Article Text

Abstract
The pathophysiology of giant cerebral aneurysms renders them difficult to treat. Advances in technology have attempted to address any shortcomings associated with open surgery or endovascular therapies. Since the introduction of the flow diversion technique, the endovascular approach with flow diversion has become the first-line modality chosen to treat giant aneurysms. A subset of these giant aneurysms may persistent despite any treatment modality. Perhaps the best option for these recurrent and/or persistent giant aneurysms is to employ a multimodal approach—both surgical and endovascular—rather than any single technique to provide a curative result with favourable patient outcomes. This paper provides a review of the histopathology and treatment options for giant cerebral aneurysms. Additionally, an illustrative case is presented to highlight the unique challenges of a curative solution for giant cerebral aneurysms that persist despite initial treatment.
- aneurysm
- flow diverter
- coil
- artery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Giant cerebral aneurysms (>25 mm) may be treated via endovascular or microsurgical means, with each approach having its own benefits, risks and technical challenges. They represent an extremely complicated subset of aneurysm pathology. Giant aneurysms may require a multimodal approach combining both endovascular and microsurgical approaches to achieve the best possible outcomes.
Pathophysiology
Giant aneurysms, defined as >25 mm, are histopathologically distinct. They have a loss of type I collagen and fibronectin in the adventitia and muscularis mucosa, respectively.1 Constant blood pulsations weaken the vessel wall, degenerate the internal elastic lamina and stretch the aneurysm dome.2 Scarring of the aneurysm wall results from the formation of thrombi within the wall and laminar necrosis. In addition, frequent microhaemorrhages in the aneurysm wall from parasitised vasa vasorum are subject to encapsulation and re-organisation by fibroblasts.3 These fibroblasts produce connective tissue that reinforces the wall while still permitting it to grow.4 5 These recurrent haemorrhages have been postulated to be the cause of a giant aneurysm’s slower growth rates compared with smaller aneurysms.6 Certain locations, such as the ophthalmic and cavernous segments of the internal carotid artery (ICA), are more likely to allow for the development of giant aneurysms due to the adjacent anterior clinoid process as well as the dura of the cavernous sinus which each partially shield the aneurysm dome and buttress it against haemodynamic forces that might otherwise cause rupture.7
Treatment options
Microsurgical techniques
Microsurgical intervention for giant aneurysms has been reported dating back to the 1950s.8 It has varying success depending on the specific intervention selected, with the most common being clipping or aneurysm trapping with extracranial–intracranial bypass. Mortality has been reported at least 6% and up to 13%, whereas favourable clinical outcomes range from 71% to 80% in most series.9–12
Gewirtz and Awad reported the results of 35 patients treated with microsurgical clipping for giant aneurysms of the anterior circulation. Twenty-six (68%) of these patients presented with subarachnoid haemorrhage. Thirty-three were treated with one or more clips across the aneurysm neck, and two were treated with aneurysm trapping. Thirty-four of 35 (97%) giant aneurysms were completely obliterated and patency of all of the parent arteries was achieved in 30 cases (86%). The clinical outcome, as defined by authors, was 34% ‘excellent’, 37% ‘good’, 14% ‘fair’, 9% ‘poor’ and 6% ‘death’. Nine patients suffered neurological morbidity and mortality was 6% with good or excellent clinical outcomes in 71%.10 Similarly, Nanda et al conducted a study of 59 giant aneurysms treated by surgical clipping by a single surgeon. Forty-eight had anterior circulation and 11 had posterior circulation aneurysms. The mortality rate was 10.1% (11 patients). The majority (71.9%) experienced a good outcome (Glasgow Outcome Score (GOS) of 4 or 5). Predictors of the poor outcome included ruptured aneurysm, poor clinical outcome and posterior location.12 Additionally, in Cantore et al’s series on 58 patients with giant aneurysms treated with surgical clipping, the mortality rate was 6.9% and clinical improvement 94.4%.9
Microsurgical clip reconstruction requires some form of aneurysmal neck, even if it is broad and fenestrated or encircling clips can be implemented for reconstruction. The option of bypass must be entertained if clip deployment obstructs the patency of one or more arteries. Temporary trapping is required along with blood pressure augmentation in order to enhance collateral flow while temporary clips are placed. The aneurysm can then be punctured and decompressed, however, if a significant thrombus is present, endoaneurysmectomy must be performed.13 Multiple bypass approaches exist including direct vessel reimplantation, side-to-side vessel anastomosis, low-flow extracranial-intracranial bypass and high-flow extracranial–intracranial (EC-IC) bypass.14–18 A bypass is done under burst suppression and temporary clip occlusion. Once the bypass is complete, patency is verified via the micro-Doppler technique along with an intraoperative angiogram. The aneurysm is then subsequently treated during the same operation via trapping or occlusion. If proximal occlusion were to obstruct branch vessels or perforators, distal occlusion can be done.19 20 Cantore et al reported results on 41 patients with giant aneurysms managed with high-flow EC-IC bypass. Four (9.8%) died and 34 (91.9%) improved. Graft patency at the follow-up examination was 92.7%.9
The use of deep hypothermic circulatory arrest with microsurgical clipping or bypass approaches is a modality that has waned in popularity. The procedure has an unpredictable recovery after circulatory arrest, with treatment complications approaching 40% with an additional 20% medical complications such as cardiac arrhythmias, pneumonia, sepsis, seizures and pulmonary embolism. Postoperative haemorrhage is also of significant concern.21 22 The 30-day perioperative mortality ranges from 12% to 18%. Temporary pharmacological cardiac standstill with adenosine has replaced deep hypothermic circulatory arrest with a more acceptable risk profile.8
Endovascular options
Balloon test occlusion with vessel sacrifice
Proximal occlusion of giant aneurysms via endovascular parent vessel sacrifice is feasible when appropriate collateral circulation exists. Preoperative testing of the adequate circle of Willis collateral circulation is most commonly performed with temporary balloon test occlusion (BTO). However, patients who pass BTO still harbour a 5%–25% risk of ischaemic stroke after parent vessel sacrifice secondary to haemodynamic and thromboembolic causes. Both a BTO without the development of neurological deficit and a transcranial Doppler demonstrating no >30% drop in the middle cerebral artery velocity from baseline should be demonstrated prior to embolisation.23 Complications related to BTOs with associated vessel sacrifice include transient ischaemic attacks from relative ischaemia, thromboembolic strokes and development of aneurysms.24
Coil embolisation
Coil embolisation of giant cerebral aneurysms is associated with significantly high retreatment rates. Chalouhi et al studied 334 large and giant aneurysms (80% anterior circulation) that were coiled at a single institution. Thirty-two (10%) were giant aneurysms. Recanalisation and retreatment rates were 39% and 33%, respectively.25 Recanalisation is highest in the setting of wide residual aneurysm necks, largely due to coil compaction, growing residual aneurysm neck, and refilling fundus.3 26 27 Fernandez et al series with 51 wide-necked aneurysms (necks>4 mm) treated with coil embolisation reported complete thrombosis was observed in only 15%.28 Additionally, Horowitz et al’s retrospective study evaluating aneurysm recurrences or subtotal initial coil embolisation found seven of the nine patients requiring repeat treatment were secondary to coil compaction.26 Comparatively, Hasan et al demonstrated in a study of 175 coiled aneurysms, 8 had major recurrences resulting from significant aneurysm sac growth (15% to 102% increase), independent of change in coil volume.27
Vascular reconstruction devices (VRD), such as Neuroform Atlas Stent (Stryker Neurovascular, Fremont, California, USA), Low-profile Visualised Intraluminal Support (LVIS; Microvention, Tustin, California, USA) and PulseRider (Cerenovus, Irvine, California, USA), were designed to augment coil embolisations of wide-neck aneurysms. An in vitro study demonstrated that these devices reinforce embolisation by improving coil neck coverage and increasing coil packing density.29 Both LVIS Jr and Neuroform Atlas stents provide low profile advantages with delivery through a 0.017-inch microcatheter. Several centres have published procedural successes with both VRDs in Y-stent assisted coilings for wide-necked aneurysms.30–32 In comparison with the tubular constructs of LVIS Jr and Neuroform Atlas VRDs, the PulseRider stent was uniquely designed in two distinct shapes, T or Y, with the intention to address coiling challenges of wide-necked bifurcation aneurysms. The Adjunctive Neurovascular Support of Wide-neck Aneurysm Embolization and Reconstruction (ANSWER) Trial evaluated PulseRider efficacy in the treatment of 34 bifurcation aneurysms. Of the treated aneurysms, 82.4% achieved immediate Raymond I or II occlusion and at a 6-month follow-up, the rate increased to 87.9%.33 These results led to the US Food and Drug Administration (FDA) approval in 2017. Although VRDs are used as procedural adjuncts for the treatment of giant aneurysms, recanalisation rates remain high given the challenging pathology of giant aneurysms.26 27 29
Flow diversion embolisation
Flow diversion is the newest endovascular technique specifically designed for the treatment of giant aneurysms. Flow diversion is fundamentally based on two concepts: (1) the placement of a high-density mesh device in the parent vessel disrupts blood flow into the aneurysm, resulting in progressive intra-aneurysmal thrombosis and (2) the device provides a scaffold for which endothelial cells can grow to isolate the aneurysm from the parent artery with subsequent radiographic obliteration of the aneurysm.34 Since the initial introduction of flow diversion in the 2000s, there have been a number of publications on the proven efficacy in durable curative treatments of giant aneurysms as well as safety with morbidity and mortality rates less than open microsurgical clipping.34–44
In the USA, the Pipeline Embolisation Device (PED; Medtronic Neurovascular, Irvine, California, USA) and the Surpass flow diverter (Surpass; Stryker Neurovascular, Fremont, California, USA) are the only two flow diverter devices approved by the FDA. A large, single-centre study looking at outcomes after PED flow diversion of anterior circulation aneurysms to identify predictors of occlusion and aneurysm persistence was performed by Bender et al. Four hundred forty-five PED procedures were performed, with 85 large (19%) and 4 giant (1%) aneurysms. Complete occlusion was achieved in 72%, 78% and 87% at 6, 12 and 24 months, respectively. The overall rate of major complications was 3.5%, including a 1.1% rate of a major stroke, a 1.8% rate of intracranial haemorrhage and a 0.7% rate of subarachnoid haemorrhage, leading to 1.1% rate of mortality. Further analysis revealed that at 12 months, adjunctive coiling predicted occlusion, whereas male sex, aneurysm size and incorporation of a branch vessel predicted aneurysm persistence. Prior treatments, vessel of origin, fusiform morphology and number of devices used did not predict aneurysm occlusion.39
Comparatively, the Surpass Flow Diverter (Surpass; Stryker Neurovascular, Fremont, California, USA) is the second flow diverter available in the USA after FDA approval in 2018. Approval was based on results of the SCENT Trial (Surpass IntraCranial Aneurysm Embolization System Pivotal Trial to Treat Large or Giant Wide Neck Aneurysms) designed as a multicentre, prospective, single-arm, non-randomised, interventional trial of the Surpass Flow Diverter for uncoilable or previously treated but failed aneurysms of the intracranial ICA extending from the petrous segment to the carotid terminus. All aneurysms had a wide neck (>4 mm) and large or giant size (>10 mm).42 One-hundred eighty aneurysms were treated at 26 medical centres. The mean aneurysm size was 12.0 mm with 13 (7.4%) giant aneurysms. Unlike the clinical trial for PED FDA approval PUFS (Pipeline for Uncoilable or Failed Aneurysms), the majority of the aneurysms treated in SCENT were intradural in location, beyond the cavernous ICA. The device was successfully implanted in 97.8% of patients. SCENT met both primary safety (major ipsilateral stroke or neurological death within 12 months) and effectiveness (complete aneurysm occlusion, absence of significant parent artery stenosis (>50%), and no retreatment at 12 months) endpoints: 12-month primary effectiveness rate was 62.8% ((113/180); 95% CI: 55.3 to 69.9) and 12-month major ipsilateral stroke or neurological death rate was 8.3% ((15/180); 95% CI: 4.7 to 13.4). With these results, Surpass provides safe and effective flow diversion of large or giant, wide-neck ICA aneurysms.42
Combined microsurgical and endovascular options
Giant aneurysms represent complex and challenging aneurysms to treat despite open microsurgical and endovascular advances. There are several reports of using combined microsurgical and endovascular approaches with good results. In Arnautović et al’s study, eight patients with giant paraclinoid aneurysms underwent endovascular balloon occlusion of the ICA with suction decompression of the aneurysm, followed by clip ligation. Postoperative results were ‘good’ (defined by the ability to return to the patient’s usual preoperative activities) in seven of eight patients (87.5%) and fair in one of eight patients (12.5%). This patient experienced right-sided hemiplegia and expressive aphasia.45
Lawton et al retrospectively reviewed 96 aneurysms, 18 of which were giant aneurysms, treated with multimodality therapy. In each patient, multimodality therapy was initiated for aneurysm occlusion in one of the following eight combinations: (1) selective revascularisation and aneurysm occlusion, (2) endovascular and surgical trapping, (3) clipping of aneurysm after attempted or incomplete coiling, (4) coiling after attempted or incomplete clipping, (5) clipping of recurrent aneurysm after coiling, (6) coiling of recurrent aneurysm after clipping, (7) coiling after previous surgery, and (8) clipping and coiling of multiple remote aneurysms. Morbidity was 11% and mortality was 11% with combined treatment.46 Lin et al identified anterior communicating artery region aneurysms with recurrences after microsurgical clipping that were subsequently treated with PED. Nine PED were performed for six recurrent aneurysms without any complications. Five of the six (83%) demonstrated complete occlusion, therefore, flow diversions with PED is an option following recurrences after surgical clipping.47 Ponce et al conducted a study of nine giant aneurysms treated with vascular bypass and endovascular parent artery occlusion. There was one case of hydrocephalus, one ischaemic stroke, three epidural haematomas and two deaths.48 In a separate study by Serbinenko et al, nine patients with giant ICA aneurysms were treated with combined EC-IC bypass and endovascular ICA occlusion. There no complications reported.49 Hoh et al treated 48 fusiform and complex wide-necked aneurysms with endovascular occlusion and either vascular bypass, clip ligation or both. In patients with giant aneurysms, GOS was 5 in two patients and 4 in two patients; one patient death was reported.50
The following case serves as an example to illustrate some of these challenges and highlight the potential need for a combined endovascular and microsurgical approach for definitive treatment.
Case example
A sexagenarian presented to another institution with progressive vision loss in the left eye while abroad in the UK. After admission to the hospital, workup revealed a giant non-ruptured 50 mm left PCoA aneurysm. Primary endovascular treatment with stent-assisted coiling was performed. Per documentation, the follow-up demonstrated persistent filling of the aneurysm dome and the outside institution chose treatment with an endovascular flow diverter, the PED. In the periprocedural period, the patient suffered a left-sided intracranial haemorrhage resulting in right-sided hemiplegia and global aphasia. In the setting of intracerebral haemorrhage, the patient’s dual antiplatelet medications were discontinued.
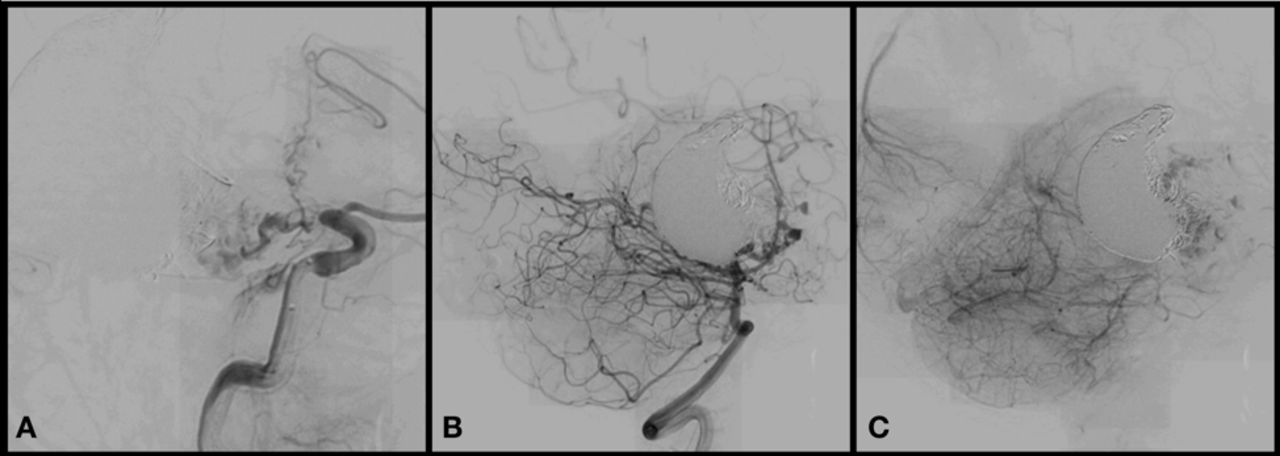
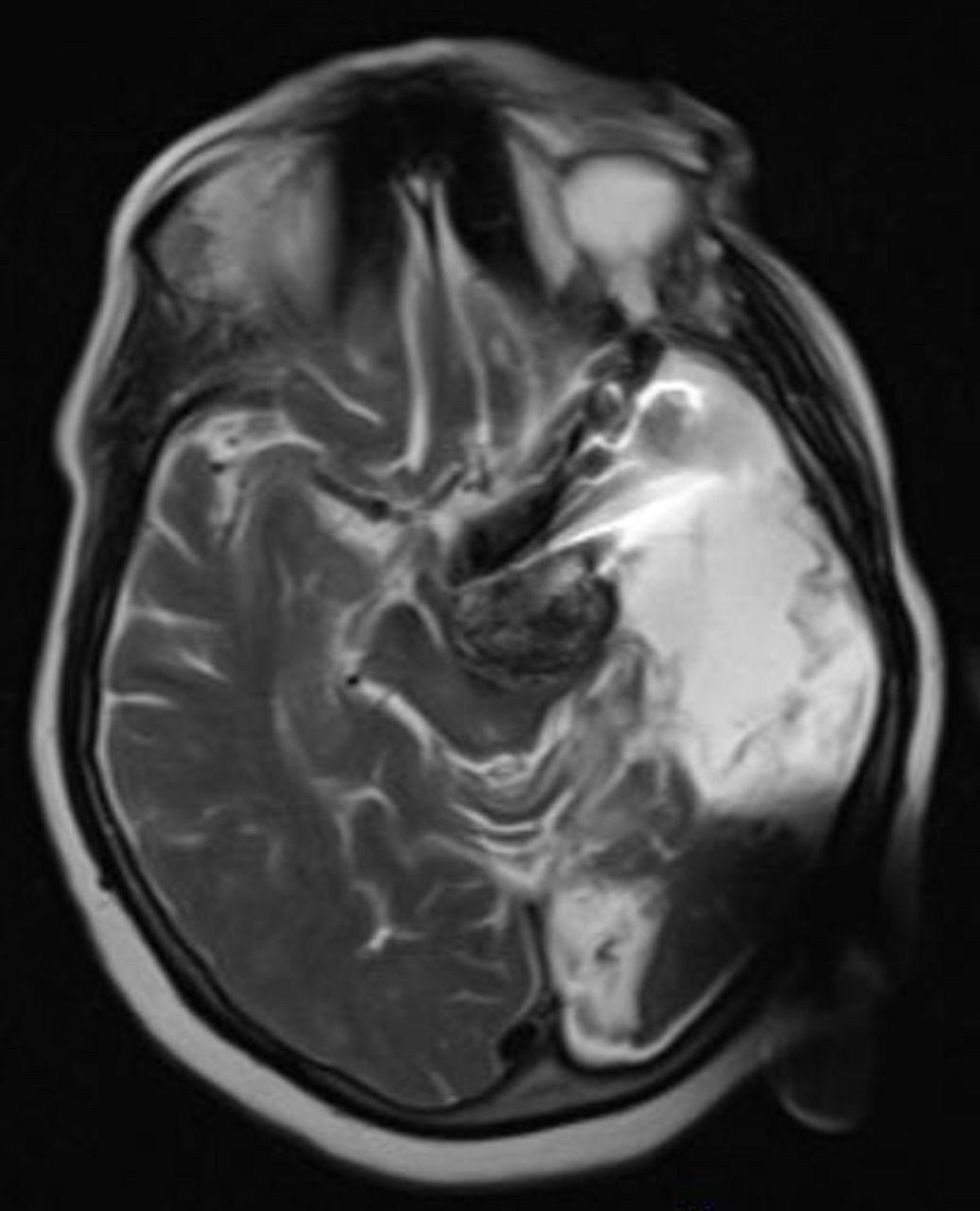
After returning to the USA, the patient continued to decline neurologically, developing left-sided dense hemiparesis over the course of several months. The family brought the patient to our institution with limited records and no preprocedural imaging. New cerebral angiography demonstrated occlusion of the distal intracranial left ICA terminating in the persistent giant PCoA aneurysm (figure 1A). In addition, the PCoA aneurysm also filled during posterior circulation injections (figure 1B and C). Direct compression of the aneurysm on the descending corticospinal tracts in the brainstem was believed to be the cause of the patient’s subacute contralateral neurological decline and warranted treatment (figure 2). A temporary balloon occlusion test of the left ICA revealed adequate collateral filling from the contralateral ICA and the posterior circulation.
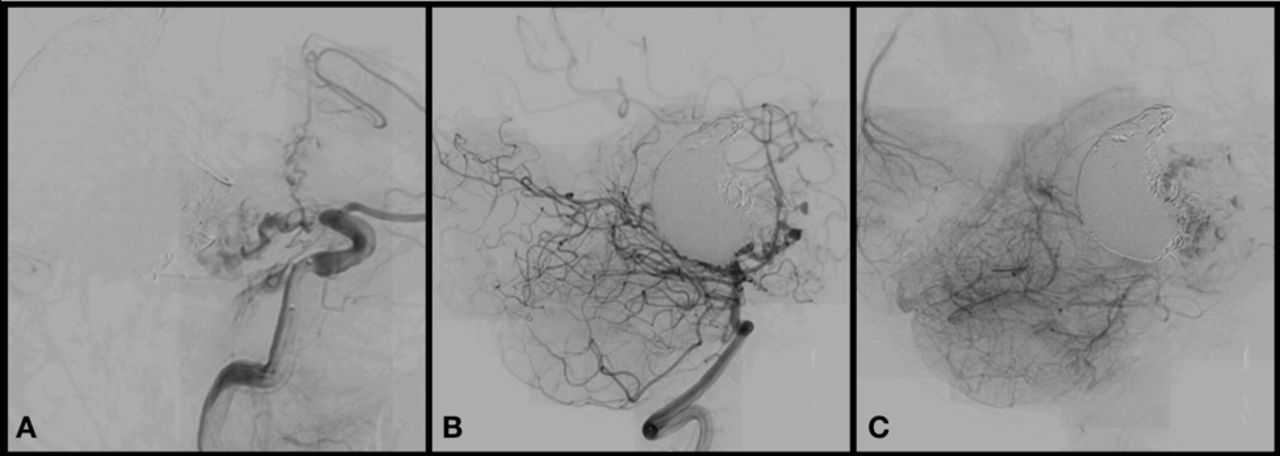
Giant, non-ruptured, 50 mm left PCoA aneurysm that persisted after initial endovascular treatment. (A) DSA (lateral view) of left internal carotid artery demonstrating partial filling of a persistent giant PCoA aneurysm treated first with stent-assisted coiling followed by flow diversion with the pipeline embolisation device. (B) DSA (lateral view) of left vertebral artery demonstrating partial filling of the aneurysm from the posterior circulation in mid-arterial (B) and late-arterial (C) phases. DSA, digital subtraction angiogram; PCoA, posterior communicating artery.

MRI reveals a mass lesion with brainstem compression. Axial cranial T2 MRI demonstrating a partially thrombosed persistent giant PCoA aneurysm causing brainstem compression. MRI, magnetic resonance imaging; PCoA, posterior communicating artery.
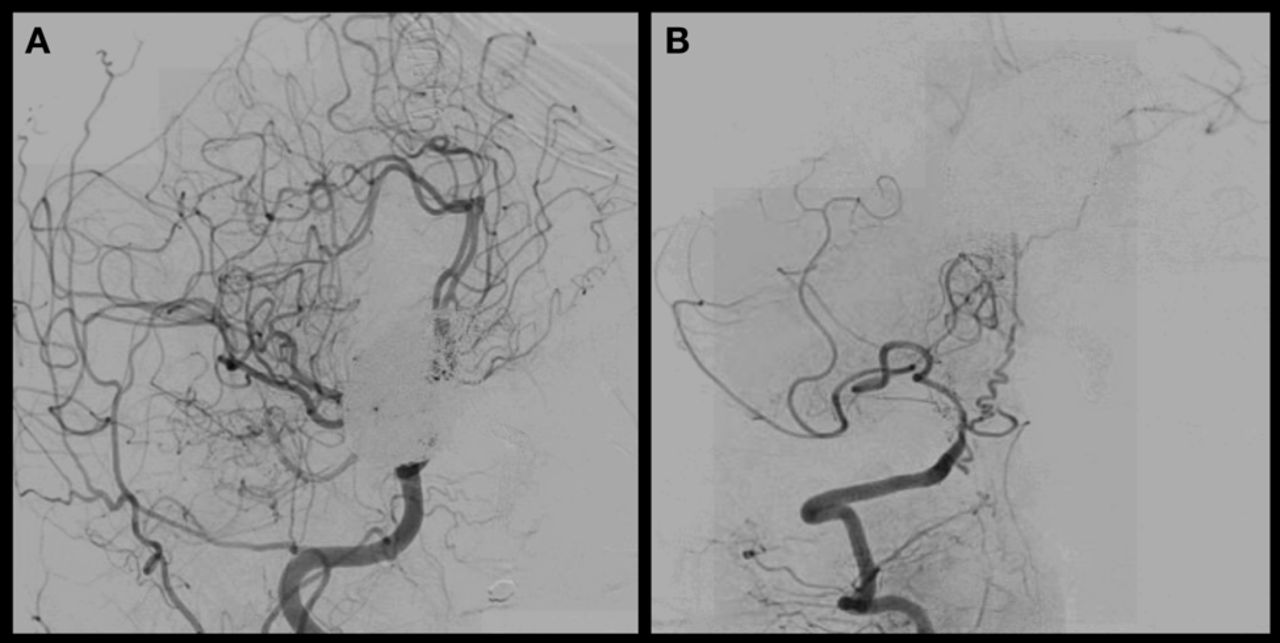
A combined endovascular and microsurgical approach was chosen to address the residual aneurysm with goals to decompress the mass effect of the giant aneurysm and secure the dome. Initial endovascular coil occlusion of the left ICA was performed. The following day, a left modified orbitozygomatic craniotomy was performed to isolate the aneurysm sac from the posterior communicating artery PCoA (posterior communicating artery) and decompress the sac. Visualisation of the aneurysm dome revealed parasitised pial vessels. The aneurysm dome was debulked revealing multiple embolisation coils, associated thrombus and the prior PED was visualised in the parent ICA (figure 3). After coil removal, the neck of the aneurysm was visualised from the inside and clipped inside-out. A micro-Doppler was used intraoperatively to confirm that the residual aneurysm dome demonstrated no residual filling from either the ICA or the PCoA. Postoperative angiogram confirmed no residual aneurysm filling from either anterior or posterior circulation (figure 4A and B) and delayed postoperative MRI demonstrated significant decompression of the brainstem (figure 5).

Microsurgical aneurysm debulking and clipping following endovascular coil occlusion of left internal carotid artery for treatment of a persistent giant PCoA aneurysm. Intraoperative image with the pipeline embolisation device flow diverter visualised through the debulked PCoA aneurysm dome. PCoA, posterior communicating artery.
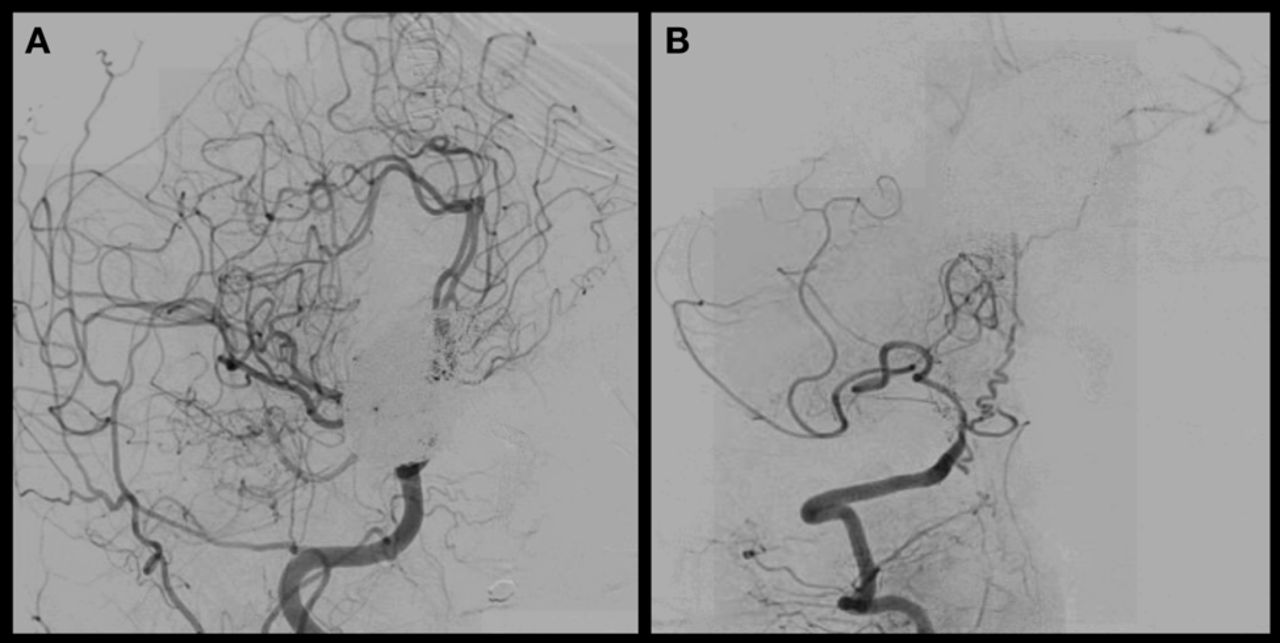
Postoperative cerebral angiography following endovascular coiling of the left internal carotid artery and microsurgical aneurysm debulking and clipping of a giant left PCoA aneurysm. Postoperative angiography of the (A) right lateral internal carotid artery and (B) vertebral artery cerebral demonstrating complete occlusion of the giant PCoA aneurysm. PCoA, posterior communicating artery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Delayed postoperative MRI following endovascular coiling of the left internal carotid artery and microsurgical aneurysm debulking and clipping of a giant left PCoA aneurysm. Delayed postoperative axial T2 MRI demonstrating the residual coil mass in a thrombosed giant PCoA aneurysm, with significant reduction in brainstem compression compared with preoperative MRI. Artifact from coil mass and aneurysm clips. MRI, magnetic resonance imaging; PCoA, posterior communicating artery.
The patient recovered from this surgery without any new focal neurological deficits and was discharged from the hospital on post-operative day 14. At the time of discharge, the patient was awake and alert with continued right-sided hemiplegia and global aphasia, and improvement in left-sided strength from dense hemiparesis to attempted localisation with noxious stimulation. The patient was last evaluated in the clinic 36 months postoperatively and has continued to improve. Currently, the left-sided strength is 4/5 in all muscle groups and the right leg has regained strength proximally to 3/5 power. The patient follows commands and attempts to vocalise words.
Discussion
Giant aneurysms, notably supergiant aneurysms (>50 mm), represent complicated dome histopathology and a single surgical modality may not be sufficient to address the various disease components. Open microsurgery lends to immediate dome occlusion but may be fraught with high morbidity.45 46 48 51 52 In contrast, conventional endovascular treatment with endosaccular coil embolisation is associated with known risks of recurrence, whereas parent vessel remodelling through flow diversion with delayed complete aneurysm occlusion can lead to aneurysm growth.39 53 Additionally, a curative result from flow diversion treatment of the more fusiform and supergiant aneurysms becomes limited given the challenges of achieving endothelialisation along a longer length of device construct without a wall. The management of complex residuum or recurrences in giant aneurysms can be particularly challenging with conventional microsurgical and endovascular techniques.34 37 54
A combination approach of endovascular and open microvascular techniques may more adequately address the precarious situation of partial aneurysm thrombosis and the complex histology of parasitised giant aneurysm domes. Such an approach may allow for greater total occlusion rates and better patient outcomes. Specifically, the debulking of the aneurysm dome can limit its mass effect on surrounding critical structures. Both patient-specific and surgeon-specific factors must be considered in the context of each individual case to determine the most appropriate intervention.
In the aforementioned case illustration, the giant PCoA aneurysm persisted following stent-assisted coiling and treatment with the PED flow diverter. Given the patient’s worsening neurological examination and imaging suggestive of direct aneurysmal compression on the brainstem, a combined endovascular and microsurgical approach was undertaken that included ICA coil sacrifice followed by debulking of the aneurysm dome and internal clipping. This combination approach, rather than a single surgical modality, was chosen to address both curative aneurysm occlusion and the vasculopathology of aneurysm dome parasitisation.
Ding et al reported a similar case in which a giant posterior cerebral artery aneurysm persisted following endovascular treatment with two PEDs. However, in that case, the aneurysm’s continued growth led to obstructive hydrocephalus. An open microsurgical approach was then taken to secure and decompress the aneurysm dome. Following surgery, postoperative venous infarcts occurred, which lead to a complicated postoperative course and death.55
There are several reports in the literature of combined concomitant endovascular and microsurgical interventions for giant intracranial aneurysm.45 46 48–50 Reported techniques include selective revascularisation and aneurysm occlusion, endovascular and surgical trapping, EC-IC bypass with parent vessel occlusion, flow redirection, or arterial transposition, intraoperative temporary balloon occlusion with aneurysm clipping, clipping after attempted or incomplete coiling, and coiling after attempted or incomplete clipping. These reports have yielded overall promising results (table 1).
Literature review of giant intracranial aneurysms treated with combined concomitant endovascular and microsurgical interventions.
Conclusions
No single approach may be the panacea for giant and particularly super-giant intracranial aneurysms. As microsurgical and endovascular techniques continue to refine, evidence suggests multimodal evaluation and treatment warrants greater consideration for these select cases often with distinct histopathology where the aneurysm dome harbours parasitised pia vessels. Our case example demonstrates a successful combined approach in a patient with multiple failed endovascular attempts of treating a supergiant intracranial aneurysm. This case may serve as a basis for further investigation of multimodal management of difficult to treat supergiant aneurysms.
References
Footnotes
Twitter @drjessicacampos
Contributors JKC, BZB, BCII, ASW, AJS and BJH: participated in literature search and drafted the manuscript. FPKH: assisted with patient management. L-ML: conceptualised and critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests L-ML is a consultant/proctor for Stryker Neurovascular and a consultant for MicroVention & Cerenovus.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.