Article Text

Abstract
Introduction Approximately 40% of strokes in young adults are cryptogenic. The diagnostic yield of thrombophilia screening remains controversial. We aimed to determine utility of current thrombophilia testing for young patients with stroke and transient ischaemic attack (TIA).
Methods We present a retrospective review of all patients with stroke and TIA ≤60 years presenting to University College London Hospital stroke unit and daily TIA clinic from 1 January 2015 to 1 August 2016. Consecutive clinical records and thrombophilia tests, including factor V Leiden (FVL), prothrombin G20210A mutation (PGM), antiphospholipid antibody (APA), and protein S, C and antithrombin (AT) levels, were reviewed.
Results The mean age of 628 patients with stroke and TIA was 49.1 years (SD 9.2). Thrombophilia testing was performed in 360 (57%) patients, including 171 with stroke and 189 with TIA. Positive tests were found in 50 (14%) patients, of whom 24 patients were <50 years. Positive results were found in 36 (10%) with acute ischaemic stroke, 4 (1%) with haemorrhagic stroke and 10 (3%) with TIA. Thirteen patients (4%) had homozygous/heterozygous FVL or PGM, and 27 (7.5%) had positive APA (anticardiolipin antibody, anti-β2 glycoprotein antibody or lupus anticoagulant). Of 27 (7.5%) patients with protein C, S or AT deficiency, 10 (2.8%) had primary deficiency, presumed hereditary with other secondary causes excluded. 9% of patients with protein C, S or AT and 27% with APA were followed by confirmatory testing.
Conclusion Thrombophilia testing was positive in only 14% of cases overall. Thrombophilia mutations and protein C, S or AT abnormalities were found rarely and were very uncommon in patients with TIA. Follow-up of abnormal results was generally poor for all groups, which further limited the impact of the thrombophilia testing policy.
- thrombophilia testing
- young stroke
- transient ischaemic attack
- antiphospholipid antibody
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In comparison with older individuals, young stroke pathogenesis is more pleomorphic, with a higher representation of uncommon causes such as dissections, cardiac arrhythmia and thrombophilia.1 2 These aetiological differences often necessitate additional investigations, including complex thrombophilia screening, but the utility of extensive thrombophilia work-up in young patients with stroke and transient ischaemic attack (TIA) is not established.
Thrombophilias are broadly defined as inherited or acquired coagulation disorders predisposing to thrombosis.3 4 Antithrombin (AT), protein C and S deficiency, factor V Leiden (FVL) and factor II mutations are rare inherited thrombophilias associated with an increased risk of venous thrombosis, but their relation to arterial ischaemic stroke and TIA is less well established.5–16 Accurate diagnosis and clinical relevance of AT, protein C and S deficiency to acute stroke are quite complex, since assays are usually influenced by active illness, concurrent medical conditions, and medications such as oral contraception and anticoagulation.17–24 Hence, repeat testing is recommended in order to distinguish false-positive diagnoses from genuine AT, protein C and protein S deficiencies.25
Antiphospholipid syndrome is an autoimmune thrombophilia characterised by recurrent arterial or venous thrombosis and/or pregnancy morbidity, and presence of persistent antiphospholipid antibodies (APA).26 A large prospective study showed that antiphospholipid syndrome manifests as stroke and TIA in 2.4% and 2.3% of cases, retrospectively.27 There are three types of APA with different phospholipid binding sites: lupus anticoagulant (LA), anticardiolipin antibody (ACL) of IgG or IgM subtype, and anti-β2 glycoprotein 1 (anti-β2GPI) of IgG or IgM subtype. The interpretation of positive APA results in the context of arterial thrombosis requires careful consideration of antibody type, isotype and titre, in the individual clinical context.26 Among APAs, the specificity for arterial thrombosis is higher for LA and anti-β2GPI.28–31 In addition, among patients with thrombosis, the highest risk of recurrence is the relatively small cohort positive for triple APA.32 Since APA can be transiently positive after acute illness, it is recommended to repeat it at least 3 months after stroke to distinguish definite antiphospholipid syndrome.26 In our study, we evaluated acute stroke admissions potentially eligible for more intensive cholesterol treatment.
Thrombophilia testing in young patients with stroke often includes protein C, S and AT levels, genotyping for FVL and prothrombin G20210A mutation (PGM), and APA testing. This complex and costly testing is often routinely sent despite limited evidence linking hereditary thrombophilia to arterial thrombosis; moreover, in practice, only a small proportion of initial abnormal results are further followed up by appropriately timed repeat testing.
The present study aimed to determine our current practice of assessing positive thrombophilia testing in the context of young stroke and TIA.
Methods
We performed a retrospective evaluation of consecutive cases within a single regional hyperacute stroke unit and daily TIA clinic at University College London Hospital, the main referral centre for North Central London. We reviewed consecutive medical and laboratory records of all patients with acute ischaemic stroke (AIS), haemorrhagic stroke and TIA 60 years and under presenting to the service from 1 January 2015 to 1 August 2016. The standard thrombophilia panel included genotyping for FVL and PGM, AT activity, protein C and S antigen and activity, and APA testing.
APA testing was conducted for LA (using dilute Russell viper venom time and/or Taipan venom time methodology according to whether the patient was anticoagulated), ACL IgG/IgM and anti-β2GPI IgG/IgM (ELISA). Laboratory criteria for positive APA were considered in accordance with the Miyakis criteria, which include the following: (1) LA present; (2) ACL (either IgG or IgM) in medium or high titre, that is, >40 GPL units or MPL units (defined as the cardiolipin-binding activity of 1 g/ml of affinity-purified IgG or IgM ACL), or >99th centile; and (3) anti-β2GPI (IgG or IgM) in titre >99th centile. ACLs with low titres were excluded.
In all those with initial positive thrombophilia testing (defined as homozygous or heterozygous FVL or PGM, presence of APA, low protein S, C and AT), clinical and laboratory records were reviewed by the stroke and haematology physicians for acquired causes, stroke characteristics and whether appropriate follow-up had been arranged. The Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification was used to subtype ischaemic stroke and the ABCD2 score was used for TIA risk assessment.
The estimated final costs for thrombophilia testing were based on the University College London Hospital NHS Trust’s pathology pricing model at the time of the study, 1 January 2015–1 August 2016, and are outlined in online supplementary table 1.
Supplemental material
Baseline characteristics of thrombophilia screen-positive patients (n=50)
Results
Six hundred and twenty-eight patients were ≤60 years: 383 (61%) AIS, 202 (32%) TIA and 43 (6.8%) haemorrhagic stroke. The mean age was 49.1 years (SD 9.2).
Three hundred and sixty (57%) patients had thrombophilia testing: 171 (40%) stroke and 189 (94%) TIA. Abnormal results were returned in 70 (19%) patients. Twenty were later excluded from this cohort on secondary screening, 17 with acquired protein C, S or AT deficiency, and 3 with negative confirmatory APA testing of initial positive APA (figure 1).

Outcome of thrombophilia testing for the whole cohort (A) and separated for TIA and stroke (B). APA, antiphospholipid antibody; AT, antithrombin; FVL, factor V Leiden; LFT, liver function test; PGM, prothrombin G20210A mutation; TIA, transient ischaemic attack.
A total of 50 (14%) patients, including 27 (8%) patients with positive APA, 13 (4%) homozygous or heterozygous for FVL or PGM, and 10 (3%) presumed genuine protein C, S or AT deficiency, were analysed: 36 (10%) AIS, 4 (1%) haemorrhagic stroke and 10 (3%) TIA. The median vascular risk factor of these 50 patients was 1 (IQR 0–5) (table 1). Of 50 patients with positive thrombophilia testing, 36 had AIS and 10 had TIA, 2 (4%) had carotid artery stenosis >70%, 6 (13%) had lacunar syndrome, 14 (30%) were cardioembolic, 4 (9%) had vertebral or internal carotid artery dissection and 20 (43%) had other determined aetiology.

{kind=link}
{kind=link}
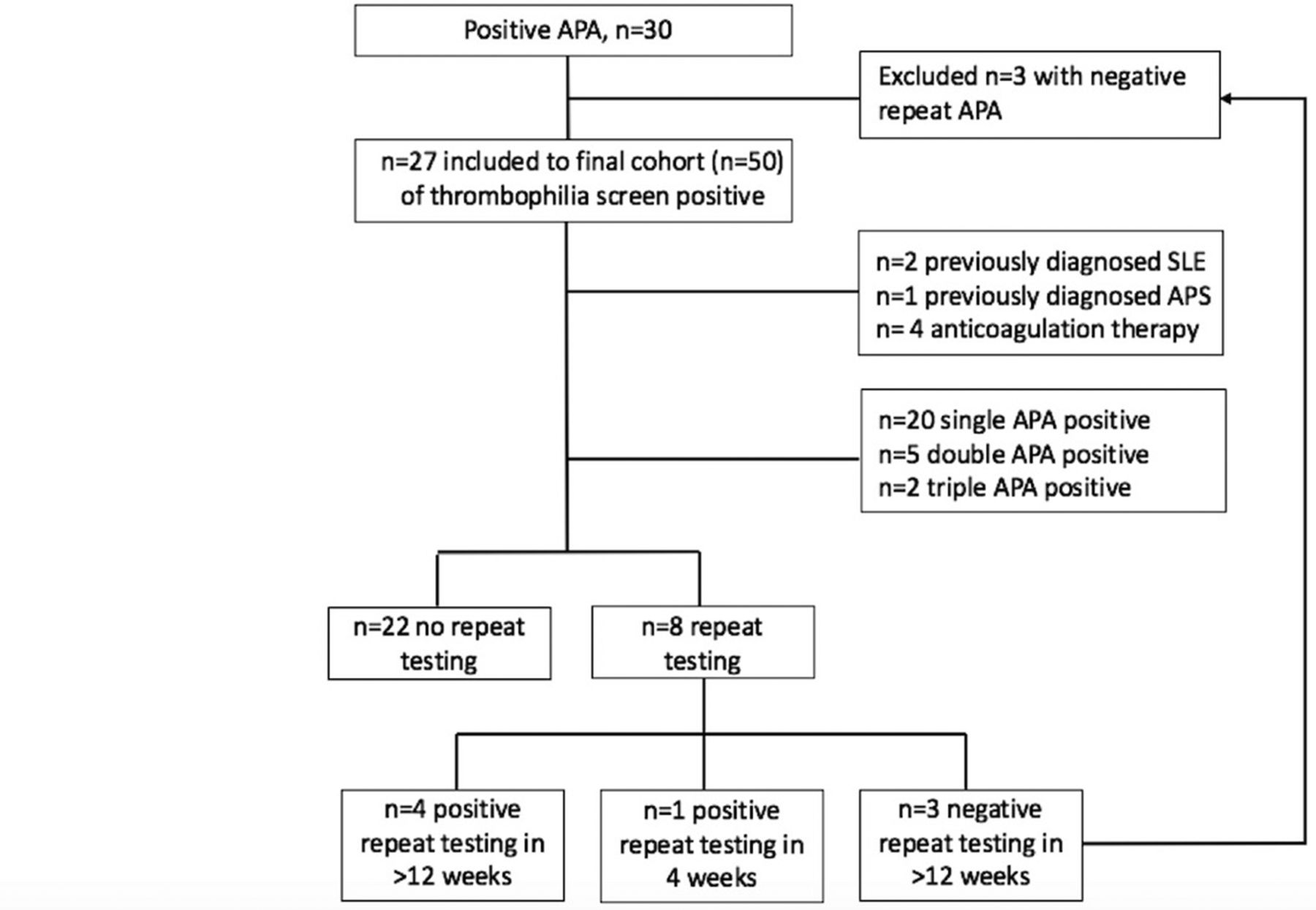
Outcome of antiphospholipid antibody testing-positive cohort. APA, antiphospholipid antibody; APS, antiphospholipid syndrome; SLE, systemic lupus erythematosus.
Twenty-four of 243 patients (9.9%) <50 years were thrombophilia testing-positive. There was no significant difference in those <50 years vs 51–60 years (p=0.15).
Of 27 (8%) positive for an APA, 20 (6%) were single antibody-positive, 5 (1%) double antibody-positive and 2 (0.6%) triple antibody-positive (figure 2). Four patients who were on anticoagulation therapy were included, although APA was not repeated after stopping anticoagulation and false positivity could not be confirmed. Three cases with medical history of systemic lupus erythematosus (SLE) and antiphospholipid syndrome were also on anticoagulation therapy.
Of 360 patients tested for standard thrombophilia, 94% were screened for both LA and ACL antibodies and 3% for ‘triple APA’ including LA, ACL and anti-β2GPI antibodies. Of 30 patients with initial positive APA, only 8 (27%) were followed by repeat APA testing.
Of 189 thrombophilia-tested TIA cases, 10 (5%) were positive and 9 (5%) with APA. Four presented with amaurosis fugax, all of whom were APA-positive. Thrombophilia mutations and protein C, S or AT deficiency were rarely positive in this group (0.5%). The positive cases included two cardioembolic, four small vessel disease, one case with SLE and three cases with a cryptogenic aetiology at the time of initial work-up (table 2). The median ABCD2 score of positive cases was 4.5 (IQR 1–5).
Thrombophilia test-positive stroke and TIA
The thrombophilia panel cost per patient ranged from £245.67 to £373.19 (online supplementary table 1). More than 94% of patients had thrombophilia test that included FVL, PGM, ACL, LA, protein C and AT functional assays, and free protein S quantification tests. Additional confirmatory tests included protein C and AT quantification, protein S functional assay and anti-β2GP1 antibody.
Discussion
There is no clear consensus on the age range of ‘young adult stroke’; most studies of this age group include young adults from 15 to 50 years. We included patients with stroke and TIA of 60 years and under into the category of ‘young adult stroke and TIA’, and analysed 51–60 years and <50 years age groups separately. This subgroup analysis showed an even distribution of positive thrombophilia testing among 51–60 and <50 age groups. Young-onset stroke and TIA are more heterogeneous than for older patients, and typical aetiologies include both traditional cardiac and large vessel atheroma, as well as a higher prevalence of ‘rarer’ aetiologies including arteriopathies, inflammatory or otherwise, cardiomyopathy and prothrombotic states. Based on the TOAST classification of ischaemic stroke, ‘stroke of other determined origin’ is traditionally deemed correspondingly highest in the younger age group. This was also represented in our thrombophilia-screen positive AIS and TIA cohorts, with 61% of the diagnosis falling into ‘stroke with other, determined or undetermined origin’ category. Nine per cent of cases with cervical artery dissection were included into this category that likely resulted from trauma and were coincidentally positive to thrombophilia screen.
In practice, patients with young stroke and TIA undergo additional investigations, including complex thrombophilia screening, despite weak association with arterial thrombosis and hereditary thrombophilia. In our institution, prior to this study, complex thrombophilia screening was indicated for all patients with AIS and TIA younger than 50 independent of vascular risk factors profile. There was no selection bias. Similarly, in our cohort screened for thrombophilia, only 3.6% of the individuals were carriers of FVL or PMG. This association was even less for patients presenting with TIA (0.5%). Moreover, more than 60% of patients with stroke and TIA with low levels of AT, protein C and S also had concurrent acquired causes, such as anticoagulation, liver function derangement and infection. In addition, only a small proportion of those with low levels of AT, protein C and S were repeated, an important step in distinguishing genuine deficiency.
Compared with hereditary thrombophilia, antiphospholipid syndrome is a more established risk for arterial thrombosis.8 11–16 27–31 Patients with triple positivity for LA, ACL and anti-β2GPI have been shown to be at the highest risk for arterial and venous thrombosis, and for obstetric complications.32 However, only 3% of our thrombophilia-screened cohort had triple APA testing. There is evidence that persistent APA is associated with the highest incidence of thrombosis,33 although only 27% of our positive initial APA cohort was followed up by confirmatory APA testing.
AT, protein C and protein S deficiencies are rare in the general population, with an estimated frequency of about 1:5000.7 9 10 34–36 Similarly, FVL and PMG present in 5% and 1%–5.5% of the Caucasian population but are rare in other ethnic groups.34 37 38 Although those hereditary thrombophilias increase the risk of venous thrombosis, their association with arterial ischaemic stroke and TIA is less well established.5–16 More than 94% of patients with stroke and TIA in the thrombophilia-tested cohort had genotyping and protein C, S and AT tests, and similar to previous findings 13% of patients with ischaemic stroke and only 0.5% of patients with TIA were either carriers of FVL/PGM genotype or protein C-deficient, S-deficient or AT-deficient after exclusion of secondary causes of deficiency (table 2), indicating low-value hereditary thrombophilia screening especially in young TIA work-up. Consequently, based on the costing scheme outlined in online supplementary table 1, limited testing focusing on triple APS testing rather than full inherited thrombophilia panel only would potentially save £267.13 per patient. Those tested positive on initial testing for protein C, S or AT deficiency should be followed up by confirmatory testing. Low numbers of confirmatory testing may reflect the ‘hub and spoke’ model of hyperacute stroke care at regional centres in London, whereby initial positive testing at the regional centre may not have been effectively communicated to the stroke unit performing follow-up.
The standard thrombophilia panel could also be stratified by including multiple triple APA testing and excluding thrombophilia mutations screening. Based on our costs at the time of the study, this more focused testing would save £267.13 per patient.
Limitations of this study include its retrospective single-centre design. Attributable risks of thrombophilia screening and interaction between the other risk factors such as contraceptive pill use, migraine and smoking were not estimated. Statistical comparison between risk factors of thrombophilia-screened cohort and not-screened cohort was not assessed. However, our review is of real-life practice, highlighting that current thrombophilia testing should be particularised to patients with young stroke and TIA without conventional cardiovascular risk factors. Initial positive tests should be repeated to distinguish genuine thrombophilia from common false-positive conditions.
References
Footnotes
Contributors AC and AT designed the study. VA and AT collected the data. VA wrote the manuscript. MS, RS, AC and AT reviewed, edited and approved the final version of the manuscript. VA, AT and AC are guarantors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests VA received a European Stroke Organisation Young Investigator Award and was funded for the platform presentation.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available data can be obtained by contacting the corresponding author.