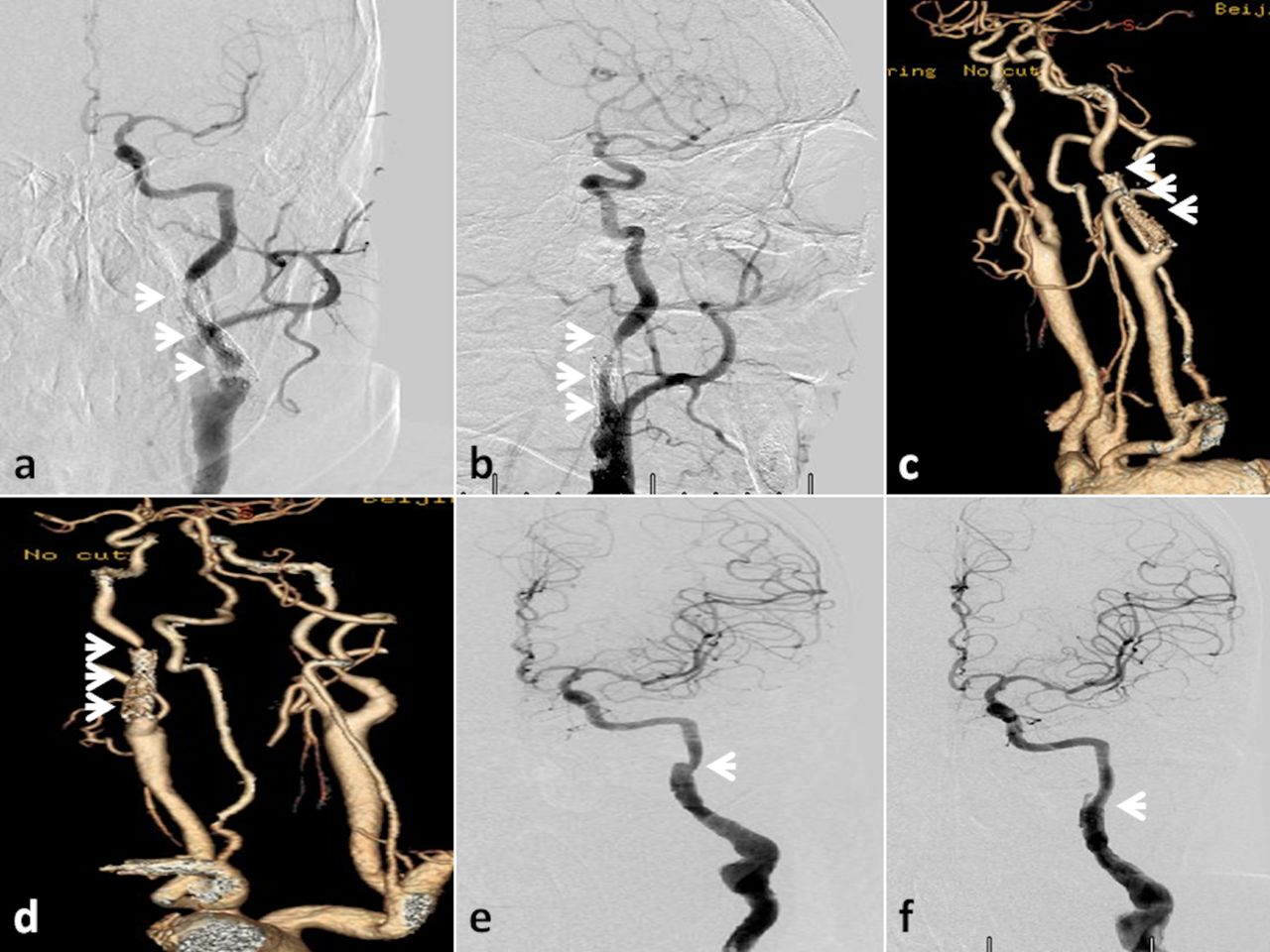
During a mean follow-up of 25 months (range, 11–54 months), one patient developed recurrent restenosis of 40% on CTA imaging 5 months after surgery, 80% 10 months after surgery and 90% 1 year after surgery (figure 1). One patient died 4 years later because of rectal cancer without recurrent ischaemic attack. All other eight patients remained asymptomatic, and none of them developed recurrent restenosis of >50% on carotid ultrasound or CTA imaging (table 2).
Detailed clinical data and follow-up results

A 65-year-old man with a clinical diagnosis of in-stent restenosis on his left side by digital subtraction angiography and CTA (A and B, arrow), CTA on the fifth day after operation shows well (C). However, the patient developed recurrent restenosis of 40% on CTA imaging 5 months after surgery (D), 80% 10 months after surgery (E) and 90% 1 year after surgery (F). CTA, CT angiography.
Discussion
So far, the optimal treatment option for ISR has not yet been determined. Different treatment options for ISR have been reported with good outcome including CEA, repeated CAS, PTA with DCBs or DES.13–16 However, no prospective studies could be carried out to directly compare these different techniques because of the low incidence. Most studies generally consist of case reports or small case series, and generally obtain short-term follow-up. More cases of ISR treated by new emerging endovascular techniques (DCBs or DES) have been reported than those of ISR treated by CEA with stent removal since 2005. To the best of our knowledge, until now a total of 39 patients who underwent CEA with stent removal have been reported, no case has been reported recently since 2013.10 17 Between September 2012 and November 2016, ten patients had been admitted to the department of neurosurgery in our hospital because of ISR after CAS. We analysed their clinical data and the longest follow-up (range, 11–54 months) had been done.
A total of 39 patients who underwent CEA with stent removal and about 200 patients who underwent endovascular treatment have been reported to date.10 The mean follow-up time was 48.8 months and 16 months, respectively. The rate of stroke between the two groups was not significantly different. Three patients among these 200 patients who underwent endovascular treatment have been reported with recurrent ISR while zero in CEA group. So, CEA with stent removal seems to have a low rate of recurrent ISR. However, CEA with stent removal operation needs more comprehensive assessment and much better physical condition compared with endovascular treatment. Elderly patients at high risk for complications preferred endovascular treatment as it was a relatively simple operation compared with CEA.
Reports have revealed that the rate of in-stent stenosis among studies ranges from 5% to 11%, with an interval time of 12–20 months.3 5 18–20 In this series, the median time of recurrent symptoms after CAS was 6.5 months (range, 1–51 months), the median time between CAS and CEA was 17 months (range, 2–54 months). All patients are in old age (mean age 67 years) combined with hypertension, which is the most common cause of carotid stenosis. Of these, nine patients were male while one was female. Male seems more common for recurrent stenosis. Earlier studies showed that most of the cases with ISR are asymptomatic,21 22 but whether these patients should perform repeat revascularisation at all remains questionable. However, 9 of 10 patients in our study were symptomatic. All patients were discharged without symptom.
In earlier studies, in about 39 patients of CEA with stent removal included, the majority of patients were followed up with good outcomes. No case of recurrent stenosis has been reported.10 14 16 19 20 In our study, one patient developed restenosis of 40%, 80% and 90% on CTA imaging 5 months, 10 months and 1 year after stent removal, respectively (figure 1). The patient was a 65-year-old man with hypertension for 7 years. He underwent a left CAS 4 years ago because of severe stenosis in the left ICA and occlusion in the right ICA, severe limb (both arms and legs) weakness and numbness on his left side disappeared after stent implantation. However, he presented with recurrent left limb weakness and numbness 17 months later. CTA demonstrated recurrent stenosis, then the balloon angioplasty was done without stent implantation. Eleven months later, he received CEA with stent removal because of restenosis. As the contralateral ICA was occlusion, his bilateral cerebral hemisphere was supported by the left ICA due to his open anterior communicating artery. Until now, the patient presented with mild limb weakness and numbness on his left side, endovascular treatment was suggested for him.
Until now, the standardised criteria and method for ISR are not defined.23 A wide range of ISR incidence was reported to be caused by different imaging tools such as CTA, ultrasonography (US) and DSA. Of these, US is the most commonly used technique to monitor ISR after CAS.24 25 However, the results of US are not always precise and usually are affected by some factors such as errors between different technicians. In our series, DSA and CTA were the most commonly used techniques to define ISR. DSA was performed in eight patients and CTA in two patients preoperatively. CTA or US was repeated at 3 and 6 months and then yearly after surgery. Preoperative DSA showed that restenosis was observed inner stent in five patients, on the border between the proximal end of stent and ICA in one patient, and on the border between the distal end of stent and ICA in two patients. CTA could show restenosis on the proximal or distal ICA to stent well while not inner stent. So we strongly suggest using DSA for diagnosis of ISR. Of course, CTA was preferred for follow-up examination. All patients were usually required CTA examination within 7 days postoperatively and unobstructed carotid was demonstrated in all patients.
Few perioperative technical difficulties or postprocedural compilations of CEA with stent removal have been reported in earlier studies.10 20 26 Our experience is that the complication of stent removal for symptomatic ISR was relatively higher but acceptable compared with CEA for CAS. The CEA operation for most cases with ISR is relatively normal without much technical difficulties. However, in some cases, if the stent is long enough or placed in distal position out of the surgeon’s control, it will be difficult to operate, nerve dysfunction and dissection in the arterial distal position may happen. In our series, one patient was implanted with a long stent in the right ICA together with a high carotid bifurcation (figure 2). The blood flowed out well from the distal ICA when the stent was removed, but a dissection in the arterial wall distal to the site of the stent was demonstrated by intraoperative angiography after the carotid was closed. As the operation was done in the hybrid OR, a stent was implanted in the distal position of the right ICA immediately after angiography. The patient sustained hypoglossal nerve dysfunction while in complete recovery 7 days after surgery and discharged in good health. Until now, he is well without any evidence of recurrent stenosis 31 months later after surgery. An asymptomatic dissecting aneurysm was formed on the petrous ICA in another patient who was followed up without intervention. The patient was well without symptom until now. The indication for operation of stent removal was not yet defined. In our opinion, intimal hyperplasia was demonstrated in our cases after the stent specimens were dissected and the intimal hyperplasia was stable compared with atherosclerotic plaque. So the indication should be more rigid than normal CEA, symptomatic ISR with severe stenosis is suggested, while stent removal for asymptomatic ISR needs further observation. On the other hand, we strongly suggest that intraoperative angiography is needed after stent removal especially when the stent is long and the carotid bifurcation is very high. The hybrid OR is a good choice for these patients (figure 3) if it is available. Two patients in our series were performed in the hybrid OR, and we demonstrated it is significant.
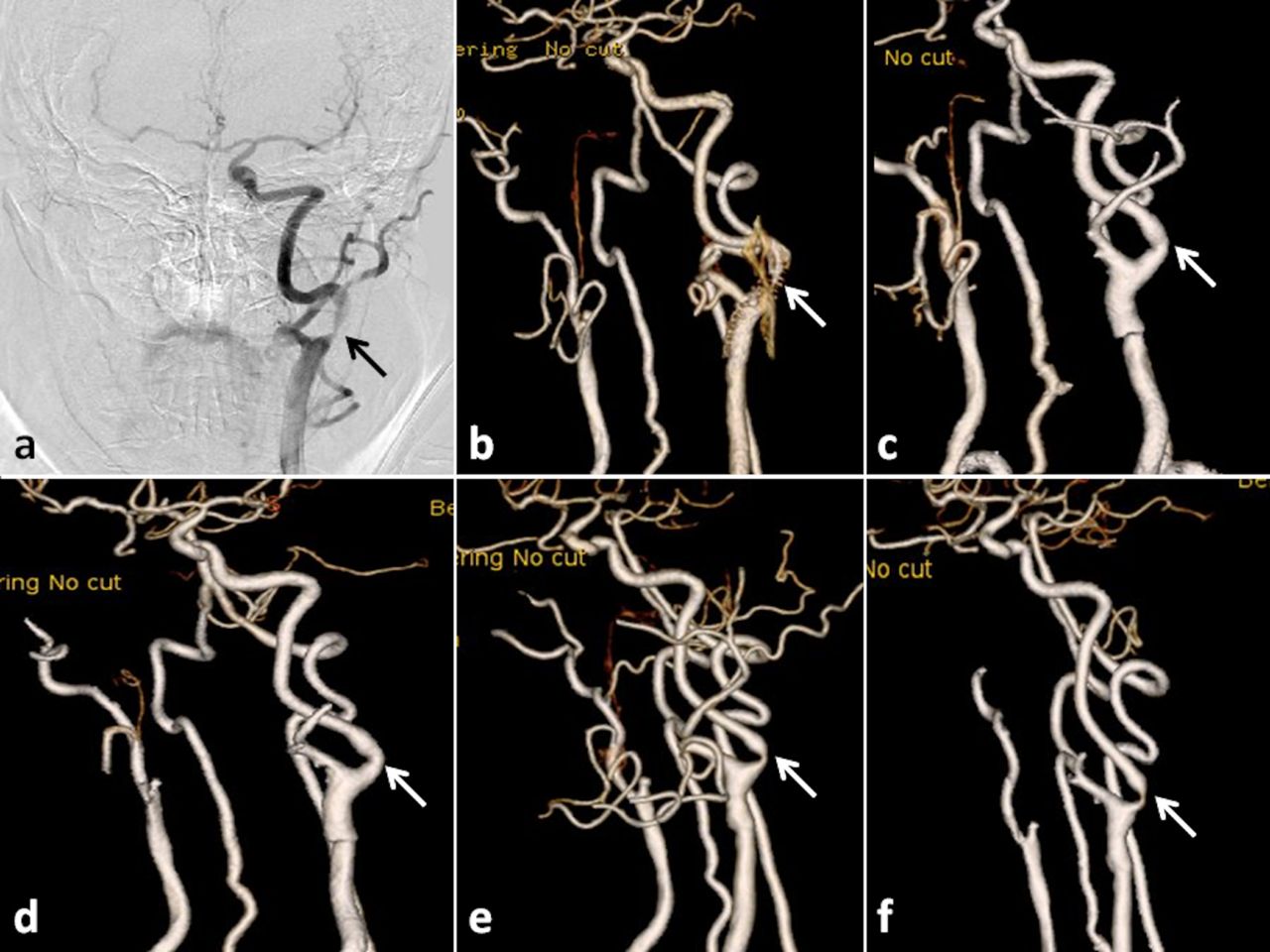
The patient is a 57-year-old man with a clinical diagnosis of in-stent restenosis on his left side by digital subtraction angiography and CT angiography (A–D, arrows), the implanted stent is very long and the carotid bifurcation is very high. A dissection in the arterial wall distal to the site of the stent was demonstrated by intraoperative angiography (E). The dissection disappeared after stenting (F).
{kind=link}
{kind=link}
{kind=link}
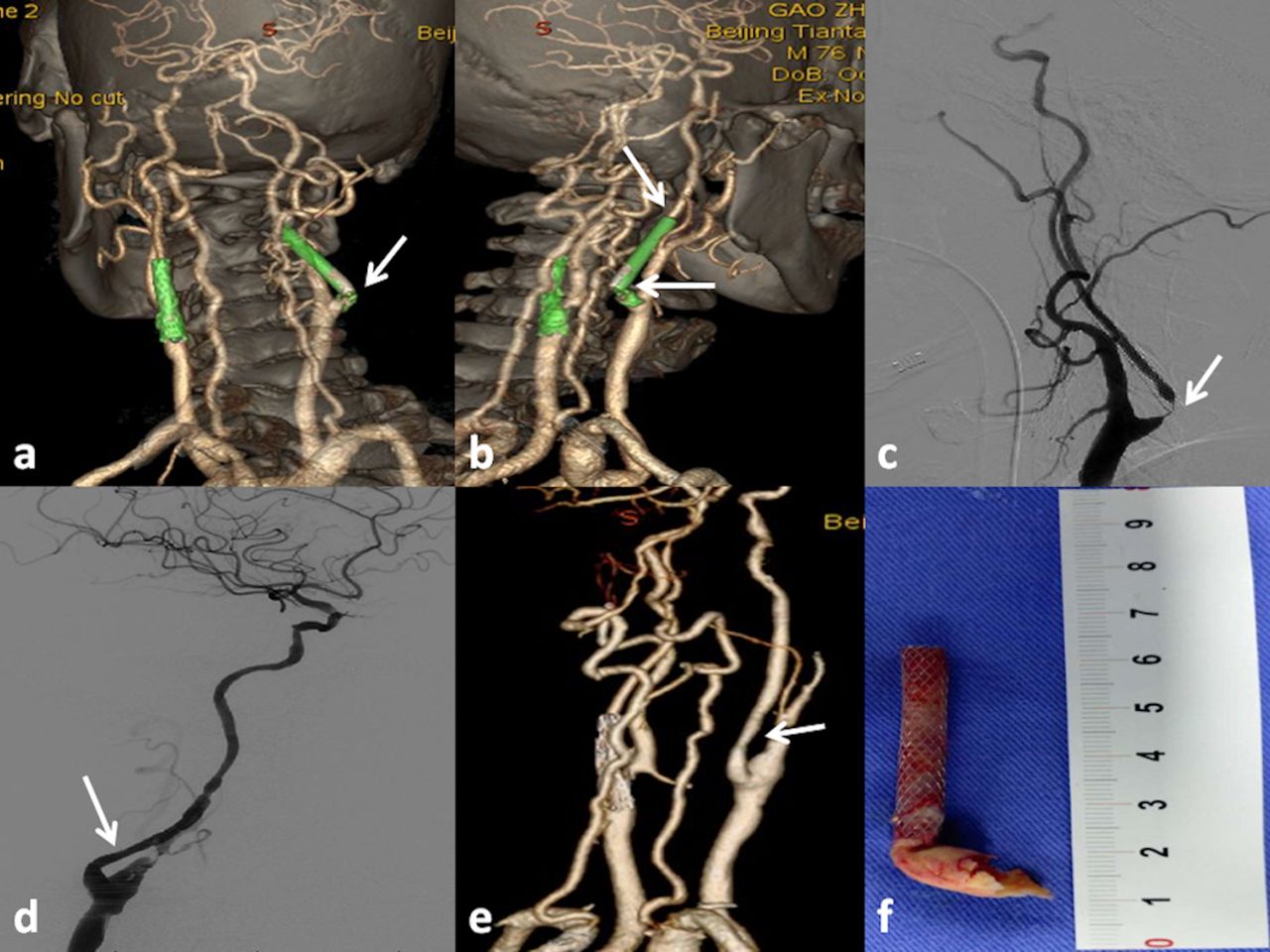
The patient is a 76-year-old man with a clinical diagnosis of in-stent restenosis on his right side by digital subtraction angiography and CTA (A–C, arrows). The operation was done in the hybrid operation room because of the long stent and the high carotid bifurcation. Intraoperative angiography after stent removal and CTA on the sixth day after surgery show well (D, E). The stent was one single complex (F). CTA, CT angiography.
Conclusion
Our experience suggests that CEA with stent removal is a reasonable choice, by experienced hand, for symptomatic ISR with relatively higher but acceptable complications. The indication of stent removal for symptomatic ISR should be more rigid than normal CEA and the indication for asymptomatic ISR needs further observation. The hybrid OR is a good choice for the patient with ISR if it is available.
Acknowledgments
We thank Dr Da-Peng MO (Chief of Invasive Technology Department, Beijing Tiantan Hospital, Capital Medical University) for general support.
Footnotes
Contributors All of the coauthors meet the criteria for authorship and are responsible for specific parts of this work. LBY, WY, QZ, MMJSS: conception or design of the work; the acquisition, analysis or interpretation of data for the work. JZZ, YZ, RW, DZ: revising the paper critically for important intellectual content.
Funding The China National Clinical Research Center for Neurosurgical Diseases (NCRC-ND)(2015BAI12B04); The Program of the National Natural Science Foundation of China (81371292).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of Tiantan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.