Article Text

Abstract
Background and purpose Individuals with intracranial artery occlusion have high rates of ischaemic events and recurrence. It has been challenging to identify patients who had high-risk stroke using a simple, valid and non-invasive screening approach. This study aimed to investigate whether fluid-attenuated inversion recovery (FLAIR) vascular hyperintensity (FVH), a specific imaging sign on the FLAIR sequence, could be a predictor of ischaemic events in a population with internal carotid artery (ICA) or middle cerebral artery (MCA) occlusion.
Methods We retrospectively analysed 147 patients (mean 60.43±12.83 years) with 149 lesions, including 37 asymptomatic and 112 symptomatic cases of ICA or MCA occlusion. Symptomatic occlusion was considered if ischaemic events were present in the relevant territory within 90 days. FVH Alberta Stroke Program Early Computed Tomography Score (FVH-ASPECTS: 0–7, with 0 indicating absence of FVH and 7 suggesting prominent FVH) and collateral circulation grade were assessed for each participant. Multivariable logistic regression analysis was performed to detect independent markers associated with symptomatic status.
Results A lower FVH-ASPECTS was associated with a more favourable collateral circulation grade (rho=−0.464, p<0.0001). The FVH-ASPECTS was significantly lower in the asymptomatic occlusion group than in the symptomatic occlusion group (p<0.0001). FVH-ASPECTS (Odd ratio, 2.973; 95% confidence interval, 1.849 to 4.781; p<0.0001) was independently associated with symptomatic status after adjustment for age, sex, lesion location and collateral circulation grade in the multivariate logistic regression. The area under the curve was 0.861 for the use of FVH-ASPECTS to identify symptomatic occlusion.
Conclusions The ability to discriminate symptomatic from asymptomatic occlusion suggests that FVH may be a predictor of stroke. As a simple imaging sign, FVH may serve as a surrogate for haemodynamic impairments and can be used to identify high-risk stroke cases early in ICA or MCA occlusion.
- Cerebrovascular Disorders
- Ischemic Attack, Transient
- Magnetic Resonance Imaging
- MR perfusion
- Stroke
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Individuals with intracranial artery occlusion have high rates of ischaemic events and recurrence.
It has been challenging to identify patients who had high-risk stroke using a simple, valid and non-invasive screening approach for these individuals.
Fluid-attenuated inversion recovery (FLAIR) is a clinically accessible imaging sequence for MRI. FLAIR vascular hyperintensity (FVH), a specific imaging sign on FLAIR, is implicated in cerebral collateral circulation and clinical outcomes in acute ischaemic stroke.
However, the application of FVH in the primary or secondary prevention of intracranial artery occlusion has not been fully elucidated yet.
WHAT THIS STUDY ADDS
This study found that FVH was prevalent in patients with intracranial artery occlusion. The FVH-Alberta Stroke Program Early Computed Tomography Score (FVH-ASPECTS) was independently associated with the symptomatic status of the lesion in the internal carotid artery or middle cerebral artery occlusion.
The ability of the FVH-ASPECTS to identify symptomatic cases yielded an area under the curve of 0.861. FVH-ASPECTS ≥2 had a sensitivity and specificity of 74.11% and 83.78%, respectively.
The ability to discriminate symptomatic occlusion from asymptomatic occlusion using FVH-ASPECTS suggests that FVH may be a competing predictor of stroke.
Our study also demonstrated a moderate negative linear correlation between FVH-ASPECTS and collateral circulation, which further confirmed the haemodynamic mechanism of FVH in symptomatic or asymptomatic intracranial artery occlusion.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
FVH can be easily understood by both neurologists and radiologists.
It may rapidly and non-invasively reflect perfusion deficits, while MR perfusion imaging requires contrast agent administration or is restricted to advanced MRI platforms that are less accessible.
As a simple imaging sign, FVH may serve as a surrogate for the early identification of high-risk stroke cases in intracranial artery occlusion, especially for people in need of clinical-evolutionary assessment.
Introduction
Individuals with major intracranial artery occlusion (internal carotid artery (ICA) or middle cerebral artery (MCA)) have high rates of occurrence and recurrence of ischaemic events.1–4 Early intervention reduces subsequent stroke by 40%.5 6 However, it has been clinically challenging to identify patients who are at a high risk for stroke using a simple, valid and non-invasive screening approach for primary or secondary prevention of ischaemic events in these individuals. Previous studies have demonstrated the critical role of cerebral haemodynamics in ischaemic symptoms in atherosclerotic occlusive disease using transcranial Doppler, positron emission tomography and MR perfusion imaging.7–10 These techniques require the administration of acetazolamide or contrast agents to capture cerebrovascular reserve or haemodynamic changes. Recently, a growing number of studies have used arterial spin labelling (ASL) perfusion imaging to assess the haemodynamic status and predict ischaemic events in patients with cerebral artery steno-occlusion.11–14 However, ASL is predominantly available in advanced MR systems. Therefore, an easily accessible technique is required.
Fluid-attenuated inversion recovery (FLAIR) vascular hyperintensity (FVH), an imaging sign of the absence of arterial flow voids on T2-FLAIR, is believed to be a feasible imaging marker for identifying patients with cerebral artery steno-occlusion.15 16 More importantly, studies have shown that the prominence and location of FVH may correlate with collateral circulation as well as the severity of haemodynamic impairments, and further impact clinical outcomes in acute ischaemic stroke.17–20 In patients with transient ischaemic attack (TIA), the presence of FVH has been proven to be a marker of stroke.21 These studies highlight the predictive value of FVH in the acute stage of cerebral ischaemia. However, the application of FVH in the primary or secondary prevention of ischaemic events has not been fully elucidated.
This study aimed to investigate whether FVH could be a predictor of ischaemic events in a population with ICA or MCA occlusions.
Methods
Participants
Symptomatic and asymptomatic patients aged >18 years with intracranial and/or extracranial ICA or MCA occlusions between August 2015 and December 2019 were retrospectively analysed. All patients underwent routine head MRI including T2-FLAIR and ASL. We excluded patients with clinically and radiologically suspected Moyamoya disease and those with a >90 day period from symptom onset to imaging.
Symptomatic occlusion was considered if ischaemic events, including stroke or TIA within 90 days, were present in the related territory. Asymptomatic occlusion was identified incidentally during clinical care or health examination, and was defined as the absence of history of ischaemic events occurring in the target downstream territory.22 In symptomatic occlusion, recent ischaemic events were categorised as acute ischaemic stroke with symptom onset to MRI time within 24 hours, subacute to chronic ischaemic stroke, and TIA.
MRI protocol
All MR studies were performed using a 3.0 T scanner (Discovery 750; GE Healthcare, Milwaukee, Wisconsin, USA) with a 32-channel head coil. The T2-FLAIR MR protocol comprised a repetition time (TR) of 6000 ms, echo time (TE) of 160 ms, inversion time of 2250 ms, field of view (FOV) of 24 cm, matrix of 256×256, slice thickness of 5 mm, intersection gap of 1 mm and number of slices of 20. The three-dimensional pseudo-continuous ASL protocol comprised a TR=4590 ms (post labelling delay (PLD)=1.5 s), 5025 ms (PLD=2.0 s), labelling duration=1500 ms, TE=10.5 ms, FOV=24 cm, spatial resolution=3.64 mm, slice thickness=4.0 mm, number of slices=36, number of excitations=2 and background suppressed.
Image analysis
The presence of ICA or MCA occlusion was confirmed using MR. FVH was defined as a linear or serpentine hyperintense appearance distal to the occlusive lesion on axial T2-FLAIR images. The FVH-Alberta Stroke Program Early Computed Tomography Score (ASPECTS), a semiquantitative scoring system for the evaluation of FVH prominence in accordance with insular and M1–M6 regions in the ASPECTS, was applied and assessed for each participant (online supplemental figure S1).23 FVH-ASPECTS of 0 indicated the absence of FVH, whereas FVH-ASPECTS of 7 suggested prominent FVH.
Supplemental material
In the collateral circulation evaluation, the hypoperfusion region and arterial transit artifact (ATA) on ASL was identified for each participant. According to previous studies,24 25 hypoperfusion was used to determine the ischaemic region, and ATA was used to depict the presence and robustness of the collaterals. An ASL-collateral grading system was adopted based on the presence of ATA and hypoperfusion abnormalities as follows: G0, no ATA in the downstream hypoperfusion abnormality; G1, no or minimal ATA distribution of less than 1/2 downstream hypoperfusion abnormality; G2, moderate ATA distribution of more than 1/2 downstream hypoperfusion abnormality and G3, normal perfusion without downstream ATA. The representative cases are shown in figure 1.

Representative cases with unilateral ICA (A) or MCA (B–D) occlusion presenting different ASL-collateral grades. (A) G0, indicating no ATA in the downstream hypoperfusion abnormality. (B) G1 suggesting minimal ATA (arrow) distribution of less than 1/2 downstream hypoperfusion region. (C) G2, suggesting moderate ATA distribution of more than 1/2 downstream hypoperfusion region. (D) G3, suggesting normal perfusion without downstream ATA. Arrows indicate ATA. ASL, arterial spin labelling; ATA, arterial transit artifact; ICA, internal carotid artery; MCA, middle cerebral artery.
Two experienced neuroradiologists (one with 5 years of experience and another one with 11 years of experience), who were blinded to other clinical or imaging information, independently assessed FVH-ASPECTS and ASL-collateral grade, respectively. The differences in opinions between them were resolved by consensus reading.
Statistical analysis
All quantitative data were expressed as mean±SD and qualitative data was expressed as the percentile. To assess inter-rater agreement for FVH-ASPECTS and ASL-collateral grade, Cohen’s kappa was applied, and weighted kappa was calculated in 30 randomly selected cases. Correlation analysis of variables was also performed to explore the relationship between FVH-ASPECTS, ASL-collateral grade and other factors using Spearman’s rank correlation. Clinical and imaging characteristics of symptomatic and asymptomatic occlusions were compared. All variables with p<0.1 were included in the multivariable analysis. Multivariable logistic regression analysis was performed to identify independent factors associated with symptomatic occlusion. The variance inflation factor was calculated to detect collinearity in the multivariate model. A variance inflation factor of >10 was considered an indicator of significant collinearity. Receiver operating characteristic analyses were performed to evaluate FVH-ASPECTS in identifying symptomatic occlusive lesions.
All statistical analyses were performed using SPSS (V.20.0; IBM Corporation, Armonk, New York, USA) and R studio(V.4.0.5; Boston, Massachusetts). Statistical significance was set at p <0.05.
Results
Patient demographics and variables’ correlation analysis
A total of 147 patients (mean 60.43±12.83 years, 35 women) with 149 lesions, including 37 asymptomatic and 112 symptomatic ICA or MCA occlusions. One patient had bilateral MCA occlusion, with symptomatic occlusion in the left MCA and asymptomatic occlusion in the right MCA. Another patient had bilateral asymptomatic ICA occlusion. No ischaemic lesions were detected in the territories corresponding to the asymptomatic occlusions. There were 78 MCA and 71 ICA occlusions. In the symptomatic occlusion group, 47 cases had acute ischaemic strokes with event-to-MR imaging time within 24 hours, 42 had subacute to chronic ischaemic stroke and 23 had lesions with TIA as an index event. The mean time from symptom onset to MRI was 13.34±18.83 days for the symptomatic lesions.
The overall rate of FVH presence was 77.2 %, and the rate of ATA presence was 81.2%. The median FVH-ASPECTS was 2 (IQR, 1–3) and the median ASL-collateral grade was 2 (IQR, 1–3) in the study sample.
FVH-ASPECTS was significantly associated with ASL-collateral grade. A lower FVH-ASPECTS was associated with a more favourable collateral grade (r=–0.464, p<0.0001). FVH-ASPECTS was negatively associated with the event-to-imaging time in the symptomatic occlusion group. The correlations between FVH-ASPECTS, ASL-collateral grade and age are shown in figure 2A. The correlations between FVH-ASPECTS, ASL-collateral grade and event-to-imaging time in the symptomatic occlusion group are shown in figure 2B. None of the tested variables reached significant collinearity, as assessed by the variance inflation factor.

Correlation analysis of variables. (A) Correlations between FVH-ASPECTS, ASL-collateral grade and age in all patients. (B) Correlations between FVH-ASPECTS, ASL-collateral grade and event-to-imaging time in the symptomatic occlusion group. ASL, arterial spin labelling; ASPECTS, Alberta Stroke Program Early Computed Tomography Score; FVH, fluid-attenuated inversion recovery vascular hyperintensity.
Overall, the inter-rater agreement was good for the assessment of the FVH-ASPECTS (weighted kappa=0.729) and ASL-collateral grade (weighted kappa=0.690).
Factors associated with symptomatic occlusion
Patients with symptomatic occlusion were older and predominantly women as compared with patients with asymptomatic occlusion (p<0.05). The FVH-ASPECTS was significantly lower in the group with asymptomatic occlusion, whereas the ASL-collateral grade was significantly higher (p<0.0001). There were no significant differences between the groups in the occlusive site and risk factors, including hypertension, diabetes, lipid disorders, coronary artery disease and smoking. The details are presented in table 1.
Comparison of clinical and imaging characteristics between symptomatic and asymptomatic occlusions
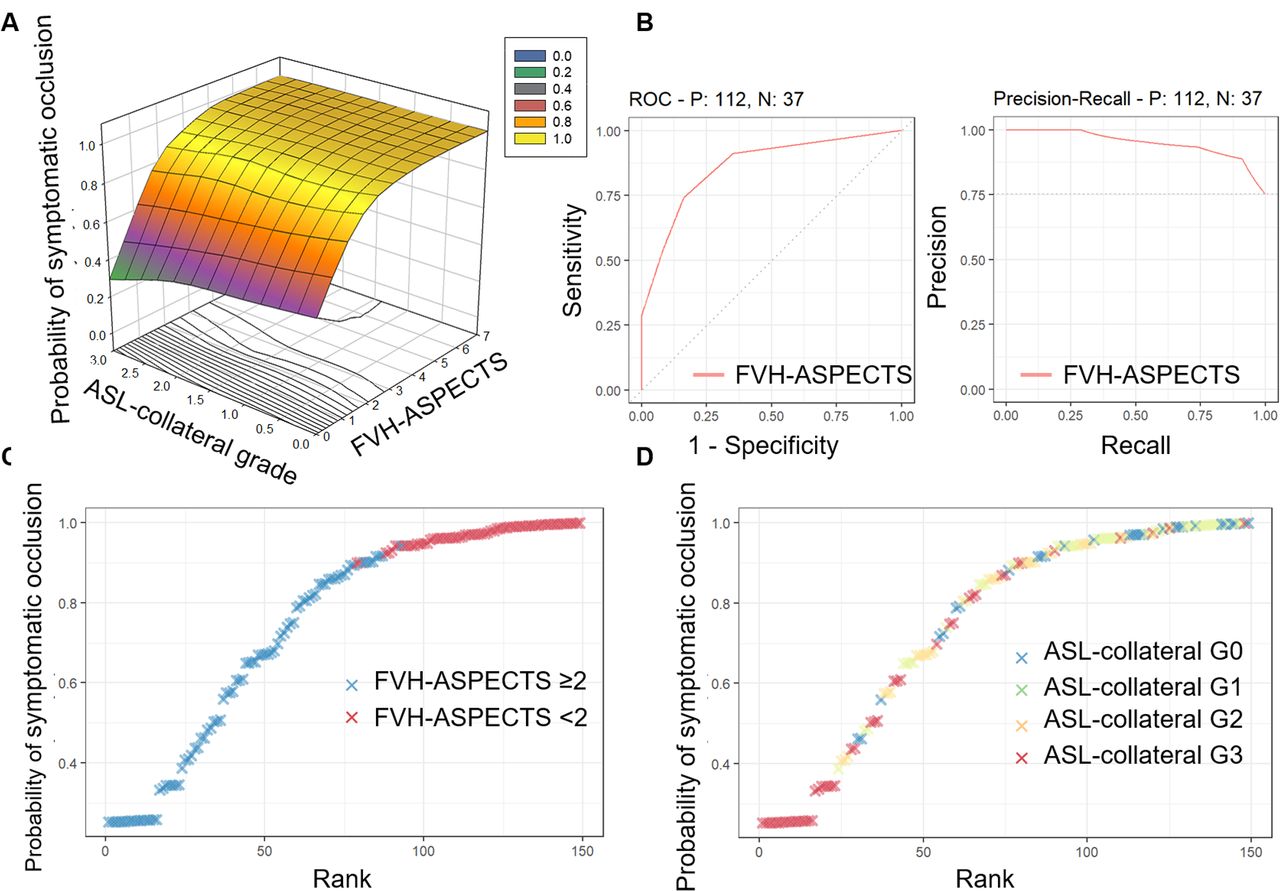
According to the discrimination model using multivariable logistic regression, there was a significant independent association between FVH-ASPECTS (Odd ratio (OR), 2.973; 95% confidence interval (CI), 1.849 to 4.781; p<0.0001) and the symptomatic status after adjustment for age, sex, occlusive site and ASL-collateral circulation grade (a summary of statistical results for different logistic regression models was provided in online supplemental table S1). The odds of being symptomatic increased by 197% for the FVH-ASPECTS, increasing the score by 1. Table 2 presents the factors associated with symptomatic status of intracranial ICA or MCA occlusion. Based on the discrimination model, the likelihood of developing symptomatic occlusion according to FVH-ASPECTS and ASL-collateral grade is presented in figure 3A.

Association between FVH-ASPECTS, ASL-collateral grade and probability of symptomatic occlusion of the internal carotid artery or middle cerebral artery. (A) Three-dimensional scatterplots with fitted surfaces illustrate the association between FVH-ASPECTS, ASL-collateral grade and the probability of symptomatic occlusion in the multivariate logistic regression. (B) Receiver operating characteristic curve and precision-recall curve of FVH-ASPECTS in identifying symptomatic occlusion of the internal carotid artery or middle cerebral artery. Distribution of FVH-ASPECTS dichotomised by ≥2 (C) and each ASL-collateral grade (D) along with the increasing probability of symptomatic status is presented. ASL, arterial spin labelling; ASPECTS, Alberta Stroke Program Early Computed Tomography Score; FVH, fluid-attenuated inversion recovery vascular hyperintensity; N, negative; P, positive; ROC, receiver operating characteristic.
Factors associated with symptomatic status in intracranial ICA or MCA occlusion
The area under the curve (AUC) was 0.861 (95% CI 0.795 to 0.912) to identify symptomatic occlusion by FVH-ASPECTS (figure 3B). The optimal threshold was FVH-ASPECTS ≥2, with sensitivity, specificity, positive predictive value and negative predictive value of 74.11%, 83.78%, 93.3% and 51.7%, respectively. We also tested the clinical practical threshold of FVH-ASPECTS ≥1 (FVH-positive vs FVH-negative), which revealed sensitivity, specificity, positive predictive value and negative predictive value of 91.07%, 64.86%, 88.7% and 70.6%, respectively (FVH-ASPECTS threshold effects on the sensitivity and specificity for identifying symptomatic status are plotted in online supplemental figure S2). Patients with FVH-ASPECTS ≥2 had a higher probability of developing symptomatic occlusion, while ASL-collateral grades showed no distinctive distribution in symptomatic status probability (figure 3C and D).
Subgroup analysis
The proportion of symptomatic occlusion as well as the subgroups of acute ischaemic stroke, subacute to chronic ischaemic stroke and TIA were compared between the different groups in figure 4A. Figure 4B shows representative cases of FVH in acute ischaemic stroke, subacute to chronic ischaemic stroke, TIA and asymptomatic occlusion. The proportion of patients with FVH-ASPECTS ≥2 was significantly higher in the group with symptomatic occlusion than in the group with asymptomatic occlusion (p<0.0001). The proportion of patients with FVH-positive was significantly higher in the group with symptomatic occlusion than in the group with asymptomatic occlusion (p<0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Symptomatic status comparison between subgroups. (A) Comparison of the proportions of the index events between subgroups of FVH, ATA, ASL-collateral grade, occlusive site and sex. P value indicates results for χ2 test of the proportion of TIA, acute stroke, non-acute stroke and asymptomatic occlusion between groups. (B) Representative cases illustrate the extent of FVH in ipsilateral middle cerebral artery occlusions with acute stroke, non-acute stroke, TIA and asymptomatic status. Arrows indicate FVH. ASL, arterial spin labelling; ASPECTS, Alberta Stroke Program Early Computed Tomography Score; ATA, arterial transit artifact; DWI, diffusion-weighted imaging; FLAIR, fluid-attenuated inversion recovery; FVH, fluid-attenuated inversion recovery vascular hyperintensity; ICA, internal carotid artery; MCA, middle cerebral artery; MRA, MR angiography; TIA, transit ischaemic attack.
Discussion
Our study found that in ICA or MCA occlusion, FVH-ASPECTS was independently associated with the symptomatic status of the lesion. The ability of FVH-ASPECTS to identify symptomatic cases yielded an AUC of 0.861. FVH-ASPECTS ≥2 had a sensitivity and specificity of 74.11% and 83.78%, respectively. The remarkable ability to discriminate symptomatic occlusion from asymptomatic occlusion suggests that FVH may be a reliable predictor of stroke. Our study also demonstrated a moderate negative linear correlation between FVH-ASPECTS and collateral circulation grade assessed using ASL, which further confirmed the haemodynamic mechanism of FVH.
FVH identified on T2-FLAIR has shown extensive utility in cerebrovascular diseases. Studies have investigated FVH and its determinants in acute and chronic ischaemic stroke. Some studies have demonstrated that the FVH prominence negatively correlates with the robustness of collateral circulation,26 27 which corroborates with the finding in our study. However, some studies have reported on the contrary that prominent FVH is associated with better collaterals.17 28 29 Tian and Lou also indicated that FVH might reflect intermediate collaterals because excellent collateral and no collateral both result in the absence of slow flow within the vessels.30 The heterogeneous results suggest that FVH may partly indicative for collateral circulation but may fully associate with haemodynamic changes.
Studies reporting association between FVH and haemodynamic impairments evaluated using perfusion imaging parameters have shown consistent results.31 A positive correlation between the severity of the delayed time to the maximum residue function (Tmax) has been reported earlier.26 Therefore, some studies have applied FVH-ASPECTS and DWI to identify the presence of a target mismatch profile as defined by the difference region between Tmax >6 s and ischaemic core in acute anterior circulation large-vessel occlusive stroke.32 33 In a prospective cohort study, Nam et al investigated the efficiency of DWI-based and FVH-based imaging paradigms in predicting stroke risk after TIA,21 and reported that FVH was significantly associated with subsequent stroke. It has been reported that FVH might resolve during follow-up.34 Our study also found a negative correlation between FVH and longer event-to-imaging times. As indicated, all underlying mechanisms may be attributed to hypoperfusion lesions and their recovery.34 Therefore, FVH may be used as a simple indicator of perfusion deficits. Further, it provides important information for subsequent outcome prediction.35 36
The findings of our study show that FVH-ASPECTS is a feasible imaging marker to understand cerebral haemodynamics. FLAIR is routinely acquired in stroke imaging while dynamic susceptibility contrast perfusion imaging requires contrast agent administration, and ASL is restricted to advanced MRI platforms, which are less accessible. Further, FVH-ASPECTS is easily understandable by both neurologists and radiologists, and may rapidly and non-invasively provide information of perfusion deficit. In patients with multiple vascular lesions who present with non-specific symptoms, FVH-ASPECTS may be indicative of the causative lesion. Hypothetically, adding FVH-ASPECTS to clinical prediction models, such as the ABCD2 scoring system,37 may improve their predictive performance. In addition, FVH and ATA, which share similar mechanisms such as slow blood flow, both have gained growing research interest and attention in stroke imaging. Based on data of 147 patients for whom ASL was acquired, this study reported their relationship that could aid better identification of their roles in clinical assessment.
Limitations
This study had some limitations. First, ATA-based grading scale has been a validated approach to assess collateral circulation24 25 38; however, ATA may be influenced by PLD. In our study, PLD was not identical in all the patients. Ninety-six patients had a PLD of 2 s in accordance with the previous study or recommendation.24 39 Fifty-one patients had a PLD of 1.5 s, which might have increased the incidence of ATA due to more labelled blood remaining in the arteries with a shorter PLD. Second, this study was a retrospective analysis with a relatively small sample size. Further prospective cohort studies analysing the occurrence of stroke in these patients during long-term follow-up are warranted to investigate the direct relationship between FVH and the risk of ischaemic events. Validation of the ability of FVH to predict symptoms in ischaemic cerebrovascular disease is also warranted.
Conclusions
FVH is prevalent in populations with ICA or MCA occlusion. FVH-ASPECTS is correlated with cerebral haemodynamics and changes over time. We found that FVH was strongly associated with symptomatic ICA or MCA occlusion and had excellent diagnostic accuracy. As a simple imaging sign, FVH may serve as a surrogate for haemodynamic impairments, and can be used for early identification of high-risk stroke cases in ICA or MCA occlusion, especially for people in need of clinical-evolutionary assessment.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The institutional review board approved the study (reference number: S2018-193-01). Written informed consent was obtained from all subjects in this study.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JL and JH are joint first authors.
Contributors XL, JL and CT conceived and designed the study. JL, JH, XB, MW, LW, YL, DZ, QD, TZ and XW acquired and analysed the data. JL, JH, XW and XL drafted the manuscript. Guarantor of the study: XL.
Funding This study was funded by National Natural Science Foundation of China (81901708, 81730048, 81825012, 82151309).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.