- Correspondence to Professor Shugui Shi; shishg{at}yeah.net
- Received 6 April 2017
- Revised 28 May 2017
- Accepted 1 June 2017
Abstract
Background Intravenous tissue plasminogen activator with or without mechanical thrombectomy during the acute phase are approved therapies for ischaemic stroke. Due to the short treatment time window (<6 hours) and often treatment failure, these patients would still have an intracranial arterial occlusion (IAO). It is unclear whether these patients can benefit from subsequent interventional recanalizationof their occluded artery in the subacute phase. In this retrospective study, we have examined the efficacy and safety in patients who have received either percutaneous transluminal angioplasty (PTA) or percutaneous transluminal angioplasty and stenting (PTAS) for IAO in the subacute phase of their stroke.
Methods Patients with subacute symptomatic ischaemic stroke caused by IAO were assessed to identify the responsible artery and low perfusion areas by CT angiography, MR angiography or digital subtraction angiography. In eligible patients, a PTA or PTAS was performed to reopen the occluded artery. Regular antithrombotic therapy, use of statins, control of risk factors and rehabilitation therapy were prescribed after the procedure. All patients had regular follow-up up to 12 months.
Results PTA or PTAS was performed in 16 patients with cerebral infarction caused by IAO in the subacute phase. After the procedure, 12 cases were recanalized, two were partially recanalized and two failed to open. One patient with left C6 segment occlusion of the carotid artery had a central retinal artery embolism after PTAS. The perioperative adverse events were 6.25%. At 3 months, the distribution of modified Rankin scale scores was 0 (seven cases), 1 (three cases), 2 (five cases) and 3 (one case).
Conclusion Selective PTA or PTAS could be performed in ischaemic stroke patients with a small infarct size and large area of hypoperfusion from an occluded large cerebral artery after the acute phase. It may improve neurological dysfunction and reduce the incidence of disability.
- cerebral infarction
- intracranial arterial occlusion
- angioplasty
- stent implantation
- efficacy
Introduction
One of the main causes of ischaemic stroke (IS) in Western countries is the stenosis or occlusion of extracranial large arteries.1 2 However, intracranial arterial occlusion (IAO) or stenosis is one of the main causes of IS in Asia.3 4 IAOs are characterised by extensive stenosis of one or many intracranial arteries.5 The Chinese Intracranial Atherosclerosis Study6 suggested that nearly 33% of Chinese IS patients had large IAO. Among them, occlusions of the middle cerebral artery (MCA), posterior cerebral artery (PCA) and internal carotid artery (ICA) were among the top 3.
Intravenous tissue plasminogen activator (tPA)7 8 and mechanical thrombectomy9–15 within the time window are the two approved treatments for acute IS. However, since the vast majority of patients cannot reach a qualified stroke centre in time after the onset of stroke, the current rate of recanalization during the acute phase is still very low.16 In China, approximately 20% of patients could arrive at the emergency room within 3 hours of onset and 12.6% of these patients were qualified to receive thrombolytic therapy. However, only 1.6%–2.4% of patients received intravenous tPA.17 Meanwhile, intravenous tPA achieved about 10% of successful revascularisation. Many patients would still be left with an occluded intracranial artery.
IS patients with an IAO have a higher incidence of recurrent stroke, about 7.27% a year.6 The rate of recurrent stroke is about 5.16% in those with 70%–99% stenosis and 3.82% in those with 50%~69% stenosis group. IAO may also affect cognitive function and lead to poor quality of life in an IS patient at a later time.18–20 Therefore, recanalization and re-establishing cerebral perfusion can prevent the recurrence of stroke and improve the quality of life.
Presently, no report on the recanalization of IAO has been identified. The benefit and risk of such treatment remains unclear beyond the time window of the acute phase. In this study, multimodel imaging studies were used to evaluate the feasibility to conduct percutaneous transluminal angioplasty (PTA) or percutaneous transluminal angioplasty and stenting (PTAS) of occluded large intracranial arteries. Cerebral perfusion and collateral circulation of these patients were evaluated by CT perfusion (CTP), MR perfusion (MRP) and digital subtraction angiography (DSA). Then, PTA or PTAS was performed to reopen the occluded arteries if all inclusion criteria were met. Regular antithrombotics, use of statins, controlling of risk factors and rehabilitation therapy were prescribed after PTAS. All patients were regularly followed up for any perioperative complications and long-term outcomes.
Methods
Study design, participants and procedures
This was a single-centre retrospective cohort study. Between August 2011 and September 2016, all patients admitted for IS with occlusion of a major intracranial artery confirmed by CT angiography (CTA), MR angiography (MRA) and/or DSA were considered for the inclusion of the study. They had to meet all of the following criteria: (1) cerebral infarction was caused by large vessel occlusion; (2) the occlusion was <90 days; (3) new infarction was mainly caused by occlusions of perforators; (4) the fresh distal occlusion of blood vessels contained mainly small artery–artery embolisms and the area of cerebral infarction did not exceed 1/5 of the area of the supplying artery; (5) large low perfusion area was present with >50% of mismatch on CTP, MRP and DSA; and (6) patient’s condition worsened despite aggressive medical treatment. Patients with the following characteristics will be excluded from the trial: (1) known allergy or contraindication to aspirin, clopidogrel, heparin, nitinol, local or general anaesthesia; (2) history of life-threatening allergy to contrast dye. If not life threatening and can be effectively pretreated, patient can be enrolled at physician’s discretion; (3) active peptic ulcer disease, major systemic haemorrhage within 30 days, active bleeding diathesis, platelets<100 000, haematocrit <30, international normalised ratio (INR) >1.5, clotting factor abnormality that increases the risk of bleeding, current alcohol or substance abuse, uncontrolled severe hypertension (systolic pressure >180 mm Hg or diastolic pressure >115 mm Hg), severe liver impairment (aspartate aminotransferase (AST) or alanine aminotrans (ALT)>3× normal, cirrhosis), creatinine >3.0 (unless on dialysis); (4) major surgery (including open femoral, aortic or carotid surgery) within previous 30 days or planned in the next 90 days after enrolment; (5) Indication for warfarin or heparin beyond enrolment (note: exceptions allowed for use of systemic heparin during stenting procedure or subcutaneous heparin for deep vein thrombosis prophylaxis while hospitalised; and (6) pregnancy or of childbearing potential and unwilling to use contraception for the duration of this study.
Thrombolysis in cerebral infarction (TICI) classification was applied with DSA findings21: TICI 0 flow (total occlusions) referred to the absence of any antegrade flow. TICI 1 flow (functional occlusion) was faint antegrade flow beyond the occlusion. TICI 2 flow (partial reperfusion) indicated delayed or sluggish antegrade flow with complete filling of the distal territory. TICI 2a showed a perfusion of less than half of the arterial distribution of the occluded artery, for example, only filling of one M2 division. TICI 2b described a perfusion of equal to or more than half of the vascular distribution of the occluded vessels, for example, reperfusion of two or more M2 divisions. TICI 3 indicated normal flow that filled the distal artery bed completely. In our study, after PTAS, a TICI 2b–3 was considered complete reperfusion, TICI 2a meant partial reperfusion and TICI 0–1 meant either no reperfusion or the operation was unsuccessful.22
The procedure was performed under general anaesthesia. Patient was given intravenous heparin bolus of 3000 IU followed by heparin 1000 IU/hour intravenous drip. After paracentesis of the right femoral artery, an 8 F arterial sheath was placed, and then a 6 F guiding catheter was advanced to the proximal segment of the occluded artery. A 0.010 micro-guidewire (Synchro, Boston), assisted by a micro-catheter, was introduced into the occluded artery and carefully passed through the occluded lesion to the distal segment. Then, the micro-guidewire was withdrawn and the length of the occlusion was determined by micro-catheter angiography. If the length of the occluded segment was <10 mm, the micro-catheter was exchanged for a 0.014 micro-guidewire (Transend or Synchro, Boston) and a 1.5–2.25 mm balloon (Gateway, Boston) was placed in the occluded segment; the balloon was then inflated carefully and slowly to recanalize the vessel. The stenting system was used in cases with a distal arterial diameter >1.5 mm, and the length of occluded segments was ≤10 mm. An Apollo or a Wingspan stenting system was acceptable based on the treating physician’s decision.
Intravenous heparin infusion was continued at 300 IU–500 IU/hour for 24 hours after the procedure. Blood pressure was reduced to 80% of the preoperative blood pressure level. After 24 hours, patients were required to take dual-antiplatelet medications (100 mg/day aspirin and 75 mg/day clopidogrel) for 3 months, and then continued with either one of the two antiplatelet drugs for their lifetime. Patients also were prescribed with statins (20–40 mg/day), provided with education on controlling of other risk factors and a rehabilitation consultation after PTA or PTAS.
Outcomes
We investigated two outcomes: the score on the modified Rankin scale (mRS) at 3 months after the operation and the safety outcomes during the 30-day perioperative period. The mRS is a seven-point scale ranging from 0 (no symptoms) to 6 (death). A score of ≤2 indicates functional independence. In our study, the mRS was assessed by trained personnel who were blinded to the type of the treatment. Safety outcomes included any vascular accidents occurring during the 30-day perioperative period.
Results
Patients
Sixteen patients received interventional recanalization procedures (13 men, 3 women) with cerebral infarction during subacute phase of their stroke (table 1). All patients did not receive intravenous tPA or mechanical thrombectomy. The time from the onset to the interventional procedure was 4–90 days. The preoperative TICI score of 14 patients was 0, and 1 in other 2 patients. The National Institutes of Health Stroke Scale (NIHSS) score before the procedure ranged from 2 to 32. The occluded sites were within the M1 segment (12 patients), M2 segment (2), C6 segment of left ICA (1) and middle and lower segments of the basilar artery (1).
Data of the 16 patients treated by percutaneous transluminal angioplasty or percutaneous transluminal angioplasty and stenting
Operation results
Twelve cases were recanalized successfully after endovascular therapy (TICI 2b–3). Among them, angioplasty and stenting were performed in 11 patients and 1 had only angioplasty. Two of them were partially recanalized (TICI 2a) and two were not recanalized (TICI 0–1). The rate of successful recanalization was about 75%. One patient with left C6 segment occlusion had a subsequent left central retinal artery embolism after PTAS. No other vascular events or death occurred within 30 days after the procedure. The proportion of adverse events during the perioperative period was around 6.25%.
Follow-up and outcome
All 16 patients had follow-up by telephone and in the clinic. Seven patients reached mRS score of 0, three reached 1, five reached 2 and one had a 3 at 3 months after the procedure. The proportion of patients with a mRS score of 0–2 at 3 months was 93.75%. Fifteen patients had no recurrence of stroke or transient ischemic attack (TIA), and one patient with partial recanalization had recurrent bilateral limb numbness during the follow-up.
Case example
Case 1
A 59-year-old woman presented with weakness in the right limb. She had 10-year history of hypertension. A detailed physical examination showed a right central facial and lingual nerve palsy. On the Medical Research Council (MRC) scale, the muscle strength of the right upper limb was 3/5 and right lower limb was 4/5. The NIHSS score was 8: level of consciousness 1, level of awareness 1, facial paralysis 1, upper limb movement 1, lower limbs movement 1, sensory 1 and articulation 1. Diffusion-weighted MRI (DWI) revealed an acute infarct in the left basal ganglia on the following day (figure 1A). MRA showed that the M1 segment of the left MCA was occluded (figure 1B). DSA confirmed the occlusion. Its distal artery was small and sparse. Statin and antiplatelet medications were used. On the eighth day of hospitalisation, the symptoms became worse. Her right arm had no strength and right leg was 3/5. The NIHSS score was 15. DWI revealed an acute infarct in the left basal ganglia with a small dot-like embolic infarct in the cortex (figure 1C). Large areas of low perfusion were present in the left MCA territory (figure 1D). She received left MCA angioplasty (figure 2A,B) and was started on antithrombolytics, statin and antihypertensive drugs. Rehabilitation continued. Her symptoms significantly relieved. Follow-up DSA examination indicated that recanalization was successful after 40 days (figure 2C).The mRS score was 2 after 3 months.
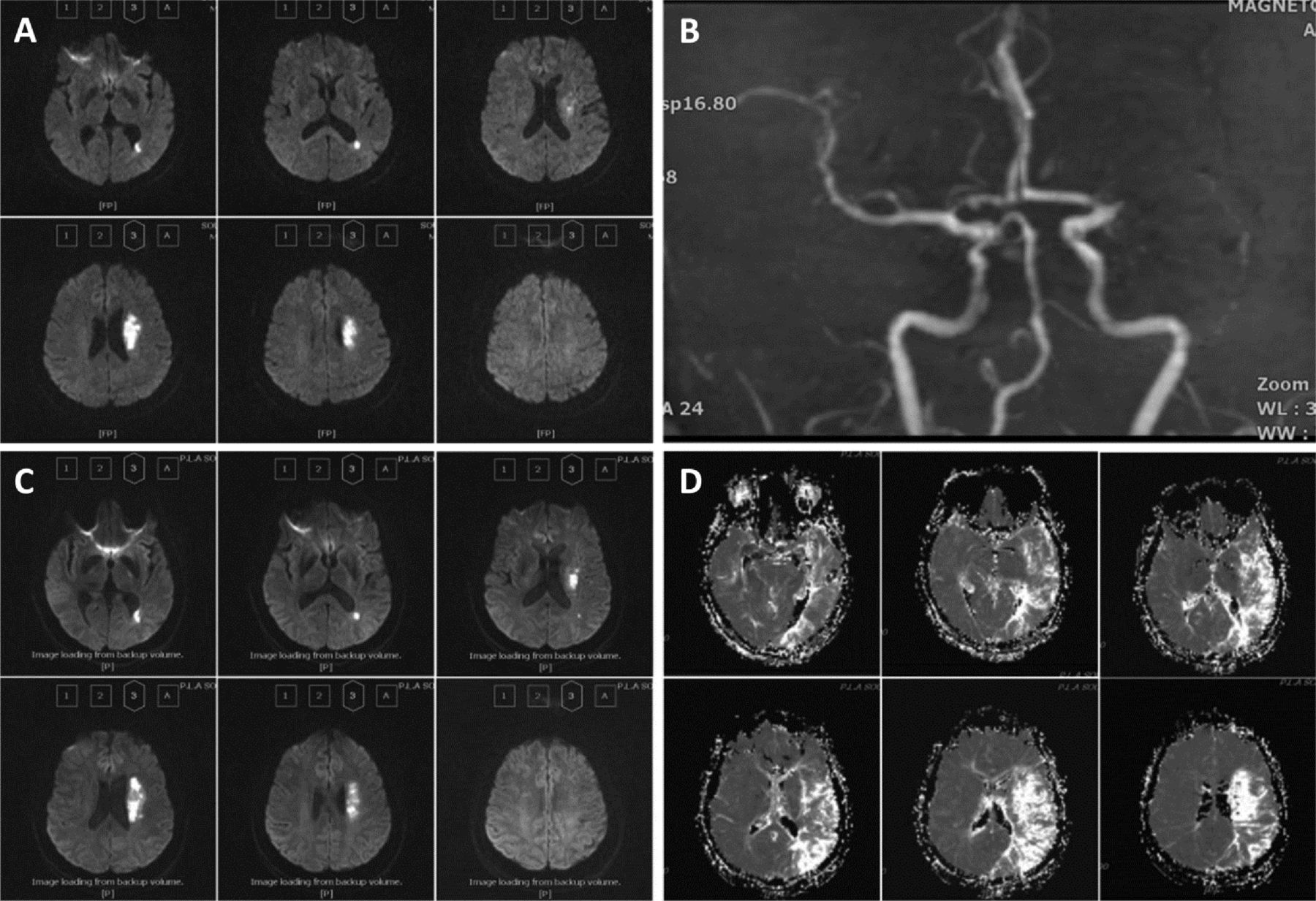
MR revealed a small infarct size and large area of low perfusion in the left hemisphere with the occlusion of left middle cerebral artery (MCA). (A) Diffusion-weighted MRI revealed an acute infarct in the left basal ganglia. (B) MR angiography showed that the M1 segment was occluded. (C) MRI re-examination after 8 days revealed an acute infarct in the left basal ganglia region with a small dot-like embolic infarct in the cortex. (D) There were large areas of low perfusion in the left MCA territory.

The process of left middle cerebral artery (MCA) angioplasty.(A) A left MCA angioplasty. (B) The M1 segment of the left MCA was recanalized after angioplasty. (C) Digital subtraction angiography examination indicated that recanalization was successful after 40 days.
Case 2
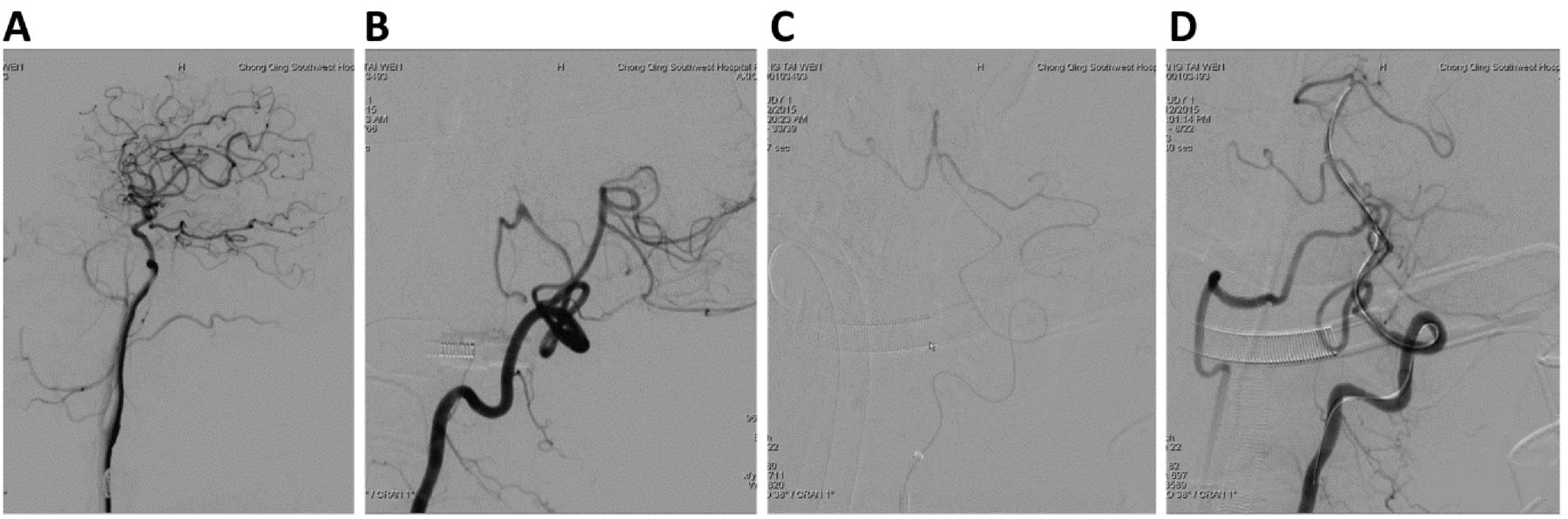
A 55-year-old man presented with dizziness and worsening of claudication for 43 hours. He had a history of hyperlipidaemia, hypertension and smoked for >30 years. On physical examination, his vital signs were stable. Neurological examination revealed horizontal nystagmus when looking to the right, vertical nystagmus when looking up, supervened dysdipsia, a weak gag reflex, normal muscle strength and weak ataxia. The NIHSS score was 3: language 1, articulation 1 and ataxia 1. MRI revealed an embolic infarct in the bilateral cerebellar peduncles and right cerebellar hemisphere (figure 3A). MRA showed that the vertebrobasilar arteries were occluded (figure 3B). The diagnosis was vertebrobasilar syndrome. On the sixth day of hospitalisation, the symptoms became worse. The NIHSS score was 6: following command 1, language 2, articulation 1 and ataxia 2. On the eighth day of hospitalisation, cerebral DSA suggested that the right vertebral artery and the V3 segment of the left vertebral artery were occluded. His bilateral PCA and the upper segment of the basilar artery were supplied by the left posterior communicating artery but were barely present. Statin and dual-antiplatelet medications were continued, volume expansion therapy was started and blood pressure was raised up to help with perfusion. On the 10th day of hospitalisation, MRI suggested that the bilateral cerebellar infarction was increased significantly (figure 4). The patient’s stroke symptoms continue to worsen. On the 17th day of hospitalisation, he became comatose and his Glasgow Coma Scale score was 5 (E2V1M2). He then had PTAS of the basilar artery (figure 5). The symptoms were significantly relieved after PTAS. Although the patient was conscious and the limbs could move, the reaction was slow. The mRS score was 3 after 3 months.
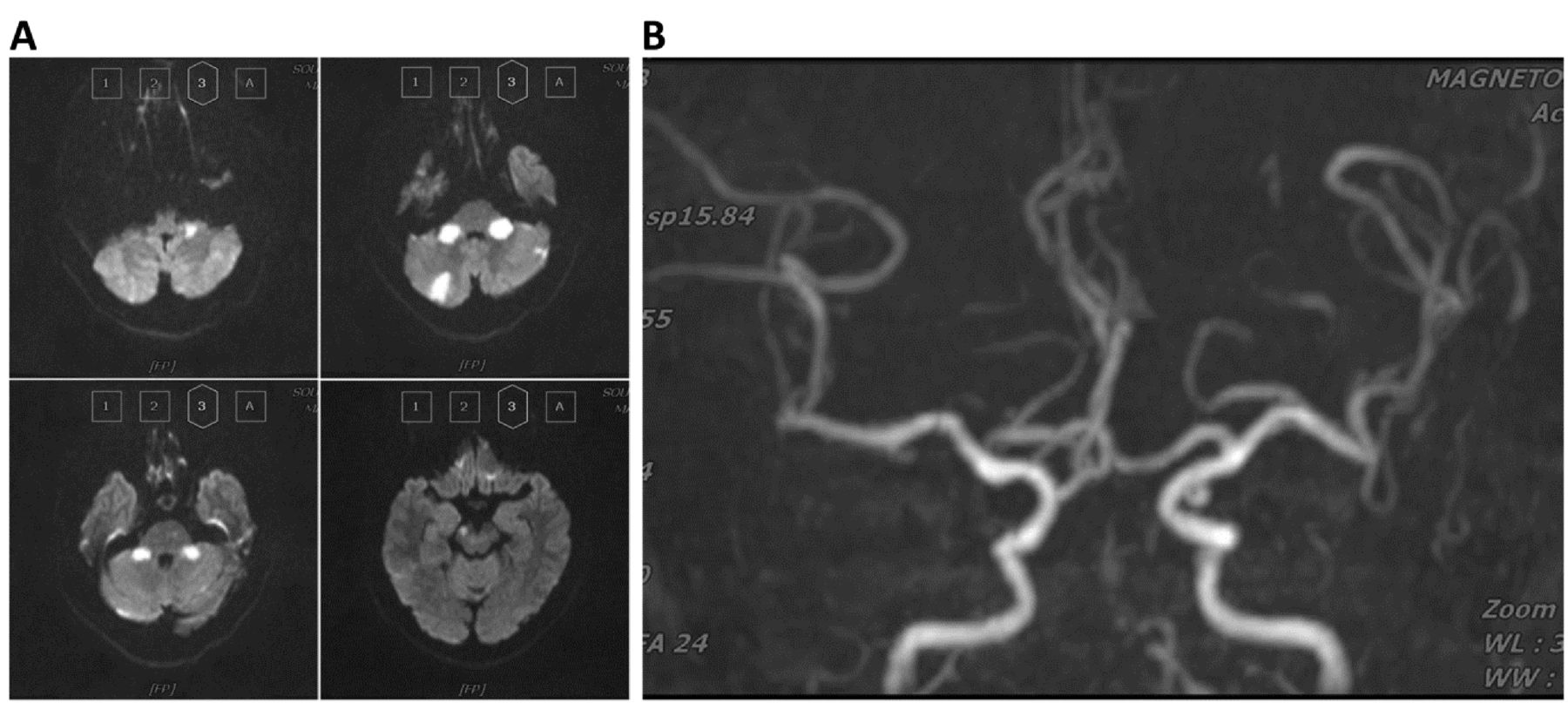
MRI examination. (A) MRI revealed multiple clusters of ischaemic infarctions in bilateral cerebellar hemisphere. (B) Both vertebral arteries and basilar artery were occluded.
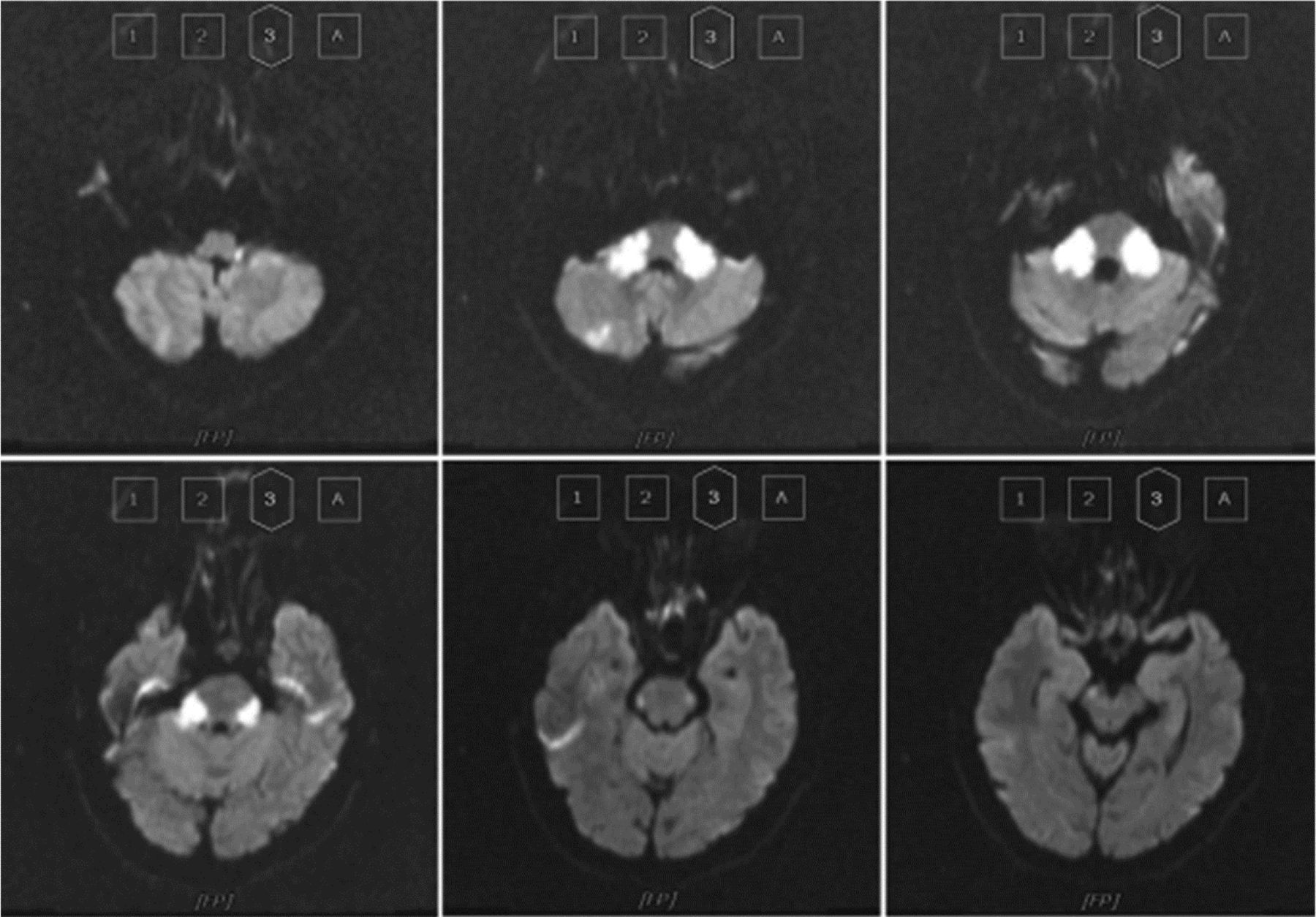
Second MRI examination. On the ninth day of hospitalisation, MRI suggested worsening of bilateral cerebellar infarctions and the involvement of brainstem.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recanalization of the occluded basilar artery by percutaneous transluminal angioplasty and stenting. (A) Right ICA angiography revealed that the superior segment of the basilar artery and bilateral posterior cerebral arteries were partially supplied by posterior communicating artery. (B) Basilar artery was completely occluded in the middle segment and left posterior inferior cerebellar artery (PICA) showed compensatory enlargement. (C) Micro-catheter passed through the stenosis of the inferior segment of the basilar artery and revealed basilar artery occlusion beyond the middle segment. (D) After balloon dilation and implantation of the self-expandable stent, basilar artery was completely recanalized.
Discussion
Our study suggested that selective PTA or PTAS could be performed in patients with IAO in the sub-acute phase when small infarctions were present but there were larger areas of low perfusion. The procedure improved neurological function and reduced the incidence of disability even when the procedure was done several days later. IAO is the main cause of ischaemic stroke in Asia.3 4Presently, recanalization outside the time windows with bridging therapy is without clinical evidence and risk of haemorrhage or worsening of stroke from hyperperfusion syndrome is high. The ischaemic penumbra around the infarct tissue may be preserved if blood flow is restored.23 However, if blood flow is not restored for a long time, brain cells would not survive and lead to worsening of clinical symptoms and even death.24 25 The risk of haemorrhage after reperfusion may depend on the size of the infarction.26 Therefore, we suggest that it is still feasible to recanalize when the volume of cerebral infarction is small and area of low perfusion is large, even if the presence of cerebral infarction has been prolonged. This could be the theoretical basis for possible successful recanalization of occluded large artery in the subacute phase.
The key points to a successful recanalization at a later time in this patient population include (1) a diagnosis of cerebral infarction; (2) mild to moderate symptoms from artery–artery embolisms distal to the occluded vessel; (3) <1/5 of arterial supply of the cerebral infarction of the responsible artery; (4) a mismatch of >50% on CTA, MRA or DSA in the hypoperfused area; and (5) deteriorated neurological symptoms despite the best medical management.
The timing from the onset to recanalization procedure was between 4 and 90 days in our series. recanalization was achieved with micro-wire and micro-catheter plus balloon angioplasty and stenting. Balloon angioplasty and stenting were not applied in two partial recanalization patients because the distal artery was slender or with excessive tortuosity. One patient had only balloon angioplasty without stenting in order to avoid potential haemorrhagic transformation since his infarction was in left basal ganglia. Neither stent-assisted clot retriever nor tPA was used in our patients. Since the occlusion was caused by vascular stenosis and that stent-assisted retriever would cause recurrent thrombosis because of the rupturing of the plaque, angioplasty with stenting could cover up the unstable plaque.27 Our series of 16 patients with no recurrent vascular occlusions or haemorrhages suggested that such treatment was feasible. However, perforating arteries could be occluded during balloon angioplasty since the plaque was crushed. This was why one of our patients had a central retinal artery occlusion. Therefore, perforating arteries should be avoided during the procedure.
The safety of the operation is one of the main factors that affect the outcome of recanalisation. Both SAMMPRIS and VISSIT28–30 trials showed failure in intracranial arterial angioplasty and stenting. In these two studies, patients receiving PTAS had a higher incidence of postoperative bleeding. However, patients treated in our study had low complication rate because of the selection process.
Our series indicated that PTAS in the subacute phase in select patients with IAO could be safe and effective. Our patients demonstrated improved functional outcome in otherwise predictable progressive large vessel stroke and likely poor outcome. However, our study had limitations: it was a retrospective, single-centre study with small sample and no controls. It is necessary to evaluate the feasibility of this treatment with large sample multicentre studies.
In conclusion, PTA or PTAS was safe and effective in patients with IAO type of stroke but with a small infarct size and large area of hypoperfusion during the subacute phase. The selection criteria need to be followed strictly in order to ensure a better outcome. Future large studies are needed to further confirm our findings.
Footnotes
Contributors KC and SS contributed to the conception, design of the study and the operative procedure. All authors acquired and analysed data. XH and SS drafted the manuscript. SS drafted the figures. All authors contributed to editing the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol was approved by the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.