Article Text

Abstract
Objectives Microembolic signals (MES) on transcranial Doppler (TCD) predict stroke and cognitive decline. Plasma levels of total homocysteine (tHcy), a prothrombotic factor, are higher in patients with microemboli in carotid stenosis and in patients with paradoxical embolism. In this study we assessed the association between the level of tHcy and the number of MES in patients with mechanical heart valves (MHVs).
Methods TCD monitoring was performed to detect MES before and after breathing 100% oxygen and repeated every 2–4 weeks up to six times.
Results Twenty-five patients with MHVs (mean age: 63.60±10.15 years) participated in this study; 15 were men (66.47±7.25 years) and 10 were women (59.30±12.60 years). In total, there were 126 study visits. In multiple regression, higher tHcy was associated with more MES in both preoxygenation (OR 1.34 (95% CI 1.07 to 1.68, P=0.009)) and postoxygenation (OR 1.40 (95% CI 1.07 to 1.83, P=0.01)) phases. Current smoking and the length of time between the operation and monitoring also correlated with a higher number of MES before and after breathing oxygen, particularly in women.
Conclusions Higher tHcy and smoking were associated with a higher MES count in both preoxygenation and postoxygenation phases. Because smoking can be stopped and hyperhomocysteinaemia is treatable, these are clinically important findings.
- homocysteine
- mechanical heart valves
- valvular heart disease
- microembolic signal detection
- transcranial doppler ultrasound
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- homocysteine
- mechanical heart valves
- valvular heart disease
- microembolic signal detection
- transcranial doppler ultrasound
Introduction
Valvular heart disease (VHD) remains a major heart condition worldwide. Despite a dramatic decline in the incidence and prevalence of rheumatic heart disease in many high-income countries, VHD is still common, probably due to an increase in the number of patients with degenerative valve diseases.1 In the USA, about 2.5% of the population have VHD, with a sharp rise after age 65.1 Accordingly, an ever-increasing number of patients with VHD may need surgical intervention. Despite a significant improvement in the diagnosis, surgical/interventional methods and follow-up of diseased valves in recent decades, there is still a risk of short-term and long-term prosthesis-related complications, namely embolic events.2 Therefore, it is important to identify and control treatable risk factors in these patients.
An elevated plasma level of total homocysteine (tHcy) is a modifiable risk factor for stroke, if not coronary artery disease.3 The vascular effects of homocysteine are not limited to arterial atherosclerosis or venous thrombosis.3 Hyperhomocysteinaemia also increases the risk of embolic events,4 including embolic strokes.5 Patients with carotid stenosis and microemboli on transcranial Doppler (TCD) have significantly higher levels of tHcy,6 as do patients with paradoxical embolism.7 This is particularly evident in the elderly and patients with renal dysfunction.8 Despite mounting evidence of embolic events due to hyperhomocysteinaemia, the current literature remains largely silent regarding any correlation between tHcy and embolic events in patients with mechanical heart valves (MHVs). This is partially due to difficulties in prospectively following up embolic complications in such patients and identifying those at risk of disabling or fatal events. TCD ultrasound is able to detect microembolic signals (MES), which can serve as an indicator of embolic events.9
This study was designed to assess the association between tHcy and the number of MES in patients with MHV.
Methods
Study population
Patients with MHVs were invited to participate in this study. Eligible patients were identified from a registry of patients who underwent mechanical valve replacement at the London Health Sciences Centre and who were living within a radius of 50 km from our research centre. A letter of information was sent to eligible patients, explaining the study design, aims and methods; 26 patients agreed to participate and gave written consent.
The study was carried out at the Stroke Prevention & Atherosclerosis Research Centre, Robarts Research Institute, London, Canada. We included patients 18 years old or older with a prosthetic mechanical aortic and/or mitral heart valve, and taking warfarin with or without aspirin as their antithrombotic therapy. We excluded patients with a history of congestive heart failure, severe pulmonary disease, if unable to tolerate oxygen administration and those without appropriate temporal bone window for insonation. Clinical and demographic data, including vascular risk factors, medications and type of valves, were collected during the first interview and from the patient registry and electronic medical record. We assessed the level of tHcy at the first visit. To minimise inconvenience to the patients, visits were scheduled to coincide with patients’ scheduled measurement of the international normalised ratio (INR), which was approximately every 2–4 weeks, based on the fluctuations in INR and patient preference. The London Health Sciences Centre Core Laboratory processed all blood work, and the INR results were also sent to the physician adjusting the patient’s warfarin dose.
TCD protocol
We performed TCD monitoring using a TCD ultrasonographic instrument (ST3 100 PM, Spencer Technologies) equipped with a head frame (Marc 600 Spencer Technologies) and two 2 MHz probes. We monitored both middle cerebral arteries at a depth of 48–54 mm. Based on the protocol of Rodriguez et al,10 each visit began with 30 min of TCD monitoring while the patient was breathing room air, and if microemboli were detected, then up to 1 hour of TCD monitoring was carried out while breathing 100% oxygen administered at a rate of 8 L/min via one-way Hi-Ox mask (Ceretec). (The purpose of the inhalation of oxygen is to eliminate nitrogen from the blood so that nitrogen bubbles, which commonly form in the cavitation of flow beyond the valve, are prevented.) Monitoring on oxygen began 20 min after beginning oxygen inhalation. The first monitoring was performed in June 2014 and the last was in August 2016. MES were defined according to the recommendations of the Consensus Committee of the Ninth International Cerebral Hemodynamic Symposium.11 We repeated TCD monitoring between one and six times, based on feasibility and patient preference. figure 1 and the online supplementary video illustrate the detection of microemboli by TCD.
Supplementary file 2
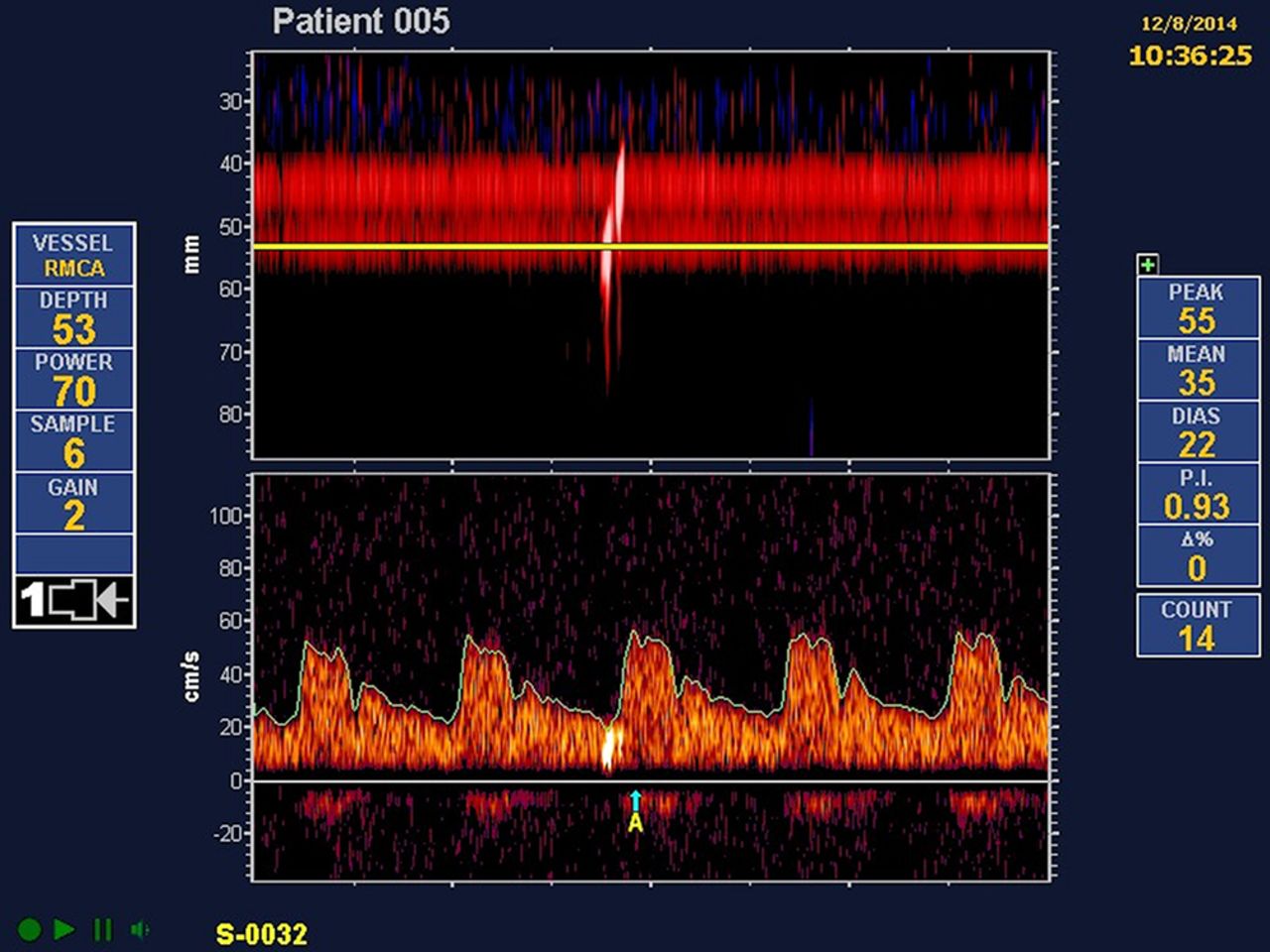
Microemboli in a patient with a mechanical valve. The patient was a 65-year-old man with a St Jude Medical aortic mechanical heart valve. The depicted microembolic signals were recorded during the preoxygen phase. The online supplementary video provides the ‘click’ sound that is heard when microemboli occur.
Statistical analysis
Data were expressed as mean+SD or median and IQR (25th–75th percentile). We analysed categorical variables using Χ2 or Fisher’s exact tests. We used the Mann-Whitney or Kruskal-Wallis H test to analyse non-normally distributed quantitative variables. Normality of data distribution was assessed with the Kolmogrov-Smirnov test. Differences between the means of multiple variables were compared with the post-hoc test (Bonferroni method). To account for the possible effects of body surface area (BSA) on valve conditions, we divided valve areas (cm2) by BSA (m2). BSA was calculated as the following:

We performed a generalised linear mixed model (Poisson distribution) to identify independent variables associated with the number of MES before and after breathing oxygen. The duration of monitoring was defined as a structural variable. All statistical analyses were performed using SPSS V.24 for Windows XP. P values <0.05 (two-tailed) were considered statistically significant.
Results
Twenty-five patients with MHVs (mean age: 63.60±10.15 years) participated in this study; 15 were men (66.47±7.25 years) and 10 were women (59.30±12.60 years). In total, there were 126 study visits. While men had a higher BSA as compared with women (P=0.02), the valve area/BSA ratio was not different between men and women. No significant difference was observed in the level of tHcy or INR between men and women (table 1).
Demographic characteristics of study participants by sex
The median (25th–75th percentile) number of MES in the preoxygenation and postoxygenation was 10 (0–73) and 4 (0–19) per hour, respectively. MES>1 were seen in 86 of 126 (68.25%) monitoring periods in the preoxygenation phase. After breathing oxygen, the number of MES decreased in 79 of 86 (91.86%) monitoring periods, increased in 4 of 86 (3.49%), and MES were not detected in the remaining 3 of 86 periods.
The majority of patients had a St Jude MHV (n=18, 72%), with Medtronic (n=3) being the next most common type. Patient characteristics by valve type are shown in online supplementary table 1. One patient had an On-X valve. Three patients had more than one type of mechanical valve. Those with Medtronic MHVs were significantly younger than patients with a St Jude (50.33±12.42 vs 66.56±7.99, P=0.02). The most frequently replaced valve was aortic (n=18: 15 St Jude and 3 Medtronic MHVs), followed by mitral (n=3: 1 On-X and 2 St Jude). No significant difference was observed between the INR and tHcy levels based on the type and location of the mechanical valves (online supplementary tables). Atrial fibrillation was more frequent in those with aortic and with multiple valve replacements (online supplementary table 2).
Supplementary file 1
In linear multiple regression analysis, tHcy was associated with a higher number of microemboli in both the preoxygenation (OR: 1.34, 95% CI 1.07 to 1.68, P=0.009) and postoxygenation (OR: 1.40, 95% CI 1.07 to 1.83, P=0.01) phases. The difference in the number of MES before versus during O2 inhalation was greater with lower levels of INR; patients with lower INR had a greater decline in the number of MES with O2 inhalation: with INR<2.5 there were −74.86+88.45 fewer MES during O2 inhalation; with INR>2.5 there were −37.17+49.92 during O2 inhalation (P=0.01). This was more pronounced by dividing INR into three categories: INR<2, −106.52+99.24; INR 2–3, −43.58+69.26; INR>3, −37.17+49.92 (P=0.017). This is surprising, as it seems to suggest that increased coagulation contributed to formation of more gaseous emboli rather than solid emboli.
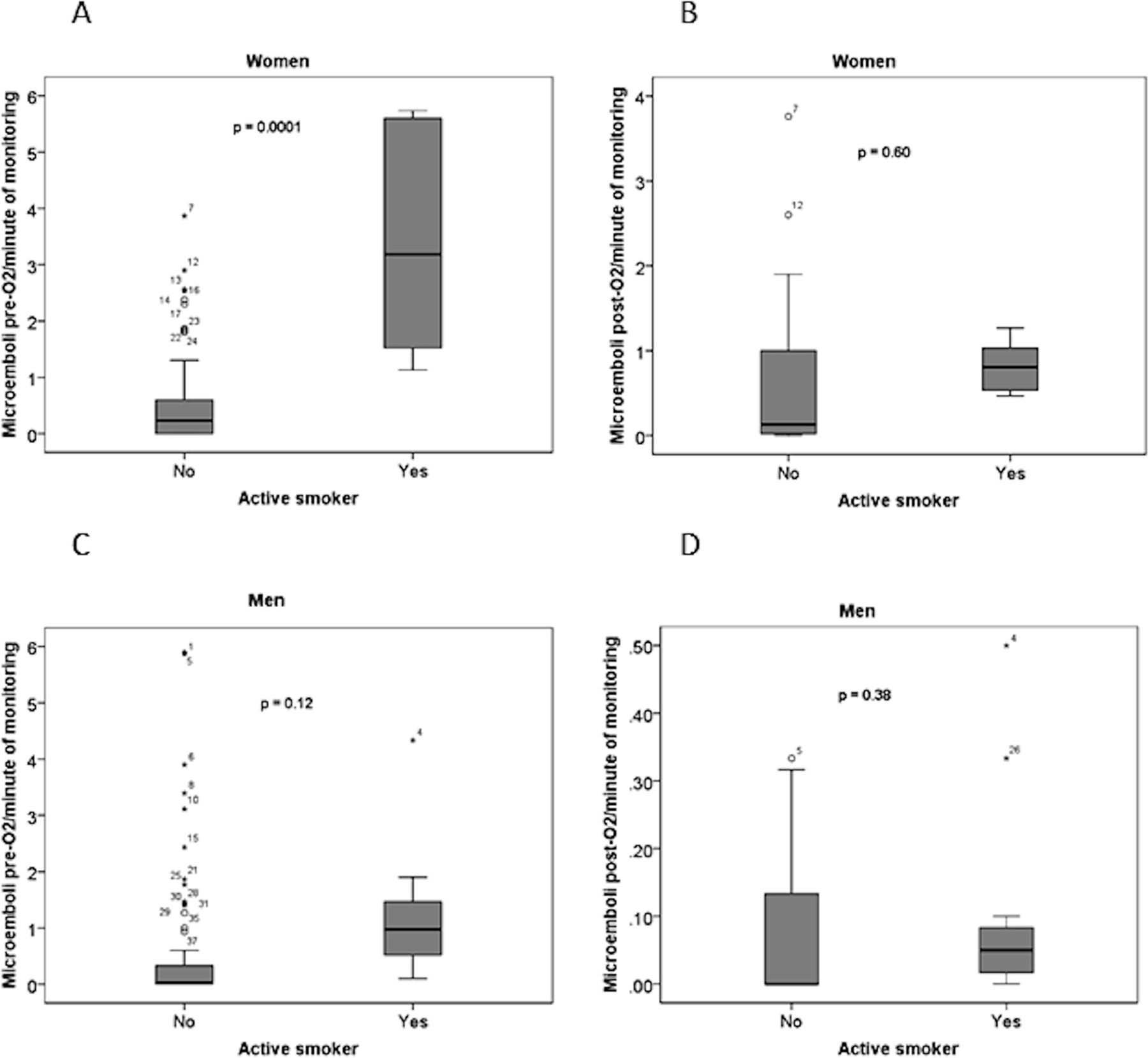
With an increasing length of time between the operation and monitoring (in months), a slightly higher number of MES was observed in both the preoxygenation (OR: 1.007, 95% CI 1.001 to 1.009, P=0.01) and the postoxygenation phase (OR: 1.01, 95% CI 1.007 to 1.015, P=0.000). Current smokers also had a higher MES count in both phases compared with non-smokers. Patients who were taking aspirin and warfarin had a higher number of MES only in the postoxygenation phase versus those merely on warfarin. The location of valve replacement was also correlated with the number of MES in the preoxygenation phases, with a higher MES count in patients with aortic valve replacement or multiple valve replacements. Increasing age was associated with a lower number of MES in the preoxygenation and postoxygenation phases. MES counts were not different by sex in linear regression, after adjustment for the other independent variables in the analysis (table 2). However, as shown in figure 2, women had more microemboli than men, particularly in the pre-O2 phase. There was a significant interaction between sex and smoking with regard to the number of microemboli before O2 inhalation. As shown in figure 1, there were more microemboli in smokers; this was only significant for women.
{kind=link}
{kind=link}
Number of microemboli per minute of monitoring in men and women, active smokers versus non-smokers. (A) Women pre-O2; (B) women during O2 inhalation; (C) men pre-O2; (D) men during O2 inhalation. Women had more microemboli than men (note the difference in scale of the x-axes), and smokers had more microemboli than non-smokers; the difference was significant for women.
Generalised linear mixed analysis of independent variables associated with the number of microembolic signals in patients with mechanical heart valves
Discussion
In repeated TCD monitoring of 25 patients with MHVs, we frequently observed MES in both preoxygenation and postoxygenation phases. No clinical embolic events were noted during the period of the study. Higher tHcy was associated with a higher number of microemboli in the preoxygenation and postoxygenation monitoring phases, indicating a possible association between tHcy and both gaseous and solid microemboli. These findings are clinically important, suggesting that tHcy should be assessed and treated in patients with MHVs. In the context of folate fortification of the grain supply, as now pertains in North America and many other countries, metabolic vitamin B12 deficiency is the most common cause of hyperhomocysteinaemia, is present in 30% of patients with stroke above age 70 and is often undiagnosed,12 so serum B12 should also be assessed in patients with MHVs.
Homocysteine is a toxic sulfur-containing amino acid that can promote the atherosclerotic process via increasing oxidative stress, oxidation of low-density lipoprotein and endothelial dysfunction.13–15 In this study, we evaluated MES as an indicator of embolic events. Although microemboli do not lead to immediate focal neurological deficits, they predict a high risk of stroke6 and have important clinical significance, including early identification of those at increased risk of cognitive impairment.9
We found that increased tHcy was associated significantly with the number of MES before and after breathing 100% oxygen. In theory, the majority of MES in the preoxygenation phase are gaseous microbubbles induced by cavitation, while MES in the postoxygenation phase are mainly solid particles. Many studies showed that hyperhomocysteinaemia is associated with procoagulant activity,16 left atrial thrombus formation,17 thromboembolic complications,18 19 stroke in atrial fibrillation19 and persistent arrhythmia after successful epicardial ablation of atrial fibrillation.20 21 In addition, homocysteine may have arrhythmogenic effects due to changes in atrial action potentials4 and inhibition of atrial myocyte potassium channels.22 Therefore, a higher number of solid microemboli in our patients with hyperhomocysteinaemia might be due to a combination of arrhythmogenic and coagulopathic effects of homocysteine. Moreover, circulating gaseous microbubbles may be recognised in our body as a foreign substance, triggering the coagulation cascade via surface tension effects on platelet aggregation.23
Several studies showed that microemboli in patients with MHVs are associated with an increased risk of stroke24 and with impaired cognitive function.25 26 The hazardous effects of microemboli are not limited to solid MES. Gaseous microemboli may also lead to tissue ischaemia via different mechanisms, from blood flow obstruction in the capillary system to inflammatory response and complement activation.23 Therefore, a higher number of MES, either gaseous or solid particles, in patients with elevated tHcy has important clinical applications, particularly for the prevention of stroke and cognitive impairment among patients with MHVs. Our findings suggest the opportunity for homocysteine-lowering therapy with B vitamins. Although for some time it was believed that B vitamins did not prevent stroke, it is now apparent that lowering homocysteine does reduce the risk of stroke; in the early clinical trials, harm from cyanocobalamin among study participants with renal impairment obscured the benefit among participants with good renal function.3 27 28 Methylcobalamin would be preferable to cyanocobalamin for this purpose.3 27 28
It is surprising that microemboli were more common in patients taking both aspirin and warfarin; we speculate that this may be due to indication bias; that is, patients thought to be at higher risk of emboli may have been prescribed both drugs.
There seemed to be an association of BSA with MES; perhaps this was related to dose of warfarin in relation to body size.
Among vascular risk factors, we found a significantly higher number of MES in current smokers compared with non-smokers. This finding might be explained by effects of smoking on formation of microemboli, or related to carbon monoxide or inflammatory/oxidative stress due to thiocyanate exposure,29 30 or the presence of another central source of emboli, for example aortic plaque. In our study, advanced age was associated with a lower MES count. This is in line with a previous study showing a higher number of MES in children with MHVs as compared with adults.31 Even with adequate oral anticoagulant therapy in patients with atrial fibrillation, hyperhomocysteinaemia increases the risk of cardioembolic events.32 Our study has some limitations. Previous studies showed that MES numbers may be different according to the valve types.33–35 We are not able to comment on the association between valve types and MES count due to a restricted range of different valves. We controlled for valve size according to BSA; however, we did not have access to all haemodynamic characteristics to calculate a valve continuity equation. We also did not thoroughly assess other potential sources of emboli, namely carotid stenosis and aortic arch atheroma; the patients recruited for this study were being cared for by their family physicians and the cardiac surgery team, and were not patients attending our stroke prevention clinic. Only the procedures permitted in the ethics protocol were carried out. Despite the above-mentioned shortcomings, to the best of our knowledge this is the first study evaluating the association between homocysteine and microemboli in patients with MHVs. Our study design, with repeated TCD monitoring, gave us adequate statistical power to perform a detailed comparison between tHcy and the MES number.
Conclusions
In patients with MHVs, higher tHcy was associated with a higher number of both gaseous and solid microemboli. Smokers, particularly women, had more microemboli than non-smokers. This finding indicates the importance of smoking cessation and of measuring tHcy and serum B12 in patients with MHVs. Further prospective studies with a larger sample size are recommended to assess the role of homocysteine and the efficacy of homocysteine-lowering in the prevention of stroke and dementia.
References
Footnotes
Contributors JDS conceived of the study, analysed data, and wrote revisions of the manuscript and the final draft. AM, CB and MAQ recruited patients. AM collected and analysed data. CM performed the transcranial Doppler studies. MRA conducted analyses of the data.
Funding The study was funded by donations to the Stroke Prevention & Atherosclerosis Research Centre, mainly from patients attending the stroke prevention clinics.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The protocol was approved on 20 March 2014 by the Human Subjects Research Ethics Research Board of the University of Western Ontario (protocol number 103490).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data could be provided upon request.