Article Text

Abstract
Background Timely delivery of intravenous tissue plasminogen activator (IV-rt PA) is pivotal to eligible patients who had a stroke while achieving higher rates of IV-rt PA has been problematic. This paper focuses on investigating influential factors associated with the administration of IV-rt PA, primarily per capita gross regional product (GRP) and healthcare system factors.
Methods The study included 980 hospitals in the Chinese Stroke Center Alliance where 158 003 patients who had an acute ischaemic stroke received IV-rt PA between August 2015 and August 2019. The adherence rate to IV-rt PA within 4.5 hours time window in each hospital was the primary outcome. Influential factors were grouped into two categories: macroeconomic status and hospital characteristics. The outcome was analysed using multivariable linear regression.
Results GRP per capita (β=2.37, p<0.001), hospital stroke centre certification (β=3.77, p<0.001), number of neurologists (β=0.12, p<0.001), existence of emergency services for neurological treatment (β=7.43, p=0.014), presence of emergency department (β=10.03, p=0.019) and cooperating with emergency centre (β=4.65, p=0.029) were significantly positively associated with the adherence rate to IV-rt PA.
Conclusions Higher GRP per capita, affluent neurological personnel, well-equipped emergency services for neurological treatment and routine cooperation with the emergency centre were important for enhancing the adherence rate to IV-rt PA among patients who had an acute ischaemic stroke in China.
- stroke
- thrombolysis
- statistics
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Stroke is the second leading cause of death in the world and the leading cause of death in China, the country alone accounting for roughly one-third of worldwide stroke mortality,1 2 with escalating cost to the healthcare system.3 Thrombolysis using intravenous tissue plasminogen activator (tPA) is one of the few evidence-based acute stroke treatments.4 5 Adherence to IV-rt PA is pivotal to the treatment for patients who had an acute ischaemic stroke (AIS): treatment with intravenous tPA within 4.5 hours of the stroke onset significantly improves clinical outcomes at 3 months.4 6
Although the overall quality of stroke care has significantly improved in China, there was no significant improvement in the adherence rate of IV-rt PA (14.1% in 2007–2008 vs 18.3% in 2012–2013), which remained significantly lower than that in the Get With The Guidelines-Stroke (GWTG-Stroke) programme (72.8% in 2007).7 8 Potential reasons for the low rate include prehospital delay, lack of regional stroke care network, high cost of tPA, low insurance coverage and concern about haemorrhagic risk.7 Significant opportunities still exist for further improvement.7
A recent meta-analysis has summarised what healthcare system factors contributed to the improvement of the thrombolysis rate,3 including travel time and location9–11 (eg, urban rather than rural location or a centralised/‘hub’ model linking outlying centres with other, generally larger, centres), training, skills and expertise11 12 (treatment by a neurologist or in a neurology department; admission to a stroke unit; treatment at a hospital with higher volume of stroke admissions or neurology beds; or accreditation as a ‘medical centre’), facilities and staffing11 13–17 (having a neurologist, stroke nurse or a stroke team; neurological or neuroimaging services; and weekend arrival) and organisational elements14 17 18 (use of stroke-specific protocols or transfer by ambulance/mobile emergency team rather than other means). However, detailed empirical data regarding the effects of such factors are not available.
Anecdotal studies mainly focused on the potential effect of individual-level socioeconomic status (SES) on the delivery of IV-rt PA, with conflicting observations. Wang et al claimed that patients with higher income were nearly twice as likely to receive IV-rt PA in China using the Chinese National Stroke Registry (CNSR) data.19 Ader et al observed that SES wasn’t associated with tPA administration among patients in the USA.20 It remains unclear how socioeconomic factors are associated with adherence rate of IV-rt PA. To the best of our knowledge, there are no published empirical studies that explore how macroeconomics and hospital-level factors associate with the adherence rate to IV-rt PA in China.
We aim to study the above research question, leveraging the natural imparity of social and economic development across China. Following previous quality improvement initiatives, such as the GWTG-Stroke programme, the Chinese Stroke Association initiated the Chinese Stroke Center Alliance (CSCA) in June 2015, as the national hospital-based stroke care quality assessment and improvement platform.21 Using data from the CSCA, we sought to identify how regional economic development and healthcare system factors were associated with adherence rate to IV-rt PA among eligible patients treated ≤4.5 hours from symptom onset.
Methods
Data collection
Hospital data were collected from the database of the CSCA, a national, hospital-based, multicentre, voluntary, multifaceted intervention and continuous quality improvement initiative,21 via a web-based data collection and management tool (Medicine Innovation Research Center, Beijing, China). Details of the CSCA programme have been previously described elsewhere.21 All participating hospitals received research approval to collect data without requiring individual patient informed consent under the common rule or a waiver of authorisation and exemption from their institutional review board.
Outcome measure
The primary outcome was the adherence rate to IV-rt PA in each hospital. To determine the adherence rate, for each hospital in our study, we considered those patients that are eligible for IV-rt PA, and are without any medical contraindications (eg, treatment intolerance, excessive risk of adverse reaction, patient/family refusal or terminal illness/comfort care only),21 and calculated the proportion of those that received the treatment within 4.5 hours.
Factors
We grouped the influential factors into two categories: macroeconomic status and hospital characteristics (healthcare system factors).
Macroeconomic status
We determined the macroeconomic status of each hospital using the hospital’s province per capita gross regional product (GRP), collected from the Statistical Yearbook published by the National Bureau of Statistics of China.22 As documented in the existing literature, GRP is conceptually equivalent to gross domestic product and measures newly created value through production by regional production unit (‘province’ in this study).23
Hospital characteristics (healthcare system factors)
Hospital characteristics were classified into three aspects following the meta-analysis. The list of variables was selected by clinicians and statisticians based on experience and previous model fitting. We characterised a hospital’s training skills and expertise by AIS volume; hospital level (1 if the hospital is a tertiary hospital and 0 if the hospital is a secondary hospital); presence of stroke certification (1 if the hospital is a comprehensive stroke centre (CSC); 0 if the hospital is a primary stroke centre (PSC)); teaching status (1 if the hospital has a medical school affiliation; otherwise, 0); whether a hospital has a neurology department or not (1 if the hospital has one; otherwise, 0); whether a hospital is equipped with stroke units or not. Hospital facility and staffing were proxied by whether a hospital has an emergency department (ED) or not; the number of beds in the neurology department; whether a hospital has neurologists or not; the number of beds in the ED; whether a hospital has stroke nurses or not; whether a hospital has a stroke team or not; whether a hospital provides emergency services for thrombolytic treatment for patients who had an AIS or not; the number of neurologists, the number of thrombolytic specialists; the number of neuroimaging services (CT and MRI; the number of stroke allocated beds (the fixed number of beds for neurological treatment in the ED). In addition, we included whether a hospital has cooperation with the emergency centres or not, whether a hospital has stroke-specific protocols as proxies for organisational elements. All variables had a low rate of missing data (<3%) except for the number of beds in the ED (4.2%).
Statistical analysis
To assess what factors might be associated with adherence rate of IV-rt PA, we first calculated quartiles of the hospital adherence rate, and then grouped the hospitals according to the quartiles. Within each adherence rate quartile, we calculated summary statistics of hospital characteristics.
Multivariable linear regression was used to identify the effect of each factor. For multivariable analysis, all factors were included in the same model and a backward stepwise approach was implemented for variable selection to obtain a parsimonious model. The results of the regression were presented as the beta coefficients ( β ), describing the magnitude and directionality of change in the dependent variable for every 1-unit change in the independent variable. The standardised beta coefficients (standardised β ) were used to compare the effect of each factor to the adherence rate after scaling the different units of the factors. P<0.05 was used as the significance level. Statistical analyses were performed with the R software (V.3.6.3).
Results
We studied a total of 980 unique hospitals, with 158 003 patients from 31 provinces in China, with the exception of Hong Kong SAR, Macau SAR and Taiwan, between August 2015 and August 2019.
Figure 1 illustrates the location of the CSCA hospitals, along with the IV-rt PA adherence rate quartiles and the GRP per capita level. As seen on the map, the hospitals achieving high adherence rate generally located in the high-GRP per capita areas, with a few exceptions.
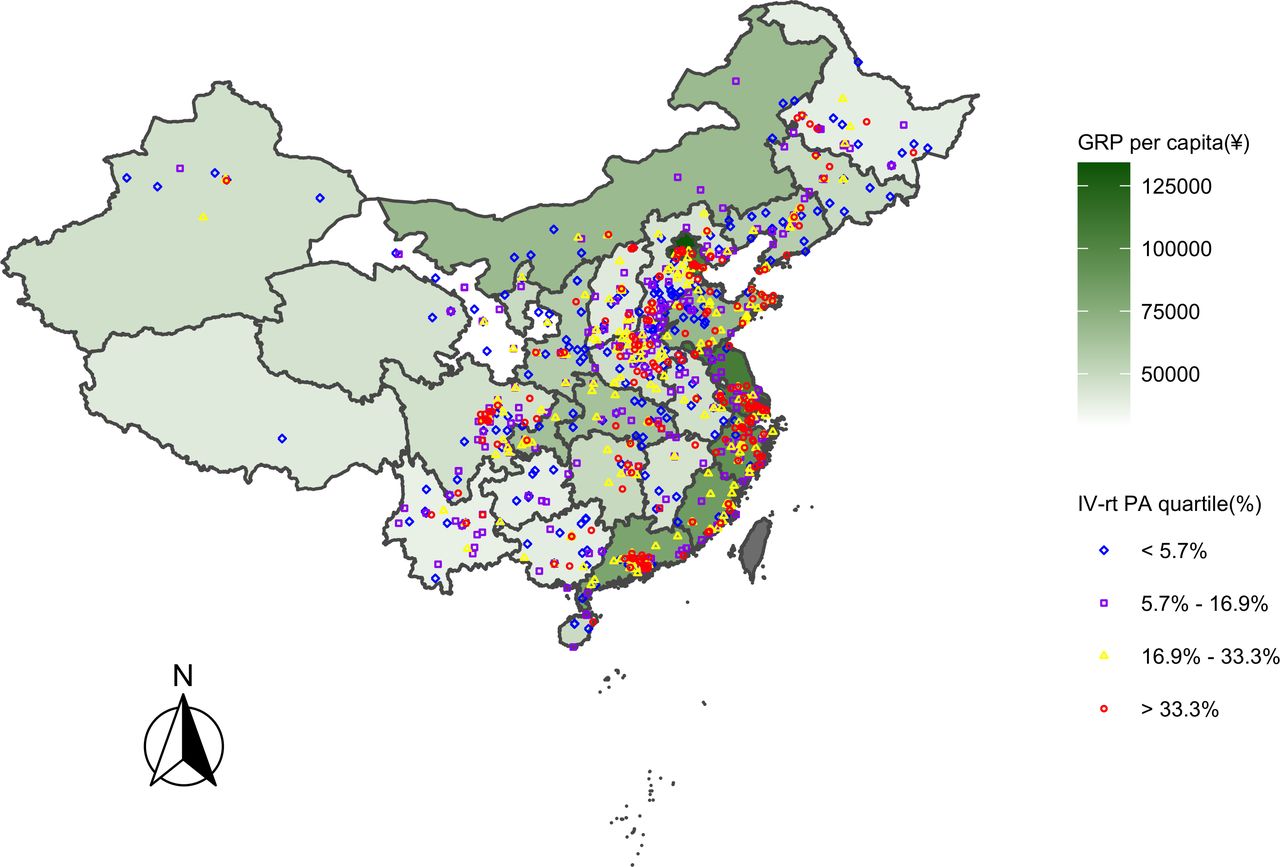
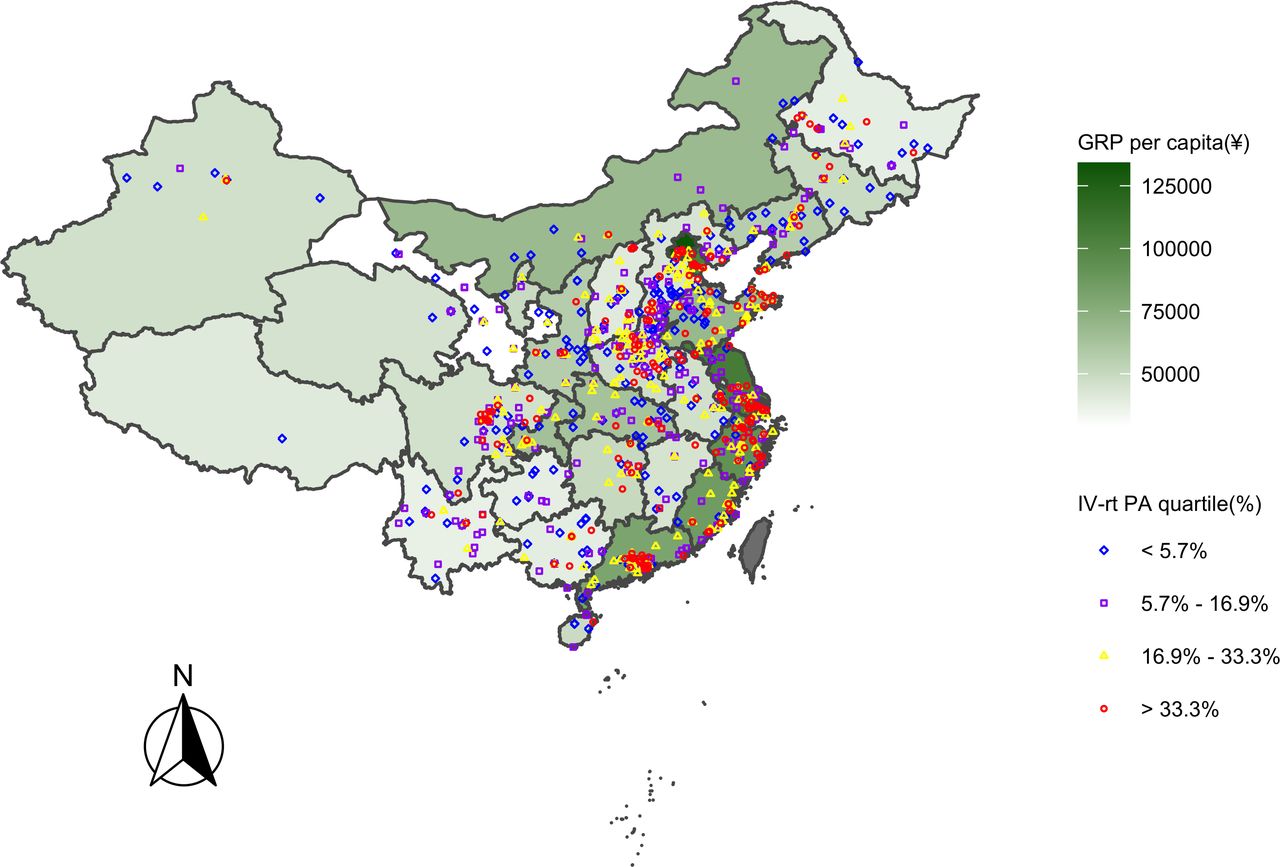{kind=link}
Hospital locations of intravenous tissue plasminogen activator (IV-rt PA) adherence rate quartiles and gross regional product (GRP) per capita distribution.
Characteristics of factors within each IV-rt PA quartile
Table 1 illustrated significant differences in macroeconomic status and certain hospital characteristics among the adherence rate quartiles. The IV-rt PA quartile boundaries at the 25th, 50th, 75th percentiles were 5.7%, 16.9%, 33.3%, respectively. Hospitals with high adherence rate appeared primarily in the high-GRP per capita provinces; mean (SD) GRP per capita was ¥71 288 (¥27 074) for hospitals’ performance in the fourth quartile (Q4), compared with ¥52 657 (¥17 565) hospitals in the first quartile (Q1), ¥57 560 (¥22 278) in the second quartile (Q2), and ¥65 013 (¥23 039) in the third quartile (Q3). The average AIS volume of the hospitals located in Q1 was 366, compared with 577 in Q2, 591 in Q3 and 572 in Q4, the differences among which were significant (p<0.001). The proportions of tertiary hospitals in Q3 and Q4 were 65.6% and 65.9%, respectively, which were higher (p<0.001) than the percentages in Q1 (46.8%) and Q2 (59.5%). Compared with the hospitals located in Q1 (11.9%) and Q2 (20.1%), the percentages of stroke-certified hospitals (CSC) in Q3 (28.8%) and Q4 (30.5%) were higher (p<0.001). The proportion of teaching hospitals in Q1 and Q2 was 86.9% and 85.3%, respectively, compared with 88.2% in Q3 and 92.7% in Q4 (p=0.044). The number of hospital beds in neurology department varied among different adherence rate quartiles, with an average of 82 units in Q1, 90 units in Q2, 93 units in Q3 and 87 units in Q4 (p=0.022). The proportion of the presence of stroke units was higher in Q4 (77.0%) than the other three quartiles (65.5% in Q1, 66.4% in Q2 and 69.5% in Q3), with a p value of 0.006. The comparison of these indicators across the quartiles suggested that the hospitals with higher adherence rate had better training, skills and expertise quality.
Baseline hospital characteristics of 980 hospitals overall and by intravenous tissue plasminogen activator (IV-rt PA) quartile
For characteristics reflecting hospital facility and staffing resources, significant differences were also identified for certain factors. The proportion of hospitals equipped with an ED varied significantly (97.4% in Q1, 100% in Q2, 98.8% in Q3 and 100% in Q4, p=0.026). Significant difference in the availability of neurologists across the quartiles was also observed with an average number of 12 neurologists in Q1, 16 in Q2, 17 in Q3 and 14 in Q4, respectively (p<0.001). Hospitals with higher adherence rate of IV-rt PA had a higher likelihood of being equipped with an acute stroke team (84.9% in Q1, 91.8% in Q2, 94.7% in Q3 and 93.2% in Q4, p<0.001) and providing ED services of thrombolysis (97.0% in Q1, 98.5% in Q2, 98.8% in Q3 and 99.1% in Q4, p=0.041). As the adherence rate increased, the number of neuroimaging services also increased, including CT (average number of CT in Q1, Q2, Q3, Q4 was 1.91, 2.15, 2.20, 2.36, respectively, p<0.001) and MRI (average number of MRI in Q1, Q2, Q3, Q4 was 1.33, 1.41, 1.47, 1.57, respectively, p=0.002).
The percentage of hospitals using stroke-specific protocols also varied significantly among the quartiles (87.3% in Q1, 91.0% in Q2, 90.3% in Q3, 93.7% in Q4, p=0.039), which reflected unequal implementation of organisation guidelines and regulations of hospitals in different areas.
Multivariable analysis of adherence rate to IV-rt PA and factors
The results of multivariable regression are reported in table 2. We considered the adherence rate among different years (2015 as the reference year) respectively and included the time effect in the model as a confounding variable. Six factors, including provincial GRP per capita, the presence of stroke certification, the number of neurologists, existence of emergency services for thrombolytic treatment, presence of an ED and cooperation with emergency centres, remained significantly associated with the adherence rate to IV-rt PA.
Multivariable regression analysis between intravenous tissue plasminogen activator (IV-rt PA) and influential factors
Supplemental material
Among 980 CSCA hospitals located in the 31 provinces, the adherence rate increased by 2.37% (p<0.001) for every ¥10 000 increase in GRP per capita, after controlling for the other factors. Among all the significant factors, the effect of GRP per capita was the largest (absolute value of the standardised βGRP =0.23). The adherence rate to IV-rt PA in the hospitals accredited as CSCs was 3.77% (p<0.001) higher than those PSCs. Compared with the hospitals without emergency services for thrombolysis treatment, the adherence rate was 7.43% higher in those that provide the urgent care (p=0.014). The presence of an ED corresponded to a 10.03% higher adherence rate (p=0.019), while cooperation with emergency centre associated with a 4.65% increase of adherence rate (p=0.029).
The year effect was included as a confounding factor in our model. Compared to 2015, the adherence rate in 2018 and 2019 increased by 4.44% (p=0.002) and 7.79% (p<0.001), respectively, while the adherence rate in 2016 was slightly lower (β=-3.71; p=0.010).
Discussion
For this national study, our analysis observed significant disparity of the adherence rate among 980 hospitals in 31 provinces in China, and identified that GRP per capita had the most significant (positive) effect on the adherence rate, even after controlling for the time effect and hospital characteristics. This empirical evidence strongly suggests that macroeconomic status may contribute to a hospital’s adherence to IV-rt PA.
There are several reasons why macroeconomic status may play a role. First, regional government health expenditure is directly affected by local economic development.24 Previous studies illustrated that the delay of IV-rt PA treatment might be due to high cost of tPA.19 Therefore, for those hospitals in the economically developed areas, they may have more affluent financial support and reimbursement from the local governments than those in the economically underdeveloped areas. Second, there might exist correlation between economic development and healthcare resource allocation. For those hospitals in the higher GRP per capita regions, they had more access to better medical resources and personnel (more neurologists, CT and MRI as well as more hospitals equipped with stroke teams and providing ED services of thrombolysis (table 1)) and therefore were more likely to perform better. Third, there might exist association between stroke centre certification and macroeconomic status. According to the multivariable regression analysis, we found that CSC performed significantly better than PSC. Interestingly, in our data, compared with the hospitals in the first two quartiles of the adherence rate, the hospitals in the third and fourth quartiles were in regions with higher GRP per capita and more of them had CSC certification (table 1). Therefore, this underlying association might also contribute to higher adherence rate among hospitals in higher GRP per capita regions; further research should be conducted following this direction.
Besides the impact of macroeconomic status on the adherence rate, significant effects of certain hospital characteristics were also identified in this study. A number of studies have described positive associations between stroke tPA rates and staffing allocation.14 15 25–27 Our study added more evidence that the adherence rate of IV-rt PA increased as the number of neurologists in a hospital increased.
Conflicting results were documented for the impact of emergency medical service and ED on the thrombolysis rate. While a study in the Netherlands found that hospitals providing ED services did not help to improve the thrombolysis rate,17 another study conducted in 34 academic medical centres in the USA found that integrated emergency medical services and organised EDs predicted increased tPA use.14 Our study confirmed that hospitals equipped with an ED and/or providing emergency services for thrombolytic treatment performed better in the delivery of IV-rt PA.
Previous studies discussed that one of the reasons for the low rate of tPA might be due to factors such as prehospital delay and lack of regional stroke care network.7 We found out that the adherence rate was higher if a hospital established routine cooperation with the local emergency centres, which supported the previous finding.
It is worth noting that the adherence rate in hospitals within the first quartile was quite low (<5.7%), even though most of these hospitals were equipped with stroke units (65.5%) and stroke team (84.9%) as well as implemented the stroke-specific protocols (87.3%) (table 1). Potential reasons might include prehospital delay, high cost of tPA, low insurance coverage and concern about haemorrhagic risk as an earlier anecdotal study concluded.7 Empirical data in the CNSR study showed that patients with a higher income (¥ 1000/month) were nearly twice likely to receive IV-rt PA, since patients and their families of low SES would have to find money to purchase drug before tPA could be given.19 The current condition may have improved because the healthcare insurance has covered IV-rt PA treatment since 2008.28 However, variations in costs still differed widely by geographical location and level of hospitals, and the expensive cost of IV-rt PA might be a barrier of a fluent decision-making process.28 29 We examined the SES of patients using monthly family income and education level as proxies in our study. In our data, in hospitals whose adherence rate was in Q1, the number of patients with a lower income (≤ ¥1000/month) was twice as many as in the other three quartiles (Q1: 12.9%; Q2: 6.4%; Q3: 6.7%; Q4: 6.0%) (online supplement table 2). In addition, patients in Q1 had a higher proportion (Q1: 32.4%, Q2: 25.5%, Q3: 28.1%, Q4: 31.1%) of low education level (below elementary) and a lower percentage of higher education level including college (Q1: 2.5%, Q2: 3.1%, Q3: 3.4%, Q4: 3.7%) and high school (Q1: 28.6%, Q2: 28.8%, Q3: 30.5%, Q4: 32.9%) than those in the other three quartiles. According to CNSR data, around 53.6% of the stroke-care-related payments in China were covered by the urban employee basic medical insurance (UEBMI).30 In our study, we found that the UEBMI scheme was relatively low among patients in Q1 (24.1%), compared with the other three quartiles (Q2:29.7%, Q3:32.0%, Q4:35.1%, respectively). Therefore, low SES and insufficient insurance coverage might account for the low adherence rate in the first quartile.
There are also several limitations in our study. First, the participating hospitals in CSCA were based on voluntary enrolment. These study sites were mainly secondary and tertiary hospitals and therefore had more medical resources and neurologists than primary hospitals. Second, since we lacked the data from non-CSCA hospitals, we were unable to determine whether the findings could be generalised beyond the CSCA hospitals. Despite this limitation, the CSCA remains the only large-scale national surveillance system covering all provinces of China and the large sample size helps the robustness and generalisability of the study. Third, other external factors that were not considered in this study might also have some unobservable effects on the adherence rate to IV-rt PA.
Conclusions
The adherence rate of IV-rt PA increased with GRP per capita. Hospitals equipped with more experienced neurologists, more comprehensive emergency services, routine coordination with local emergency centres performed better in adhering to the delivery of IV-rt PA. Our findings provide some evidence that the thrombolysis disparity can be partially explained at the macroeconomic and healthcare system level, not merely attributable to individual factors. The policy-makers should carefully consider medical funding level and medical resource allocation to increase the IV rt-PA usage among eligible acute ischemic stroke patients.
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank all participating centres in the Chinese Stroke Center Alliance program for their hard work in data collection.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SZ and TJL contributed equally, did the data analysis and drafted the manuscript. ZL, HL and HS served as scientific advisors and oversaw all scientific aspects of its implementation. ZL, HS and HG critically reviewed and revised the whole manuscript. CW, XY and JY collected and managed the data. YW has full access to and take full responsibility for the data, the analyses and interpretation, and the conduct of the research.
Funding This work is supported by Ministry of Science and Technology Major Project of China (2017YFC1310901 and 2017YFC1310903), University of Hong Kong (HKU) Stanley Ho Alumni Challenge Fund (207032065.087736.07030.430.01), HKU University Research Committee Seed Funding Award (104004215), and HKU BRC Fund (007300017.000000.07030.100.01).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.