Article Text

Abstract
Background and purpose We investigated the baseline demographics of patients with severe unilateral atherosclerotic stenosis of the middle cerebral artery (MCA) using multimodal MRI and evaluated the haemodynamic impairments and plaque characteristics of patients who had a recurrent stroke.
Materials and methods We retrospectively recruited consecutive patients with severe unilateral atherosclerotic MCA stenosis who underwent arterial spin labelling (ASL) with postlabelling delay (PLD) of 1.5 and 2.5 s, and vessel wall MRI. For each PLD, cerebral blood flow (CBF) maps were generated. Hypoperfusion volume ratio (HVR) from 2 PLD CBF was calculated. An HVR value ≥50% was considered as severe HVR. Plaque areas, plaque burden, plaque length and remodelling index were measured. Plaque enhancement at maximal lumen narrowing site were graded. Baseline clinical and imaging characteristics were compared between patients with (event+) and without (event−) 1 year ischaemic events.
Results Forty-three patients (47.23±12.15 years; 28 men) were enrolled in this study. Seven patients had an HVR ≥50%. During the 1-year follow-up, 7 patients had experienced a recurrent stroke. HVR were significantly higher in the event+ than event− (53.17%±29.82% vs 16.9%±15.57%, p=0.0002), whereas no significant difference was detected in plaque areas, plaque burden, remodelling index, plaque length and plaque enhancement grade. The multivariable analysis revealed that a severe HVR was significantly associated with a recurrent stroke (Odds ratio=12.93, 95% confidence interval 1.57 to 106.24, p=0.017) after adjusted by hypertension and smoking.
Conclusion HVR obtained from two PLD ASL may be a useful imaging predictor of recurrent stroke.
- intracranial atherosclerotic disease
- arterial spin labeling
- post labeling delay
- high-resolution mri
- stroke mechanism
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- intracranial atherosclerotic disease
- arterial spin labeling
- post labeling delay
- high-resolution mri
- stroke mechanism
Introduction
Haemodynamic impairments and plaque rupture are considered as the two most important factors causing ischaemic stroke in patients with intracranial atherosclerotic stenosis (ICAS).1 Doppler microemboli monitoring studies have provided great insight into the mechanisms of ICAS stroke.2 Some studies have suggested that hypoperfusion and embolism from active plaque may act alone or interact and complement each other, causing ischaemic stroke in patients with ICAS.3 Thus, more and more attention has been paid to the brain tissue perfusion and to atherosclerotic plaque activity attributed to the development of advanced neuroimaging. Multimodal MRI including perfusion imaging and plaque imaging has been used to assess brain perfusion deficit and the intracranial artery atherosclerotic plaque vulnerability by high-resolution vessel wall imaging (HRVWI). Especially, arterial spin labelling (ASL) perfusion imaging provides unique advances in non-invasive haemodynamics and collateral circulation status assessments in stroke,4 5 with the application of multiple postlabelling delays (PLD).6–8 Contrast-enhanced HRVWI has been shown to allow for plaque activity evaluation particularly in case of intraplaque inflammation.9 10 The applications render these techniques more competitive ways to explore the underlying mechanism or mechanism evolution of ischaemic stroke and stroke recurrence.
Stroke mechanism closely relates to the prognosis and response to medical therapy or endovascular treatment in symptomatic intracranial stenosis. Establishing the role and weightiness of haemodynamic impairments and plaque vulnerability in specific mechanism of individual patient is potentially important.1 3 11
In the present study, we investigated the baseline demographics of patients with severe unilateral atherosclerotic stenosis of the middle cerebral artery (MCA) using multimodal MRI and evaluated the haemodynamic impairments and plaque characteristics of patients who had a recurrent stroke.
Materials and methods
In this retrospective study, we recruited consecutive patients with unilateral atherosclerotic stenosis of the MCA in two different hospital centres from August 2013 to March 2015. Written informed consent in accordance with the Declaration of Helsinki was obtained from each patient or their family member.
Including criteria were as follows: (1) symptomatic unilateral severe MCA stenosis (70%–99%) as confirmed by magnetic resonance angiography (MRA) or conventional angiography with ischaemic stroke, or transit ischaemic attack within 90 days; (2) age >18 years; (3) presence of two or more atherosclerotic risk factors including hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease, obesity and smoking; (4) no contradiction to aggressive medical therapy; (5) not receiving endovascular stenting therapy; (6) having conducted multimodal MRI and (7) completed follow-up.
Excluding criteria were as follows: (1) patients with multiple moderate-to-severe stenoses (>50%) in intracranial arteries and extracranial arteries or with less than two atherosclerotic risk factors; extracranial arterial stenosis was evaluated by routine carotid ultrasound; (2) other vasculopathy such as vasculitis or dissection; (3) evidence of cardioembolism; (4) poor image quality that prevented further analysis.
Imaging protocols
Our multimodal MRI protocol included a routine head protocol, three-dimensional (3D) time-of-flight (TOF) MRA, HRVWI and 3D pseudocontinuous ASL (3D pCASL) with two PLDs: 1.5 and 2.5 s. Three-dimensional pCASL was acquired using 3D spiral fast spin echo (FSE) with the following parameters: repetition time (TR)=4590 (PLD=1.5 s), 5285 ms (PLD=2.5 s), labelling duration=1500 ms, echo time (TE)=10.5 ms, field of view (FOV)=24 cm, 512 sampling points on eight spirals, spatial resolution=3.64 mm, slice thickness=4.0 mm, number of slices=36, number of excitation=2, background suppressed. The HRVWI technique consisted of proton density-weighted imaging (PDWI), T1WI and postcontrast T1WI. A sagittal view, perpendicular to the MCA lesion and covering the site of maximal lumen narrowing (MLN), was acquired. Then, T1WI was obtained by quadruple inversion recovery fast spin echo with TR/inversion time / TE=800/650/8.6 ms, FOV=16×16 cm, thickness=2 mm, matrix=256×320, number of excitations=4, echo-train length=12. Postcontrast T1WI was performed after 5 min of gadolinium injection (0.1 mmol/kg gadopentetate dimeglumine, Magnevist; Bayer Schering Pharma, Berlin, Germany). The total scan time was about 20 min.
Conventional angiography was performed within 5 days of MR scanning and imaging assessments were required to cover the transition from arterial phases to venous phases in order to be adequate for the reviewer grading collateral circulation.
Imaging postprocessing and evaluation
Cerebral blood flow (CBF) map was automatically postprocessed from ASL sequences on an AW workstation 4.3 (GE Healthcare). The CBF maps were then transferred to a personal computer. For each patient, hypoperfusion volume was measured in 1.5 and 2.5 s CBF maps by manual segmenting using a free software: perfusion mismatch analyzer, V.5.0 (http://asist.umin.jp/). Through visual inspection, hypoperfusion was defined as a decrease in CBF compared with the contralateral territory. Haemodynamic impairments were indexed using the hypoperfusion volume ratio (HVR), which was calculated as follows: HVR=(hypoperfusion volume at 2.5 s/hypoperfusion vol at 1.5 s×100%). An HVR value ≥50% was defined as severe haemodynamic impairments (severe HVR). HVR measurements were performed twice by a reader (JL) with a period longer than 1 month, and were also performed by another reader (XL) to test the intra-reader and inter-reader variability.
Collateral grades from conventional angiography were obtained according to the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) grading system.12 13
Regarding HRVWI, the plaque at MLN was identified by eccentric wall thickening and the degree of plaque enhancement was categorised from grade 0 to 2. Grade 0 indicated a similar degree of enhancement to the unaffected intracranial arterial wall. Grade 2 indicated that the plaque enhancement was similar to or greater than the postcontrast pituitary signal intensity. Grade 1 indicated a degree of enhancement between grade 0 and grade 2.9 Intraplaque haemorrhage was identified as a focal intraplaque lesion with a signal intensity ≥150% of the adjacent normal brain parenchyma. Meanwhile, vessel area (VA) and lumen area (LA) were manually traced at MLN site as well as reference site to calculate plaque areas, plaque burden and arterial remodelling index according to previous PDWI studies.14 15 Wall area (WA) was obtained by VA−LA. Plaque area was calculated by (WA at MLN site−reference WA). Remodelling index was the ratio of VA at MLN to reference VA. Plaque burden was calculated as (plaque area/VA at MLN)×100%. Plaque length was obtained by number of slices affected by the plaque×slice thickness.
All imaging evaluations were independently conducted by two experienced neuroradiologists. Disagreements were resolved by consensus reading.
Aggressive medical treatment
Patients received aspirin (100 mg/day) plus clopidogrel (75 mg/day) for 90 days after the quantifying event as well as vascular risk factors modification included keeping systolic blood pressure at <140 mm Hg (or <130 mm Hg in patients with diabetes), low-density lipoprotein at <70 mg/dL or a decrease by 50%, and smoking cessation.
Follow-up
The primary outcome was the presence of ischaemic events, including recurrent TIA or ischaemic stroke in the same territory of the qualifying event, which was confirmed by a neurologist and/or by neuroimaging. The secondary outcome was the value obtained on the modified Rankin Scale (mRS) after 3 months, for which a value >2 was thought to be a poor outcome. Patients were then followed up for 12 months by telephone investigating for signs of cerebrovascular events, risk factors and current medical treatment.
Statistical analysis
Intra-reader and inter-reader variability for the measurements of HVR were determined by intraclass correlation coefficient (ICC). In patients who had conducted conventional angiography, a Spearman’s correlation was performed between conventional angiography collateral grades and hypoperfusion volume and HVR. Baseline characteristics, HVR and plaque parameters were compared between patients with and without ischaemic events using Student’s t-tests or non-parametric tests and X2 tests or Fisher’s exact tests when appropriate. Then, multivariable logistic regressions were used to detect a potential association between baseline clinical and imaging characteristics and follow-up ischaemic events. A p value <0.05 was used to infer statistically significant difference. All statistical analyses were performed using the Statistical Package for Social Sciences (V.20, Chicago, Illinois, USA).
Results
Forty-three patients (47.23±12.15 years; 28 men) were enrolled in this study with 41 M1 segment lesions and two M2 segment lesions. Baseline characteristics of these patients are listed in table 1.
Baseline characteristics of patients with different outcome
HVR measurements and intra-reader and inter-reader variability assessment
Mean hypoperfusion volume at 1.5 s was 51.55±43.14 mL. Mean hypoperfusion volume at 2.5 s was 18.30±33.26 mL. The mean of HVR was 22.8%±22.64% and ranged from 0% to 93.08%. Seven patients presented with an HVR ≥50%. Intra-reader variability was with an ICC of 0.851 (95% confidence interval (CI) 0.741 to 0.916) and inter-reader variability was with an ICC of 0.755 (95% CI 0.443 to 0.904), which indicated a moderate-to-good test–retest reliability for HVR measurements.
Correlation between HVR and collateral circulation grades
Seventeen patients (50.47±7.23 years; 12 men) underwent conventional angiography, including ASITN/SIR grade 3=6 patients, grade 2=8 patients, grade 1=3 patients, grade 0=0 patients. HVR was significantly correlated with collateral grades (r=−0.484, p=0.049), while hypoperfusion volumes at 1.5 and 2.5 s CBF map were not significantly correlated with collateral grades (r=0.394, p=0.118 and r=−0.088, p=0.738).
Group comparison and multivariable analysis
In MLN site, plaque areas, plaque burden, remodelling index and plaque enhancement grade are listed in table 1. No intraplaque haemorrhage was detected in all the patients. During the 1-year follow-up, seven patients were confirmed to have a recurrent event in the same territory. Four patients had a recurrent stroke during the first 3 months, including two patients treated with endovascular stent therapy after the stroke occurrence. Two patients had an mRS score >2 after 3 months. Results showed that hypoperfusion volumes at 2.5 s PLD, and HVR were significantly higher in patients with ischaemic events than in patients with no ischaemic events. The proportion of severe HVR was significantly higher in patients with ischaemic events than in patients with no ischaemic events (57.14% vs 8.33%, p=0.008). In contrast, no significant difference was detected in plaque areas, plaque burden, remodelling index, plaque length and plaque enhancement grade between the two groups. Some representative cases are shown in figures 1-2. Risk factors between groups also showed no significant differences (table 1).

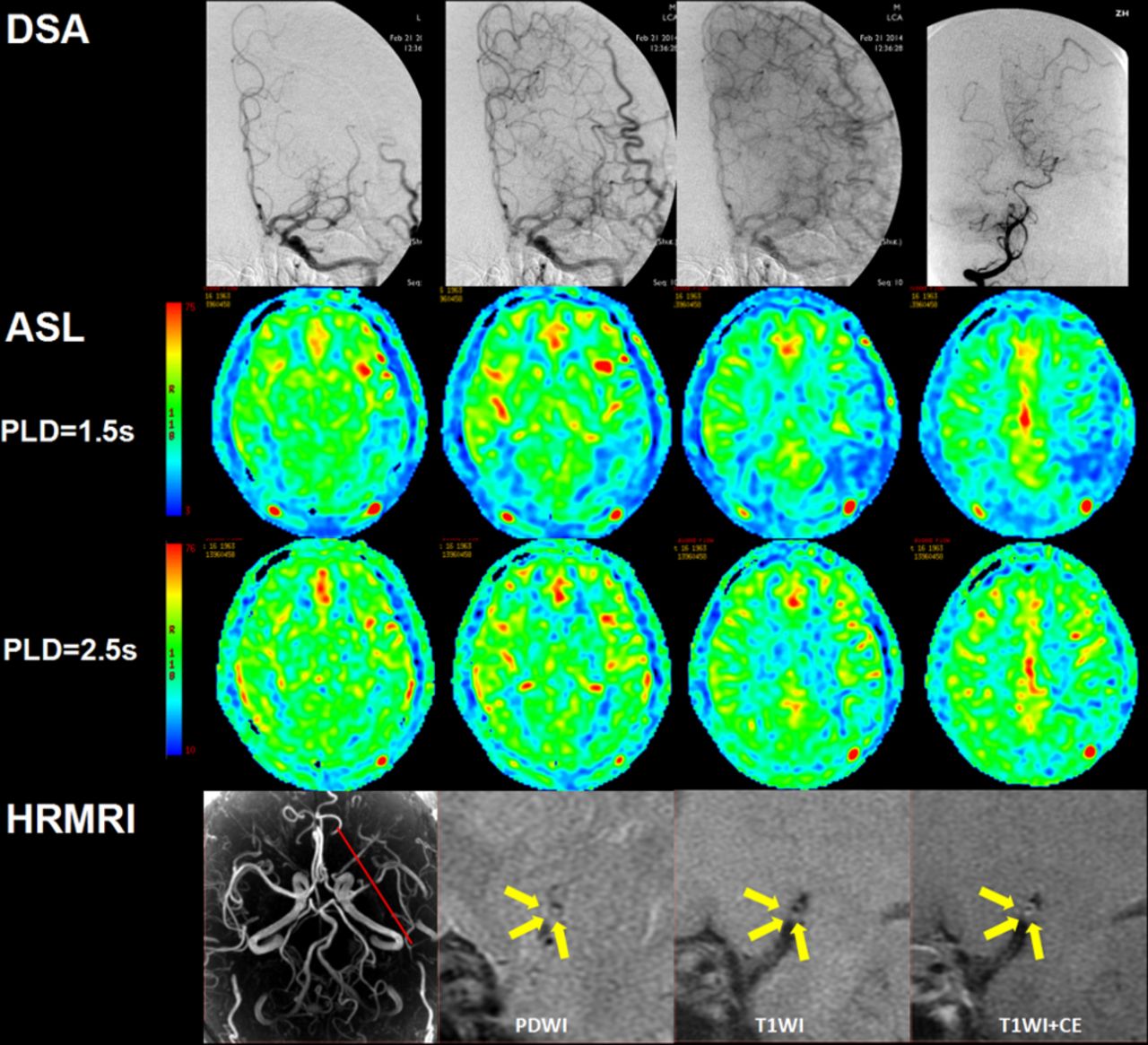
Representative patient with recurrent stroke. A male aged 52 years with left M2 segment severe stenosis shows inadequate collateral within MCA territory on DSA and is assessed as ASITN/SIR grade 1. Slow and only a few inflows can be seen on CBF map from 1.5 to 2.5 s. Hypoperfusion is still observed on 2.5 s CBF map. Hypoperfusion volume ratio is measured as 63%. HRVWI shows that a plaque affects the anterior and inferior arterial wall and has focal moderate contrast enhancement. The patient had experienced a recurrent stroke in the subsequent 6 months. ASL, arterial spin labelling; CBF, cerebral blood flow; HRVWI, high-resolution vessel wall imaging; MCA, middle cerebral artery; PLD, postlabelling delay.
{kind=link}
{kind=link}
Representative patient without recurrent stroke. A male patient aged 51 years with left M1 segment severe stenosis shows slow and complete collateral compensation within MCA territory on DSA and is assessed as ASITN/SIR grade 3. Obvious slow inflow can be seen on CBF map from 1.5 to 2.5 s, and therefore only a very small hypoperfusion volume can be observed on 2.5 s CBF map. Hypoperfusion volume ratio is measured as 10%. HRVWI shows a plaque affects the anterior and inferior arterial wall and has heterogeneous moderate contrast enhancement. ASL, arterial spin labelling; CBF, cerebral blood flow; HRVWI, high-resolution vessel wall imaging; MCA, middle cerebral artery; PLD, postlabelling delay.
The multivariable analysis revealed that a severe HVR was significantly associated with a recurrent stroke (Odds ratio =12.93, 95% CI 1.57 to 106.24, p=0.017) after adjusted by hypertension and smoking.
Discussion
To the best of our knowledge, this is the first study evaluating haemodynamic impairments and plaque features in stroke recurrence for ICAS using multimodal MRI, and the first study using ASL to evaluate the severity of perfusion deficits. The strength of this study is that it demonstrates the feasibility of using two PLD ASL to evaluate collateral circulation and the prognostic value of HVR in patients with severe stenosis of the MCA. We also focus on the relationship between ischaemic events and the culprit plaque characteristics which has not been found to be relevant to future ischaemic events. Although the cohort, with a limited sample size and by the nature of retrospective, represented a selected population, the overall 1 year stroke recurrence (16.3%) was close to a published prospective series with population-based cohort which found a similar 1 year stroke recurrence (17.1%) for intracranial atherosclerosis in Chinese population,16 and were also within the range of stroke recurrent rate reported in Warfarin–Aspirin Symptomatic Intracranial Disease Trial17 and Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis Trial.18
Hypoperfusion may lead to border-zone infarction and disorder of regional microemboli clearance resulting in artery-to-artery embolism infarction located in the cortical region.19 In ICAS, good collateral circulation is able to compensate for the decreased blood flow in the ischaemic tissue due to artery stenosis or occlusion.20 Collaterals characterise dynamic and various complementary patterns in cerebral blood circulation and the capability of collaterals greatly impacts the haemodynamic status.21 In the present study, although associated with prognosis, hypoperfusion volume at 2.5 s CBF was not helpful to interpret collateral circulation and severity of hypoperfusion. We developed a haemodynamic parameter (HVR) and showed its correlation with collateral grades assessed by conventional angiography, which also promoted HVR as an potential imaging marker to evaluate collaterals for this specific disease. Previously, Bang et al 22 and Olivot et al 23 in Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution Study 2 cohort also reported a similar finding using a hypoperfusion intensity ratio generated from time thresholds when the residue function reaches its maximum (Tmax). However, HVR is different from the hypoperfusion intensity ratio. Indeed, HVR contains the spatial distribution of hypoperfusion and some information regarding the collateral flow filling efficacy as revealed by ASL with PLD from 1.5 to 2.5 s. Additionally, we found that HVR independently associated with recurrent ischaemic events, which indicated more severe baseline ischaemia might be associated with higher risk to have recurrent stroke, in accordance with a previous study that showed baseline National Institute of Health stroke scale was significantly associated with subsequent ischaemic events.24
Also, HRVWI has been used as a promising approach to detect atherosclerotic plaque vulnerability. Active plaque releasing microemboli is the main cause of embolism infarction in ICAS. Recently, it has been reported that plaque enhancement could be a useful imaging marker associated with the intraplaque inflammatory reaction that could then allow identifying the culprit lesion.9 In our study, plaque enhancement was observed in 37/43 (86%) of patients. In this symptomatic cohort, plaque enhancement was prevalent. However, no significant difference was detected between patients with or without 1 year ischaemic events. Our data showed that the predictive value of plaque enhancement was still not clear, and the role of haemodynamic impairments might outweigh plaque vulnerability in the evolution of stroke recurrence. The drawbacks of one-shot plaque enhancement for the evaluation of plaque vulnerability might attribute to such result. We speculate that plaque enhancement may be reliable to assess the current status of the culprit lesion. Indeed, since plaque enhancement usually changes with time, only those culprit lesions with persistent enhancement may contribute to the occurrence of a new embolism infarction. Further study is needed, however, to clarify this speculation.
Moreover, it should be noticed that the 1 year ischaemic events rate of this population was 7/43 (16.3%). Since all patients were treated by aggressive medical therapy, patients with severe hypoperfusion might not be able to restore perfusion in a short period only by aggressive medical therapy, when collateral circulation was lacking, and was therefore at a high risk of stroke recurrence. Thereby, haemodynamic impairments indexed by HVR may be valuable for patients’ selection for preventive intervention decision making in ICAS.
There are some limitations in the present study. First, the study sample was small. Correlation between HVR and collateral grades was performed in only 17 patients, which might limit the power and precision to detect more significant results. Second, ASL was limited by the PLD time which is currently no longer than 3 s.7 Total flow including antegrade and collateral flow may not reach the peak flow during this period. Therefore, exact hypoperfusion volume may be overestimated.6 Although measuring the exact final hypoperfusion volume would be ideal, the HVR that we proposed in this study can be interpreted as a relative hypoperfusion volume evolution along with delay time prolonging. It contains information about spatial and temporal changes. Third, we did not perform any comparative analysis between good and poor functional outcome (mRS >2) because only two patients had a poor outcome. Fourth, only MLN plaque enhancement was graded since a previous study reported that recurrent stroke might be related to proximal site enhancement of plaque.25 Fifth, no intraplaque haemorrhage was detected in this cohort since a previous study reported that intraplaque haemorrhage was as high as about 20% in symptomatic severe stenosis of the MCA, which might induce bias in the evaluation of plaque characteristics.26
Conclusion
Haemodynamic impairments may have played a critical role in the mechanism of stroke recurrence. HVR obtained from two PLD ASL may associate with collateral circulation and be useful for the prediction of recurrent stroke and therapy decision support in patients with ICAS. However, given the small number of analysed cohort, the present study may be viewed for hypothesis generation rather than to guide patient selection in clinical practice. Prospective studies are warranted.
References
Footnotes
Contributors Conception and design of the study: XL, NM, LM and XZ. Acquisition and analysis of data: JL, CT, FX and HS. Drafting a significant portion of the manuscript: JL and NM.
Funding This work was supported by The National Natural Science Foundation of China (contract grant number:81825012, 81730048, 81671126 to XL and contract grant number: 81471390 to NM).
Competing interests None declared.
Ethics approval The institutional ethics committee of the two hospitals approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.