Article Text

Abstract
Purpose Cerebral misery perfusion (CMP) is a condition where cerebral autoregulatory capacity is exhausted, and cerebral blood supply in insufficient to meet metabolic demand.
We present an educational review of this important condition, which has a range of clinical manifestations.
Method A non-systematic review of published literature was undertaken on CMP and major cerebral artery occlusive disease, using Pubmed and Sciencedirect.
Findings Patients with CMP may present with strokes in watershed territories, collapses and transient ischaemic attacks or episodic movements associated with an orthostatic component. While positron emission tomography is the gold standard investigation for misery perfusion, advanced MRI is being increasingly used as an alternative investigation modality. The presence of CMP increases the risk of strokes. In addition to the devastating effect of stroke, there is accumulating evidence of impaired cognition and quality of life with carotid occlusive disease (COD) and misery perfusion. The evidence for revascularisation in the setting of complete carotid occlusion is weak. Medical management constitutes careful blood pressure management while addressing other vascular risk factors.
Discussion The evidence for the management of patients with COD and CMP is discussed, together with recommendations based on our local experience. In this review, we focus on misery perfusion due to COD.
Conclusion Patients with CMP and COD may present with a wide-ranging clinical phenotype and therefore to many specialties. Early identification of patients with misery perfusion may allow appropriate management and focus on strategies to maintain or improve cerebral blood flow, while avoiding potentially harmful treatment.
- cerebral misery perfusion
- carotid occlusion
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key Points
Consider the diagnosis of CMP in patients with:
orthostatic TIA symptoms
episodic limb-shaking
watershed territory infarcts
high-grade carotid steno-occlusive disease
decrease in CBF with increased oxygen extraction distal to an occlusion
Confirm diagnosis with imaging of carotids and PET/MRI ASL
Blood pressure should be lowered cautiously
Consider revascularisation in selected individuals
Address episodes of hypotension aggressively
Background, pathogenesis and epidemiology
Cerebral misery perfusion (CMP) is a condition where regional cerebral blood flow (rCBF) is reduced relative to the regional metabolic demand for oxygen, and is defined by increased tissue oxygen extraction fraction (OEF) on positron emission tomography (PET).
Atherosclerosis of the internal carotid artery or the middle cerebral artery causing occlusive disease is the most common cause of CMP. Less common causes include dissection, cardiac embolism, radiation vasculopathy, vasculitis and other chronic inflammatory conditions such as Takayasu’s aortoarteritis. The occlusive process leads to reduced CBF in the distal arterial system, leading to haemodynamic impairment with disease progression. Table 1 illustrates the stages of cerebral haemodynamic impairment and the pathophysiology behind the development of CMP. Most of our understanding of CMP comes from studies looking at carotid occlusive disease (CAO), on which this review will focus.
Pathophysiology of cerebral misery perfusion and stages of cerebral haemodynamic impairment
Many patients with CAO remain asymptomatic and therefore the true prevalence of asymptomatic CAO is unknown. When ‘symptomatic’ (transient ischaemic attack (TIA) or stroke), the prevalence of CAO has been reported to be 6/100 000; however, the authors in the study felt that true prevalence was probably higher as many patients with transient symptoms may not have sought medical help.1 In addition to the above, the difficulty in ascertaining the epidemiology of CMP is compounded by the limited availability of diagnostic investigations such as PET, and the under-recognition of symptoms that may be attributed to CMP in day-to-day clinical practise.
Clinical and radiological features
People with CMP may present with a range of clinical manifestations such as collapses, strokes in watershed territories or with reversible neurological deficits resembling TIAs. The recognition of this condition enables appropriate management, with avoidance of unnecessary and potentially harmful treatment. Several factors such as collateral blood supply, extent of haemodynamic impairment, contribution of posterior communicating arteries and rapidity of development of CAO determine the clinical phenotype (table 2). Chronic occlusions from progressive atherosclerotic disease usually develop slowly and may allow for the formation of collaterals. Such occlusions are usually asymptomatic and are often discovered incidentally on vascular imaging after a TIA or stroke. van Laar et al found that in functionally independent patients with symptomatic CAO, the ipsilateral middle cerebral and anterior cerebral arteries were supplied by the vertebrobasilar and contralateral internal carotid arteries, respectively.2
Clinical spectrum of carotid occlusive disease
While strokes due to CAO may present with clinical features similar to those due to any other aetiology, certain distinctive radiological features suggest an underlying haemodynamic mechanism. Rosary-like infarction of the centrum semi-ovale (indicating internal watershed territory infarction) has been shown to be the most sensitive marker for haemodynamic failure (figure 1 A,B and C).3

(A) Diffusion-weighted MRI showing internal watershed infarcts. (B) T2-weighted MRI showing posterior cortical watershed infarction. (C) CT brain showing anterior cortical watershed infarct.
In patients with transient symptoms, a detailed history may reveal an underlying haemodynamic problem. Particular attention should be paid to symptoms provoked by standing up, exercise, postprandial or the recent commencement of antihypertensives. Rarely, patients present with transient repetitive involuntary movements in the limbs contralateral to the occluded internal carotid artery (ICA), called limb-shaking TIAs.4
Syncope and collapses may be caused by CMP.5 In our own experience, syncope was the presenting feature in 7 patients out of a case series of 204 patients, who were later found to have unilateral or bilateral CAO at Nottingham City Hospital. This was felt to have been an underestimation as many more patients had given a history of ‘collapses’, which in retrospect were probably syncopal episodes. In the same case series, nine patients presented with transient global amnesia; it is possible that the resultant cerebral ischaemia from CAO may be involved in the pathogenesis of this poorly understood condition.6
In addition to the increased OEF measured by PET, which has limited availability, there may be other ways to identify those patients with CAO, haemodynamic insufficiency and a higher stroke risk. Leptomeningeal and ophthalmic collateral circulation, watershed infarction, impaired vasoreactivity to acetazolamide and orthostatic limb-shaking were all noted to predict haemodynamic failure, increased OEF on PET and higher stroke risk.7 Another study identified age, cerebral (rather than retinal) symptoms, limb-shaking TIAs at presentation, history of previous strokes and the presence of leptomeningeal collaterals as risk factors for recurrent stroke in patients with symptomatic CAO.8
Investigations
Doppler ultrasound (DU) is the usual initial imaging modality to look for disease of the extracranial ICA. It has the benefit of being cheap and non-invasive, with a diagnostic accuracy of 97% in identifying complete CAO.9 Distinguishing between complete and near-occlusion can however be difficult: an important distinction to make, as revascularisation should be considered in patients with near occlusion. DU with the use of contrast improves the ability to distinguish between total and near-occlusion.10 It is however operator dependent, and has a limited field of view that renders the evaluation of vessel course and tandem lesions difficult.
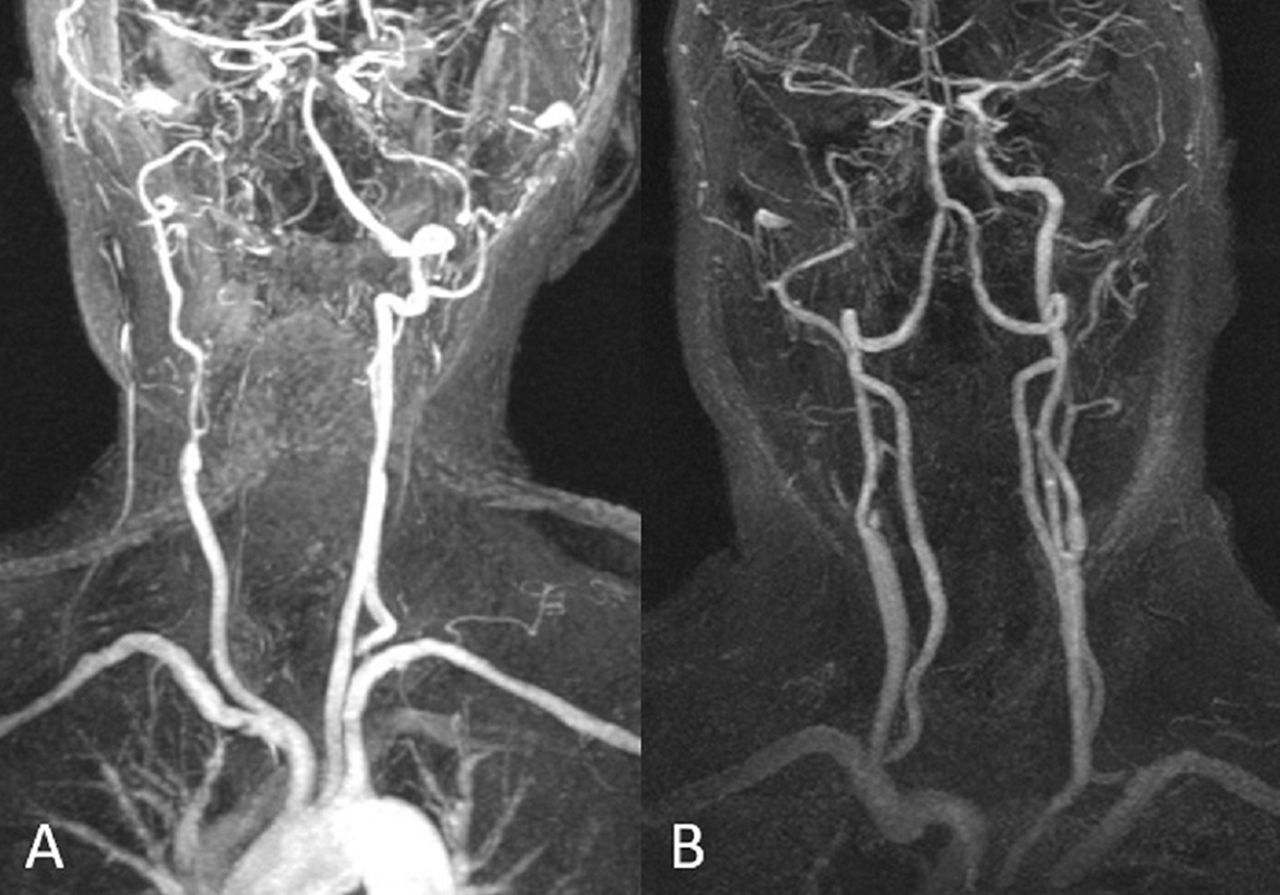
The ‘gold standard’ for the evaluation of CAO is digital subtraction angiography. But it is invasive and carries the risk of neurological complications. Multislice CT angiography (figure 2A) has excellent correlation with catheter angiography in diagnosing complete versus near-occlusion of the ICA, and if used in combination with DU averts the need for catheter angiography.11 12 Time-of-flight magnetic resonance (MR) angiogram (figure 2B) uses the movement of blood as endogenous contrast to measure the degree of stenosis. However, it is flow-dependent, and may overestimate the degree of carotid stenosis due to signal loss in areas of slow flow from severe steno-occlusive disease. Gadolinium-enhanced MR angiogram is less susceptible to this, and has equivalent sensitivity to DU in diagnosing complete CAO, and is probably better than DU at identifying near-occlusion.13
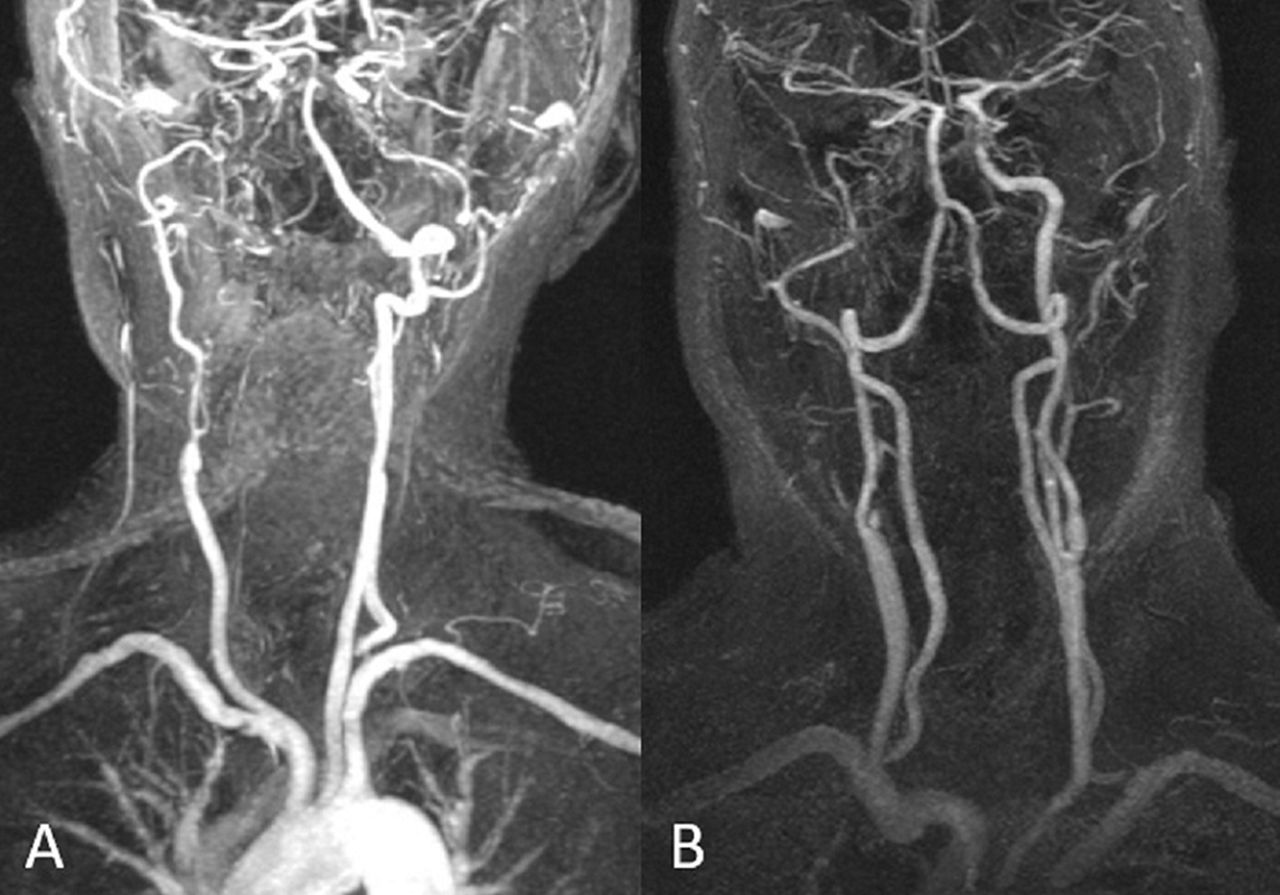
(A) CT angiogram showing bilateral internal carotid occlusive disease (CAO). (B) MR angiogram showing right internal CAO.
The assessment of CBF is important when clinical and radiological features suggest haemodynamic impairment. PET remains the gold standard for assessing cerebral haemodynamics, but there are issues with high cost and concerns over methodology.14Transcranial Doppler (TCD) US, Xenon-CT and single-photon emission CT have all been used to assess cerebral haemodynamic status and vasoreactivity.15–17 However, TCD US is also operator-dependent and may not technically possible in some individuals, while CT-based techniques carry radiation exposure. One advantage with TCD is the assessment of collateralisation, using the direction of flow in the anterior communicating and posterior communicating arteries.
In recent years, there has been particular interest in advanced MRI techniques. Arterial spin labelling (ASL) MRI uses radiofrequency pulses to non-invasively label water protons in blood, and can measure vasodilator capacity in symptomatic carotid stenosis.18 T2*-based blood oxygen level-dependent contrast (BOLD) MRI uses deoxyhaemoglobin as an indicator of OEF. Cerebrovascular reactivity (CVR) can be quantified using hypercapnia BOLD MRI with good reproducibility.19 The technique involves serial MR scans obtained during periods of normocapnia and hypercapnia. CVR maps are then obtained and cerebrovascular vasodilatory capacity can be assessed. An increase in the BOLD signal indicates cerebral vasodilatation, whereas loss of CO2-induced BOLD reactivity suggests maximum compensatory vasodilatation. As BOLD MRI allows whole-brain imaging, it is possible to assess regional variations in CVR.
In spite of the recent developments in advanced MR techniques, PET has been the investigation of choice in major trials evaluating CMP and revascularisation techniques (to be discussed later). There are however other complexities with PET imaging in addition to cost and unavailability. While the original definition of CMP was increased OEF, there has been much heterogeneity in what is considered to be CMP. Some investigators have used a hemispheric OEF ratio of >1.13 to define CMP (Carotid Occlusion Surgery Study (COSS) study), while others have included decreased CBF and decreased CBF/CBV ratio in addition to increased OEF.20
Prognosis and outcomes
Flaherty et al reported the risk of stroke in patients with symptomatic carotid occlusion to be 10% and 14%, at 1 and 5 years, respectively. The same study also reported a mortality of 29% at 5 years.1 The risk of recurrent stroke in patients with symptomatic CAO is 2.4%–7% per year, and this rises significantly in the presence of haemodynamic impairment due to exhausted cerebrovascular reserve.8 21–23 The ipsilateral ischaemic and all stroke risk was found to be higher in patients with CMP (17.1% and 26%, respectively), than those without CMP (3.1% and 9.2%, respectively).20 The stroke risk in patients without CMP decreased over time; however, there was no such reduction in stroke risk over time in patients with CMP. The presence of CMP and bilateral asymptomatic lacunar infarcts were significant independent predictors of future ipsilateral ischaemic strokes. The study included patients with middle cerebral and internal carotid artery occlusive disease, and a separate analysis of the two groups revealed that CMP was a predictor of recurrent ischaemic stroke in both.20
The ability of patients with CAO and CMP to lead normal lives may be impaired in other ways, separate from the devastating effect of stroke. There is now accumulating evidence of impaired cognition and quality of life in patients with CAO.24 25 What is not known is the long-term effects of CAO and CMP on mood, level of function and disability. There is a need for high-quality research evaluating these specific domains in relation to revascularisation for patients with CAO.
Management
Revascularisation
An important first step is to distinguish between complete occlusion and near-occlusion. Symptomatic internal carotid artery near-occlusion presents a strong case for revascularisation through carotid endarterectomy (CEA) or carotid artery stenting (CAS), in order to reduce future stroke risk. While CAS in patients with near-occlusion can be effective in preventing stroke recurrence, there have been concerns with cerebral hyperperfusion syndrome (CHS) and postprocedure vascular events.26 There is of course a risk of CHS with any carotid revascularisation procedure, and this was in fact originally described after CEA. In older people, CAS is associated with increased stroke risk, whereas CEA has similar neurological outcomes in both the young and old but at the expense of increased mortality in the elderly.27
The evidence for revascularisation in the setting of complete occlusion is weak. Yasargil was the first to describe an anastomosis between superficial temporal artery and a branch of the middle cerebral artery (figure 3).28 While initially incorporated into clinical practice, bypass surgery was abandoned after publication of the initial extracranial-intracranial (EC-IC) bypass surgery, which showed no benefit with surgery over best medical treatment.29 The study was however criticised for poor design and implementation. Additionally, it was hypothesised that surgery should only be offered to patients with haemodynamic impairment.22

{kind=link}
{kind=link}
{kind=link}
Patient with bilateral carotid occlusive disease who has had a right extracranial-intracranial bypass shunt surgery.
The COSS and Japanese EC-IC Bypass Trial (JET) were set up to answer this question. JET showed benefit at 2 years (second interim analysis) for patients undergoing EC-IC bypass, but the final results were never published.30 COSS was stopped early after an interim analysis showed no additional benefit with surgery compared with best medical treatment.31 Both studies had recruitment problems, and required PET imaging, which is expensive and not readily available. A subsidiary study of COSS also found that EC-IC bypass surgery did not improve cognitive function in patients with increased OEF.32 The study however was small, and did not evaluate quality of life, level of disability or mood. Nevertheless, anecdotal evidence suggests that EC-IC surgery may be of benefit in carefully selected patients with CAO and haemodynamic impairment benefit from revascularisation. Research evaluating the natural history of patients with CAO is needed.
Finally, another way to revascularise patients with CAO is through CAS, which has been shown to be feasible and practical;33 34 however, larger trials are needed to prove efficacy and long-term follow-up data.
Medical management
Conventional vascular risk factors should be addressed and appropriately treated. The benefit of strict blood pressure (BP) control in CAO and CMP is controversial. The loss of compensatory cerebrovascular vasodilatory capacity and the resultant uncoupling of cerebral autoregulation from systemic BP makes cerebral perfusion susceptible to any fall in systemic BP, especially in borderzone regions. Aggressive BP lowering in this context may therefore lead to unwanted clinical outcomes.
The presence of CMP seems to modify the relationship between BP and stroke risk. Patients with lower BP and CMP had a higher stroke risk, while those with a higher BP without CMP had a greater stroke risk.35 In the non-surgical control arm of COSS, lowering BP (<130/85) was associated with lower subsequent stroke risk.36 On the other hand in another study, lowering BP (<130 systolic) was noted to increase the risk of ipsilateral stroke in those with CMP.37 Guidelines in the UK recommend a BP target of 130–150 systolic for those with ‘severe bilateral carotid stenosis’.38 Although CAO and severe bilateral carotid stenosis are not the same entities, a proportion of patients with the latter would have developed CMP.
Our recommendations
While we recommend liberal BP control (systolic 130–150) to avoid cerebral hypoperfusion, it is important to tailor the target BP for an individual patient according to clinical response. Particular consideration should be given to the frequency and severity of symptoms that occur with lowering BP, presence of postural hypotension and the severity of haemodynamic impairment found on CBF studies. Any depletion of intravascular volume should be corrected, and the temporary cessation of antihypertensives should be considered at times of hypovolaemia or expected hypovolaemia (such as during periods of fasting), or when on holiday in warm countries (case report).39
Finally, notwithstanding the unestablished benefit from surgical procedures to improve CBF, it is the opinion of the authors that certain patients may still benefit from revascularisation. Such patients may include those who are thought to be developing cognitive impairment related to CAO, with proven CMP from haemodynamic studies, and those who are relatively young with good baseline functional status, favourable anaesthetic risk profile and no life-limiting comorbidities.
Conclusions
Patients with carotid occlusive disease and CMP may present to multiple specialities with a wide-ranging clinical phenotype, and should be considered in those with watershed infarcts, collapses and TIAs or episodic movements associated with an orthostatic component. Early identification of patients with CMP may allow appropriate management and focus on strategies which may maintain or improve CBF, while avoiding potentially harmful treatment.
References
Footnotes
Contributors SM was responsible for the conceptualisation of the work.
The literature review was performed by MM and SM.
The initial draft was prepared by MM, with critical revisions and additions by NS, PMB and SM.
All authors have approved the final version of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it published Online First. Figures 1, 2 and 3 have been corrected as well as the key points.