Article Text

Abstract
Background Acute vestibular syndrome (AVS) features continuous dizziness and may result from a benign inner ear disorder or stroke. The head impulse-nystagmus-test of skew (HINTS) bedside assessment is more sensitive than brain MRI in identifying stroke as the cause of AVS within the first 24 hours. Clinicians’ perspectives of the test in UK secondary care remains unknown. Here, we explore front-line clinicians’ perspectives of use of the HINTS for the diagnosis of AVS.
Methods Clinicians from two large UK hospitals who assess AVS patients completed a short online survey, newly designed with closed and open questions.
Results Almost half of 73 total responders reported limited (n=33), or no experience (n=19), reflected in low rates of use of HINTS (n=31). While recognising the potential utility of HINTS, many reported concerns about subjectivity, need for specialist skills and poor patient compliance. No clinicians reported high levels of confidence in performing HINTS, with 98% identifying training needs. A lack of formalised training was associated with onward specialist referrals and neuroimaging (p=0.044).
Conclusions Although the low sample size in this study limits the generalisability of findings to wider sites, our preliminary data identified barriers to the application of the HINTS in AVS patients and training needs to improve rapid, cost-effective and accurate clinical diagnosis of stroke presenting with vertigo.
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Acute vestibular syndrome (AVS) presents with ‘continuous’ vertigo lasting more than 24 hours, associated with nystagmus and often with nausea, vomiting and head motion intolerance.1 2 The head impulse-nystagmus-test of skew (HINTS) test is a three-step bedside oculomotor assessment,3 which has 100% specificity and 96% sensitivity for stroke in specialist units when undertaken by trained neurologists and neuro-otologists.4 The HINTS assessment is reportedly superior to a brain MRI in the first 24 hours in AVS patients.3 In the UK, however, its uptake in emergency departments (ED) is low.5 Quimby et al 6 attributed this low usage to lack of awareness of the test and/or low physician confidence in performing and interpreting the HINTS assessment. However, UK front-line clinicians’ perspective on the use of HINTS has never been explored. Such knowledge is essential for validating this assessment in relevant settings.
To address this knowledge gap, this study explores clinicians’ perspectives on the use of HINTS in two UK National Health Service (NHS) hospitals.
Methods
This study used a cross-sectional online survey (Online Surveys. Jisc, UK) to explore clinicians’ perspectives of HINTS. The eligibility criteria were as follow: state registered qualified healthcare professionals (eg, General Medical Council, The Health and Care Professional Council, The Nursing and Midwifery Council) who assessed a patient with AVS in the last 6 months (time frame chosen to assist with information recall). The targeted clinicians worked in the following settings: ED, neurology (acute medical unit) and stroke (hyperacute stroke unit) wards. These settings were chosen as those most likely exposed to AVS patients. Following communications with the department leaders it was estimated that a total sample of 297 potential clinicians from two urban NHS Trusts were eligible respondents (hospital A, n=80 and hospital B, n=217). A total sample size of 73 was recommended to generate 95% confidence level and 10% margin of error. Convenience sampling was used, with department leaders disseminating the survey to eligible team members.
We designed and validated a survey to evaluate the study aim. Subcategories captured demographic information, experience of assessing patients with AVS, training and perceived confidence related to the use of HINTS. The survey was launched in February 2020 and was live for 6 weeks at Hospital A and 3 weeks at hospital B (closed early to avoid staff burden during the COVID-19 pandemic). Reminders were sent out at 1, 2 and final weeks of live periods.
Data were exported from Online Surveys to IBM SPSS statistics V.27.0 software for analysis. Responses from closed questions were analysed descriptively and Pearson’s χ2 test explored associations within the data. Two independent researchers explored open response sections using content analysis.
Results
Seventy-eight surveys were returned (five were excluded as they reported no experience of AVS). We analysed 73 surveys (hospital A, n=21 and hospital B, n=52). The majority of the respondents were physicians (n=51, 70%), the remainder were therapists (n=15, 20.5%), nurses (n=6, 8.2%) and a physician associate (1.3%). Multiple work settings were reported with the majority in the ED and acute medical unit (n=36, 49%), neurology (n=28, 38%) or stroke wards (n=38, 52%).
Experience and use of HINTS
Twenty-six per cent of respondents (n=19) reported having no experience of performing HINTS and 43% (n=31) reported no use of HINTS. Forty-three respondents (60%) reported experience of using the test (of which 58%, n=42 reported use in the last 6 months). However, 46% (n=33) of those reporting experience with HINTS rated this as ‘limited’ and only 14% (n=10) reported consistent use of HINTS in the last 6 months. Seven consultants (4 neurologists, 3 ED) do not use/had never heard of HINTS.
Training
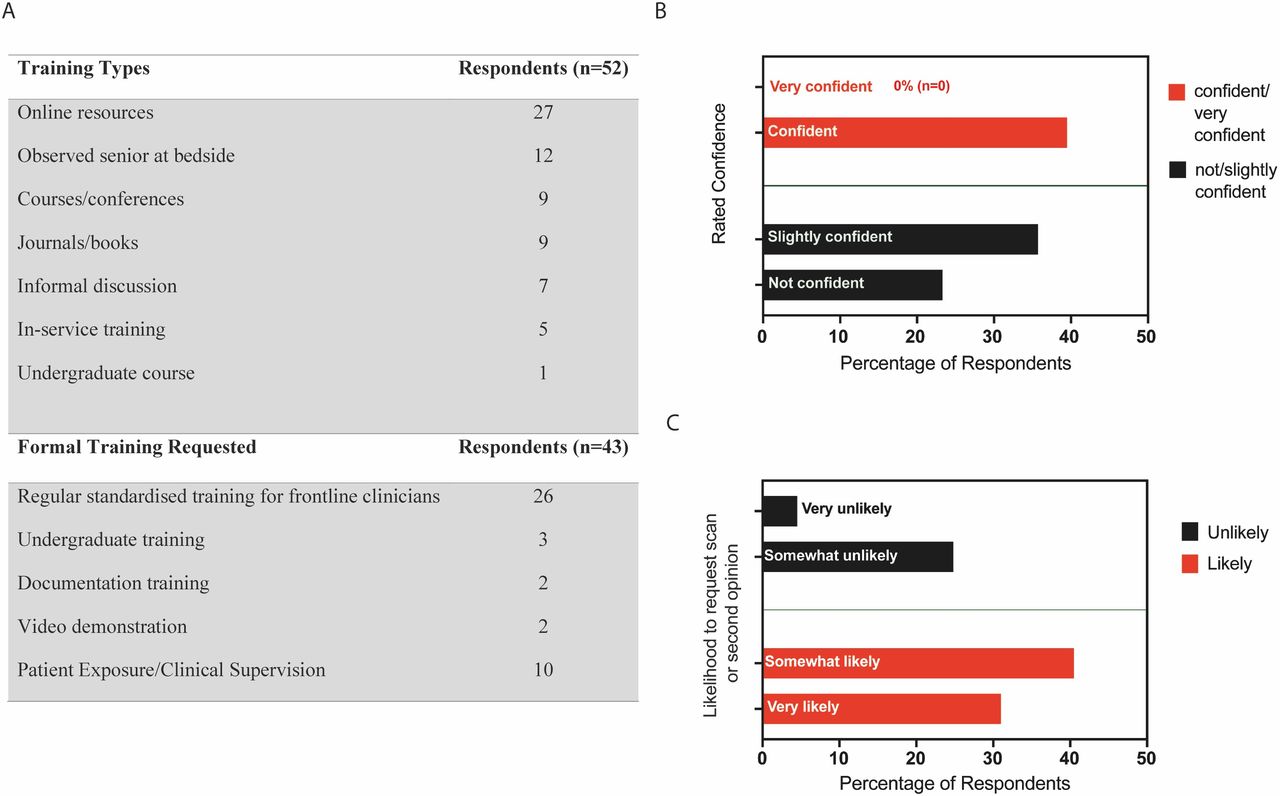
Twenty-nine per cent (n=21) reported no training on HINTS. Seventy-two per cent (n=52) described some element of training, which was self-directed in 35 respondents (figure 1A). Almost all respondents (98%, n=71) reported requiring further training on HINTS to increase confidence, knowledge and expand scope of practice, quoting a need for formal, standardised training (n=29) and clinical exposure (n=10; figure 1A).

{kind=link}
(A) Training types that respondents have used for learning and performing HINTS assessment, and types of formal training that respondents requested. (B) The perceived confidence of performing HINTS (n=42). Note that no respondent was ‘very confident’, with the majority rating themselves as being ‘not or slightly confident’. (C) The likelihood to request further investigation even if no central pathology was suspected when using HINTS (n=42). Most participants were somewhat or very likely to request a scan or second opinion. HINTS, head Impulse-nystagmus-test of skew.
Advantages and disadvantages
Fifty-eight per cent (n=42) of respondents identified advantages associated with the use of HINTS: Its evidence-based status, use as a bed-side test, speed and ease of administration and potential to avoid further investigation or specialist referrals. However, 42% (n=31) encountered barriers to use: some patients were unable to tolerate the assessment, it required a skilled operator, involved subjectivity of assessment and inaccuracies when assessing nystagmus in elderly patients. Nineteen per cent (n=14) of respondents reported barriers to the application and analysis of the head impulse subsection, describing patient intolerance (heightened anxiety, arthritic necks, symptom provoking) and excessive blinking as key factors.
Confidence with HINTS
Of those 42 respondents who had used HINTS in the last 6 months, 15 reported being ‘slightly confident’ and 17 ‘confident’ (of which 12 were consultants: 6 stroke, 2 neurology, 4 ED). None felt ‘very confident’ at performing the test (figure 1B).
Use of imaging/specialist review in AVS
The majority of the sample (72%, n=30) who used HINTS in the last 6 months reported they would be ‘very’ or ‘somewhat likely’ to request further investigations (figure 1C). Reasons for this included a lack of confidence, standard procedure/associations with risk factors, fear of litigation and in response to a patient’s underlying concern.
Inferential analysis
There was a significant association between professional grade of doctors and responses regarding the use of HINTS in the last 6 months (χ2 (df:2, n=51)=8.153, p=0.017) and overall experience of HINTS (χ2 (df:2, n=51)=8.855, p=0.012).
Those that received training were more likely to use HINTS in clinical practice (χ2 (df:3, n=73)=42.403, p<0.001). Clinicians whose training was self-directed were more likely to rely on imaging and specialist opinion, compared with those that received formal training or clinical supervision (χ2 (df:1, n=42)=5.536, p=0.044).
There was no association between the two NHS Trusts and clinician’s experience of HINTS (χ2 (df:2, n=73)=1.277, p=0.528), use of HINTS (χ2 (df:2, n=73)=4.517, p=0.105) or training (χ2 (df:2, n=73)=0.552, p=0.759).
Discussion
Despite the global uptake of HINTS following reports of its ability to diagnose stroke accurately and quickly in subpopulations of those with AVS,3 over a quarter of our respondents reported no experience of HINTS and no respondent perceived themselves as ‘very confident’ in its use. This is consistent with US data,7 suggesting a global issue impacting on the uptake of HINTS.
Dizziness can be diagnostically complex8 and while the HINTS assessment could accurately identify stroke in patients with acute vertigo, only 29% of the respondents had been trained in its use, with training mostly comprising internet-based self-directed study. During the COVID-19 pandemic, restricted physical contact and prohibited group training has precipitated an increased demand for online educational platforms, despite concerns regarding quality of resources available.9 Indeed, we observed that respondents using self-directed training were more likely to rely on imaging or specialist review rather than sole use of the HINTS.
The Care Professions Council training standards, recognise that learning a new clinical skill requires theory and practical teaching, with support from experts.10 With 98% reporting further training needs, formalised HINTS training programmes with practical elements appear necessary to ensure clinical competence and confidence.
While HINTS was generally deemed to be easy to administer, concerns were identified in its application with elderly patients and the head-impulse subsection. Challenges when diagnosing acute vertigo in the elderly, partially due to a deterioration in the oculomotor system, are reported in the wider evidence base.11 With a high prevalence of both benign dizziness and strokes in the elderly population12 this assessment challenge and associated risk of inaccurate HINTS scores could be a frequently encountered problem. Adaptations to testing, such as video-oculography, used to assist with objective head impulse subscoring, could improve accuracy if feasible to use.13
Limitations and future research
Due to time constraint, district general hospitals were not included in this study. Therefore, it may be of benefit to produce a larger scale study involving multiple NHS trusts, to increase the generalisability.
Training needs were evident with a clear lack of regular, formalised teaching programmes on HINTS. Currently, there is paucity in the literature on training programmes with small samples and targeted specialist roles.14 Further research is required on the impact of a large-scale training programmes, to support front-line staff with AVS assessments and measure the potential impact on patient outcomes and healthcare costs. Following training the sensitivity and specificity of HINTS in AVS patients when performed by non-specialist clinicians needs to be investigated. In addition to training, frequent exposure to HINTS implementation and support from a teleconsultant may increase the applicability of this assessment for acute vertigo.15
Respondents highlighted barriers with HINTS with subjectivity, the need for specialist operators, assessment errors and poor patient compliance. With the growing advances in healthcare technology,8 it would be useful for future research to trial the feasibility of video-oculography with front-line clinicians to support assessment of patients with AVS and minimise the barriers highlighted. In addition, qualitative studies are needed to assess confidence of clinicians on performance and interpretation of HINTS.
This study is limited to be the small sample size that was affected by the COVID-19 pandemic, particularly in hospital B (the urban-capital site which was under significant strain), coincident with the roll-out of the questionnaires. While our sample size of 73 was sufficient for this study with a 95% CI and 10% margin of error, we acknowledge that the generalisability of findings to wider sites remains limited.
Conclusion
We identified a reliance on neuroimaging and associated low confidence in performing and interpreting a HINTS assessment of AVS. This is despite a compelling evidence base for superiority of HINTS compared with traditional assessment that can lead to false-negative results and misdiagnosis.3 The underutilisation of a valid and reliable bedside assessment indicates the need for clearer clinical guidelines and training in the assessment of acute vertigo.
Ethics statements
Patient consent for publication
Ethics approval
The Health Research Authority’s (HRA) and Capacity and Capability departments at UCLH and NBT (formerly Research and Development Departments). As this study did not involve patients and was of a non-contentious nature, approval through an NHS Research Ethics Committee (REC) was not required. Further ethical approval was required from the Faculty of Health’s Research Ethics and Integrity Committee. Approval was gained prior to the study commencement and was received on (31 January 2020) IRAS number 274627, FREIC reference 19/20–530.
Acknowledgments
We would like to thank the NHS healthcare professionals who completed the survey.
Footnotes
JF and DK are joint senior authors.
Twitter @CBneurophysio, @LisaBunnPT, @DiegoKaski
Contributors Study concept and design: CLW, DK, LB, JF. Data collection: CLW. Drafting the manuscript: CLW, LB, NK, GS, JF and DK. Data interpretation: CLW, LB, NK, GS, JF and DK. Critical revision of the manuscript: CLW, LB, NK, GS, JF and DK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.