- Lingling Ding,
- Yuehui Hong,
- Bin Peng
- Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (CAMS & PUMC), Beijing, China
- Correspondence to Dr Bin Peng; pengbin3{at}hotmail.com
- Received 15 October 2016
- Revised 26 December 2016
- Accepted 18 January 2017
Abstract
Objective The aim of this systematic review and meta-analysis was to provide evidence that biomarkers of large artery atherosclerosis, including arterial stenosis and greater carotid intima-media thickness (cIMT), may serve as clinical markers of subclinical haemorrhage-prone cerebral small vessel disease, reflected by cerebral microbleeds (CMBs).
Methods We searched PubMed, MEDLINE, Web of Science, EMBASE and the Cochrane Library to identify relevant studies published before 1 July 2016. The association between arterial stenosis and CMBs was estimated by the OR and 95% CI. The association of cIMT and CMBs was calculated using the standardised mean difference (SMD). Heterogeneity and publication bias were explored.
Results 8 studies including a total of 7160 participants were pooled in the meta-analysis. 6 of the included studies were cross-sectional, except that 2 were prospective. We found a significant association between arterial stenosis >50% and the presence of CMBs (OR 1.95, 95% CI 1.13 to 3.36, I2=56.1%). A fixed-effects model suggested that patients with CMBs were more likely to have a greater cIMT (SMD 0.20, 95% CI 0.11 to 0.28, I2=24.7%).
Conclusions This systematic review and meta-analysis found that there is a relationship between large artery atherosclerosis and CMBs. Future studies are needed to confirm the impact of atherosclerosis on the CMBs, which may have potential therapeutic implications.
- cerebral microbleeds
- intima-media thickness
- Atherosclerosis
- arterial stenosis
Introduction
Cerebral small vessel disease (CSVD) contributes to about a fifth of all strokes worldwide, and is considered a major cause of disability and vascular cognitive impairment.1 ,2 Prominent manifestations of CSVD on neuroimaging include white matter hyperintensity (WMH), lacunar infarction, enlarged perivascular spaces and cerebral microbleeds (CMBs).1 ,2 The most common causes of CSVD are diseases that affect the cerebral perforating arteries, arterioles, capillaries and venules. However, recent studies have shown a link between CSVD and the markers of large artery atherosclerosis, including arterial stenosis and greater carotid artery intima-media thickness (cIMT).3–7
Large artery atherosclerosis is considered a systemic and chronic inflammatory disease that may lead to both cardiovascular and cerebrovascular diseases.8 Recent studies found a positive association between large artery atherosclerosis and CSVD.9 To the best of our knowledge, treatments for large artery atherosclerosis such as antihypertensive therapy are also effective in patients with CSVD.10 Although the aetiology and pathogenesis of CSVD remain unclear, large artery atherosclerosis may become a potential therapeutic target for the prevention of CVSD. Therefore, it is meaningful to clarify the relationship between CSVD and large artery atherosclerosis.
CMBs are regarded as small areas of signal loss on T2*-weighted gradient echo (GRE) MRI sequences, pathologically representing bleeding-prone microangiopathies, including hypertensive arteriopathy and cerebral amyloid angiopathy.2 ,11–13 The presence of CMBs is considered a strong predictor of future stroke, particularly haemorrhagic stroke.14 ,15 There is evidence that large artery atherosclerosis may be associated with CMBs, but the results are controversial. Older age, hypertension and diabetes mellitus are common vascular risk factors that have an impact on both large arteries and small vessels.9 Chronic cerebral hypoperfusion could be a mechanism by which CMBs are associated with large artery atherosclerosis.16 ,17 To determine whether an association exists between large artery atherosclerosis and CMBs, we conducted a systematic review and meta-analysis of the literature, hoping that this would throw light on the pathogenesis and therapeutic strategy for CMBs.
Methods
Search strategy
We searched PubMed, MEDLINE, Web of Science, EMBASE and the Cochrane Library to identify relevant studies published before 1 July 2016 using the following search terms: ‘microbleeds', or ‘microhaemorrhage’, or ‘gradient-echo’, or ‘susceptibility weighted imaging’ in association with ‘artery atherosclerosis’, or ‘artery stenosis’, or ‘artery plaques’, or ‘artery calcification’, or ‘carotid intima-media thickness’. Related articles and reference lists from all included articles were also searched to identify additional studies.
Selection criteria
Two independent reviewers selected all studies. Inclusion criteria for the studies were: (1) cross-sectional or longitudinal in design; (2) investigated the association of large artery atherosclerosis and CMBs; (3) artery atherosclerosis including: cerebral artery stenosis >50% (internal carotid artery (ICA) or common carotid artery, intracranial or extracranial arteries) measured by digital subtraction angiography, CT angiography (CTA), MR angiography or carotid duplex ultrasound (CDUS); cIMT measured by CDUS; (4) studies published in English; (5) full paper could be obtained; (6) the participants were humans. Consensus was reached through discussion.
Quality assessment
The quality assessment standards for observational studies were recommended by the Agency for Healthcare Research and Quality (AHRQ). Quality assessments of cohort studies were performed using the Newcastle Ottawa Scale (NOS), and quality of cross-sectional studies was assessed using an 11-item instrument.18 ,19 Two independent researchers evaluated the included studies. Any disagreements were resolved after discussion with another author.
Data extraction
Two authors independently went through each eligible study and extracted information on the following items: first author's name, publication year, study design, sample size, sex and age distribution, prevalence of CMBs, MRI parameters, incidence rate of stenosis >50%, mean cIMT, detection methods, definition of large artery atherosclerosis and other principal findings associated with CMBs (p<0.05). The missing data and information of included studies were obtained by contacting the authors if possible.
Statistical analysis
The association of arterial stenosis and CMBs was estimated by the OR. The association of mean cIMT and microbleeds was calculated using the standardised mean difference (SMD). A random-effects model was employed when heterogeneity was found (p<0.10 or I2 >50%); otherwise, a fixed-effects model was used. The heterogeneity among studies was assessed by the Higgins I2 statistic and Cochran's Q test. An I2 > 50% and (or) a Q test p value <0.10 indicated statistical heterogeneity. Funnel plots and Egger's linear regression test were used to evaluate publication bias. A sensitivity analysis was investigated by omitting a single study in each turn. The meta-analysis was performed using Stata V.14.1 (Stata Corporation LP, College Station, Texas, USA). All p values were two-sided and p<0.05 was considered statically significant. We prepared this report according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) proposal.20
Results
Selection process and study characteristics
A total of 339 studies were identified. Case reports, letters and reviews were excluded. Only 42 studies were included for review of the full text based on the titles and abstracts. Of these, 34 were subsequently excluded: no stenosis>50% or mean cIMT reported (n=20), no CMBs rate reported (n=5), no study of association between large artery atherosclerosis and CMBs (n=2), no control group (n=4), not cross-sectional or longitudinal in design (n=3). Finally, eight studies including a total of 7160 participants were pooled in this meta-analysis (figure 1).21–28 Four of the eight studies reported an incidence rate of stenosis>50%,23–25 ,28 and four studies reported mean cIMT.21 ,22 ,26 ,27 Six of the included studies were cross-sectional, except that two were prospective.27 ,28 The main characteristics of included studies are shown in table 1.
Characteristics of included Studies

Flow chart of the study selection process. cIMT, carotid intima-media thickness; CMBs, cerebral microbleeds.
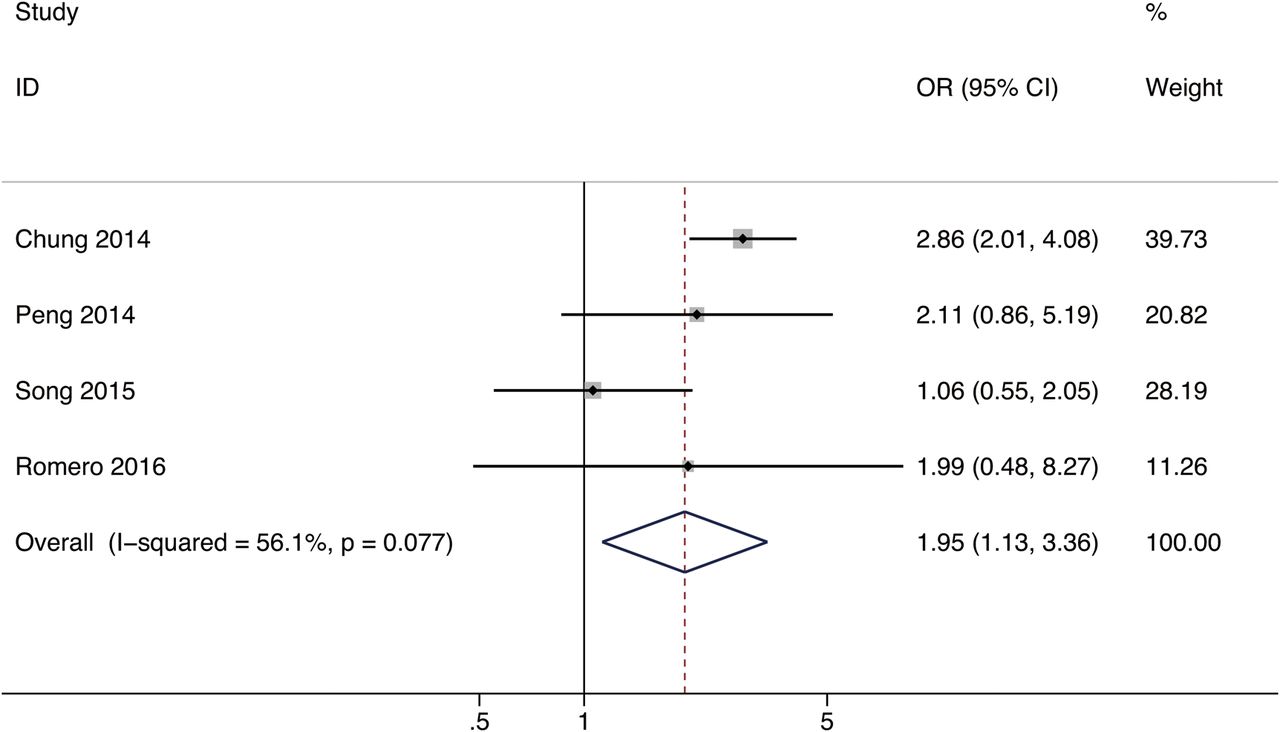
Four studies including a total of 2387 patients were pooled in the meta-analysis of the association between large artery stenosis and CMBs.23–25 ,28 The mean age of the study participants was 61.4 years (range, 56.9 to 66.8 years). The overall prevalence of CMBs on MRIs was 21.4% (range, 8.2–40.2%). ORs (95% CI) and adjustments are reported in table 2. Only one study demonstrated a significant relationship between cerebral large artery stenosis and CMBs presence.23 We calculated the pooled OR by most adjusted OR using a random-effects model. The combined OR was 1.95 (95% CI 1.13 to 3.36) for the association between large artery stenosis >50% and CMBs (figure 2).
ORs of studies included in the meta-analysis

Forest plot for the association between large artery stenosis and CMBs. CMBs, cerebral microbleeds.
Risk of bias and heterogeneity between studies
The I2 statistics and Cochran's Q test indicate evidence of substantial heterogeneity among studies (p=0.077, I2=56.1%). Furthermore, visual inspection of the funnel plot and Egger's test (p=0.48) indicated no evidence of publication bias.
We conducted a sensitivity analysis by excluding a single study each time to explore the robustness of the combined results. The range of the combined ORs was from 1.41 (95% CI 0.86 to 2.32) to 2.70 (95% CI 1.96 to 3.72). The result showed no significant relationship between large artery stenosis >50% and CMBs presence when excluding Chung's study,23 with an OR 1.41 (95% CI 0.86 to 2.32). The I2 statistics and Cochran's Q test indicated the reduction of heterogeneity (p=0.423; I2=0.0%). This absolute difference may be due to different detection methods. First, Chung et al23 used CTA to detect the degree of intracranial ICA stenosis; however, three other studies mainly defined arterial stenosis by ultrasound scan, which might lead to heterogeneity. Second, the incidence rate of CMBs in Chung's study was much higher than in other studies. Chung et al assessed CMBs on susceptibility-weighted imaging (SWI), which is more sensitive. This may explain part of the heterogeneity.
Association between cIMT and CMBs
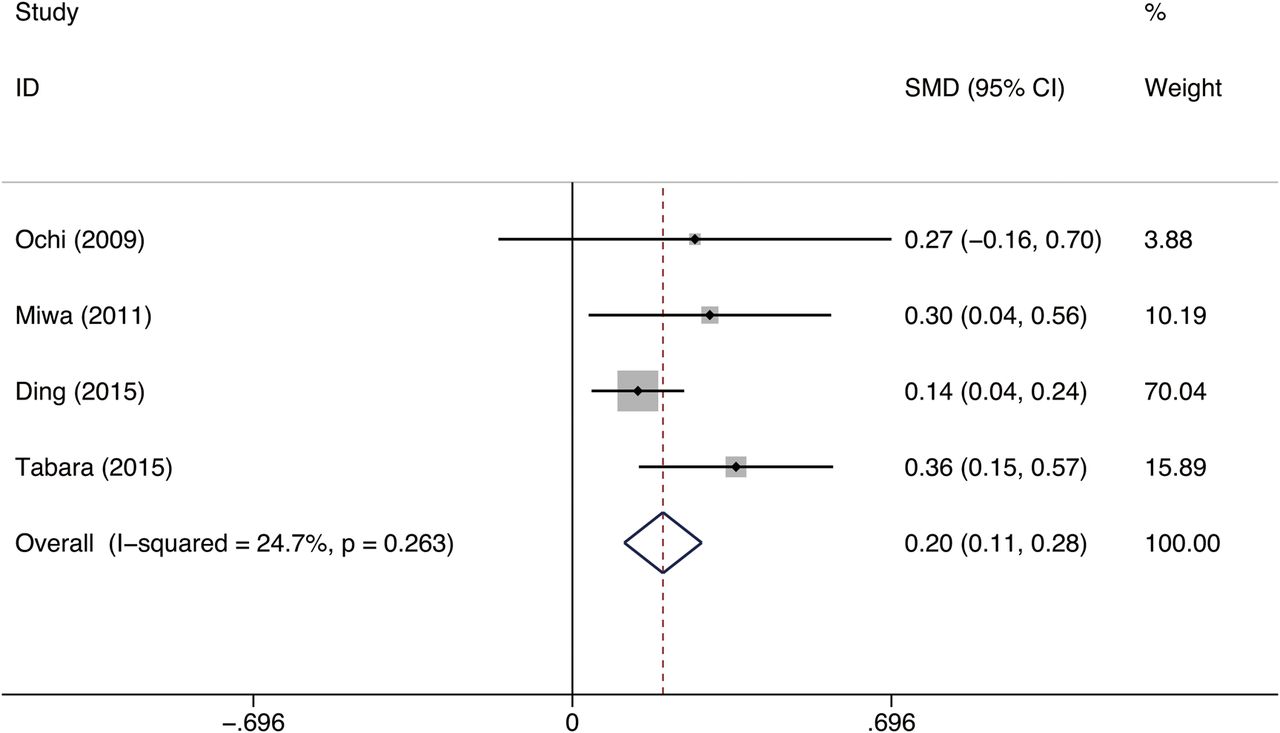
Four studies including 4773 patients provided data on the association between mean cIMT and CMBs were pooled in the meta-analysis.21 ,22 ,26 ,27 The mean age of the study participants was 71.2 years (range, 67 to 74.6 years), with fewer participants being men (41.3%; range, 39.4–52%). The overall prevalence of CMBs on MRI was 13.5% (range, 5% to 18.4%). A fixed-effects model was applied to estimate a pooled SMD of 0.20 (95% CI 0.11 to 0.28), which demonstrated that patients with CMBs were more likely to have a higher cIMT (p<0.001; figure 3). Three of the four studies demonstrated a statistically significant association between cIMT and cerebral microbleeds. Only one study found no association between cIMT and CMBs in healthy individuals free from a history of stroke.21

{kind=link}
{kind=link}
{kind=link}
Forest plot for the association between cIMT and CMBs. cIMT, carotid intima-media thickness; CMBs, cerebral microbleeds; SMD, standardised mean difference.
Risk of bias and heterogeneity between studies
The I2 statistics and Cochran's Q test indicate low heterogeneity (p=0.263; I2=24.7%). A funnel plot and Egger's test were used to assess the publication bias. The funnel plot seemed asymmetric, and the asymmetry was detected by Egger's test (coefficient=1.59, p=0.23). This demonstrated that asymmetry of the funnel was unlikely due to publication bias.
A sensitivity analysis was performed through excluding a single study each time. The result by excluding one study showed an increased SMD borderline (SMD 0.326, 95% CI 0.17 to 0.48), with no heterogeneity (p=0.909; I2=0.0%), because of the greater weight in this study.27 However, this did not change the outcome statistically. The analysis was consistent when using a random-effects model.
Discussion
CSVD is an important public health problem that has attracted increasing attention, and may coexist with large artery atherosclerosis.9 The aim of this systematic review and meta-analysis was to provide evidence that biomarkers of large artery atherosclerosis, such as greater cIMT and arterial stenosis, may serve as clinical markers of subclinical haemorrhage-prone CSVD, reflected by CMBs. Previous studies have suggested that the incidence rate of CMBs in patients with large artery atherosclerosis was 9–41.3%.24 ,28 ,29 Different populations and detection methods may lead to different incidence of CMBs. Kwon et al reported 14 of 313 patients (9.0%) with intracranial arterial stenosis (ICAS) presented with CMBs on baseline MRI in the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial. However, they found no evidence linking CSVD with an increased risk of stroke in patients with ICAS.29
Large artery atherosclerosis and CSVD may share disease mechanisms, which are likely to be mediated via common vascular risk factors, such as older age, hypertension and diabetes mellitus.29 The prevalence of CMBs gradually increased with age.30 Advanced age and long-term hypertension may cause structural changes in microvessels, represented by fibrinoid necrosis and lipohyalinosis, thus increasing the risk of rupture and bleeding.31 Histopathological analyses have found hypertensive vasculopathy was specially associated with CMBs in the thalamus, basal ganglia, brainstem and cerebellum.32 Otherwise, Qiu et al33 indicated that diabetes was associated with markers of both cerebral macrovascular and microvascular diseases. Older age, hypertension and diabetes mellitus are risk factors that may lead to large artery atherosclerosis, thus giving rise to CMBs.
Previous studies have found that carotid stenosis, carotid plaque and cIMT were likely to be associated with WMH and cognitive decline in elderly people, even after accounting for vascular risk factors.7 ,34 In addition to the common risk factors, other mechanisms may explain the correlation. Factors that may influence cerebral blood flow especially at the origin of perforator arteries may also be involved. Gregg et al16 reported that the presence of incidental cortical CMBs is associated with significant and widespread reduction in resting-state cerebral blood flow (CBF), especially in the frontal, parietal and precuneus cortices. Moreover, Hashimoto et al17 found reduced CBF in the centrum semiovale in patients with five or more CMBs compared with those with <5 CMBs in patients with CSVD. Individuals with cortical or deep or infratentorial CMBs may be exposed to chronic cerebral hypoperfusion.16 ,17 ,35 Long-term hypoperfusion could accelerate the development of age-related ultrastructural aberrations of capillaries and cause blood-brain barrier (BBB) damage.36 ,37 Disruption of BBB has been suggested as a main initial pathogenic mechanism in CSVD.22 ,24 However, another possibility is that both CMBs and hypoperfusion are markers of small vessel diseases, and that no causal relationship between them should be considered. Further studies are needed before a conclusion can be drawn.
In this meta-analysis, we found a significant association between large artery stenosis and microbleeds in the included studies, with an OR 1.95 (95% CI 1.13 to 3.36). The results from the Framingham Heart Study demonstrated that carotid stenosis ≥25% was associated with presence of CMBs overall (OR 2.20, 95% CI 1.10 to 4.40), especially at deep and mixed locations (OR 3.60, 95% CI 1.23 to 10.5). Paradoxically, the study found that carotid stenosis ≥50% was not associated with CMBs. The study observed carotid stenosis ≥50% in only 1.5% of 1243 participants and the incidence rate of CMBs was 8.3%, which might be an underestimate.28 The evidence relating arterial stenosis to CMBs was inconsistent. This may be attributed to different inclusion criteria, different sample size, differences in demographic characteristics and different methodology for cerebral artery stenosis estimation. Some of the included studies defined arterial stenosis by ultrasonography, which may limit accuracy. In our study, we found evidence that arterial stenosis >50% was related to the incidence of CMBs. Large artery stenosis may lead to hypoperfusion, thus resulting in CMBs. Further research is needed for confirmation.
There may be other potential mechanisms that cause CMBs in patients with large artery atherosclerosis. CIMT is a non-invasive ultrasound marker of early atherosclerosis, and is increasingly used as a predictor of future clinical cardiovascular events including myocardial infarction and stroke.38–40 Previous studies considered cIMT as a marker of large-artery damage rather than CSVD. The Second Manifestations of Arterial disease study showed that mean cIMT was greater in patients with large vessel disease (1.08 mm) than in those with small vessel disease (0.92 mm) (SMD 0.11 mm, 95% CI 0.05 to 0.18).41 However, new research showed that patients with CSVD had greater cIMT compared with normal participants.42 The present systematic review and meta-analysis identified four studies focusing on the relationship between cIMT and CMBs. The result demonstrated that patients with CMBs were more likely to have a greater cIMT (SMD 0.20, 95% CI 0.11 to 0.28). Ding et al27 conducted a prospective population-based cohort study that included individuals aged >65 years without dementia and found that an increase in mean cIMT as a marker of arterial atherosclerosis was associated with an increased risk of CMBs, especially in the deep and infratentorial brain regions. All these findings suggest that there is a significant relationship between higher cIMT and CMBs risk.
One of the included studies in this review also explored the relationship between inflammation and CMBs in addition to increased cIMT. The results indicated that higher levels of circulating inflammatory markers, such as high-sensitivity C reactive protein (hsCRP), interleukin-6 (IL-6) and IL-18 were associated with CMBs, suggesting the involvement of inflammation.22 Inflammation is also implicated in the pathogenesis and development of atherosclerosis. Several studies have demonstrated that high levels of some inflammatory cytokines are important determinants in the pathogenesis of increased cIMT. Patients with higher cIMT have increased circulating levels of fibrinogen, tumour necrosis factor α, white cell count, hsCRP and IL-6.43 ,44 Moreover, Chung et al45 detected underlying intracranial atheroma in 60% of patients with lacunar infarction by high-resolution MRI and found potential intraplaque inflammation, suggesting the involvement of inflammation in both cerebral artery atherosclerosis and CSVD. We speculated that the link between CMBs and large artery atherosclerosis might be inflammation. Further studies are needed to confirm these findings.
There were some limitations in our study. First, only studies published in English were included, which may introduce publication bias. Second, the participants in the cross-sectional studies were consecutive patients, which may have introduced selection bias. Third, some of the studies were subject to bias because they did not involve blinded assessment of large artery atherosclerosis or blinded identification of CMBs. Fourth, the included studies varied in many aspects, such as study population, which resulted in a wide range of CMBs incidence rate (5% to 40.2%). Fifth, only one study demonstrated a significant relationship between cerebral large artery stenosis >50% and CMBs,23 using CTA to define arterial stenosis. The included studies used CDUS or transcranial Doppler to detect arterial stenosis may introduce bias due to limited accuracy. Moreover, most of the included studies assessed CMBs using T2*GRE or 1.5 T MRI machines. The use of higher-field MRI and SWI are known to increase CMBs detection. The variety of different techniques used in the assessment of artery atherosclerosis or CMBs in the included studies should be considered a source of heterogeneity. The accuracy of the methodology needs to be established in future studies.
Conclusions
In conclusion, the results of this systematic review and meta-analysis suggest that there is a relationship between large artery atherosclerosis and CMBs. Whether the occurrence of CMBs in patients with large artery atherosclerosis can predict the future risk of haemorrhagic cerebral vascular events is unclear. Longitudinal studies in larger populations are needed to confirm the impact of atherosclerosis on the bleeding-prone CMBs, which may have potential therapeutic implications.
Footnotes
Contributors BP designed the study, and revised the manuscript. LD collected and extracted data, and drafted the manuscript. YH collected and extracted data.
Funding This work was supported by the National Natural Science Foundation of China (grant number 81471206) and the Beijing Natural Science Foundation (grant number 7152121).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/