Article Text

Abstract
Objective Many patients receiving dual antiplatelet therapy still had recurrent strokes. We aimed to identify factors associated with recurrent stroke at 90 days in patients receiving dual antiplatelet therapy in Clopidogrel in High-risk patients with Acute Non-disabling Cerebrovascular Events trial.
Methods Patients with transient ischaemic attack or minor stroke receiving clopidogrel and aspirin in the trial were analysed in the study. The primary outcome was recurrent stroke within 90 days after the index event. Cox proportional hazard model with backward selection was used to identify factors associated with stroke.
Results Among 2584 patients, 212 (8.2%) had a recurrent stroke, 216 (8.4%) had a composite of stroke, myocardial infarction, or vascular death and 204 (7.9%) had ischaemic stroke within 90 days. Multivariate analysis identified the following factors associated with stroke: history of hypertension with poor blood pressure control (HR, 1.92; 95% CI 1.22 to 3.03), the high baseline National Institute of Health Stroke Scale (NIHSS) score of 2 and 3 (2.12 (1.07 to 4.21) and 4.11 (2.05 to 8.22), respectively), time from onset to randomisation of <12 hours (1.47 (1.12 to 1.94)), the lipid-lowering therapy (0.61 (0.47 to 0.83)), the open-label aspirin dose at day 1 of ≥300 mg (1.98 (1.45 to 2.69)). Intracranial arterial stenosis (ICAS) was significantly associated with stroke in the sensitivity analysis (2.17 (1.16 to 4.04)).
Conclusions The high baseline NIHSS score, hypertension with poor blood pressure control, ICAS, time from onset to randomisation of less than 12 hours and no lipid-lowering therapy were associated with stroke, suggesting that patients with identified predictors still remain to be at high risk of recurrent stroke although being under the dual antiplatelet therapy.
Trial registration number http://clinicaltrials.gov/show/NCT00979589. ClinicalTrials.gov number: NCT00979589
- Transient ischemic attack
- Acute ischemic minor stroke
- Dual antiplatelet therapy
- Recurrent stroke
- Risk factor.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Transient ischemic attack
- Acute ischemic minor stroke
- Dual antiplatelet therapy
- Recurrent stroke
- Risk factor.
Introduction
Transient ischaemic attack (TIA) or acute minor stroke is common and associated with 10%–20% risk of subsequent stroke in the first 90 days following index events.1–3 The Clopidogrel in High-risk patients with Acute Non-disabling Cerebrovascular Events (CHANCE) trial showed that the combination of clopidogrel and aspirin is superior to aspirin alone for reducing the risk of 90-day stroke and does not increase the risk of haemorrhage in patients with TIA or minor stroke.4 However, up to 8.2% of patients receiving dual antiplatelet therapy still experienced a recurrent stroke in the CHANCE trial.
Importantly, approximately 2%–5% of recurrent stroke occurred early within 24–48 hours after the index event,1 5–7 highlighting the need for rapid assessment and treatment of these high-risk patients. A study showed that the ABCD2 score might not have a good performance in triage for acute non-disabling stroke or TIA patients with hyperacute symptomatic carotid stenosis.8 Therefore, examining factors associated with recurrent stroke may help identify a target for secondary stroke prevention, especially among patients who have already received more aggressive antiplatelet therapy. Using data from the CHANCE trial, we performed a post doc analysis of patients with TIA or minor stroke who were randomised to aspirin and clopidogrel dual antiplatelet therapy to identify factors associated with recurrent stroke within 90 days.
Methods
Study design and population
Details about the CHANCE study design and results have been described before.4 9 Briefly, CHANCE was a multicentre, randomised, placebo-controlled, double-blind clinical trial conducted in China. The eligibility criteria were patients aged 40 years or older with a diagnosis of acute minor ischaemic stroke (National Institute of Health Stroke Scale10 (NIHSS) ≤3) or high-risk TIA (ABCD2 ≥4)6 and the ability to start the study drug within 24 hours after symptom onset. From October 2009 and July 2012, a total of 5170 patients within 24 hours after the onset of minor ischaemic stroke or high-risk TIA were randomly assigned to either clopidogrel plus aspirin (intervention) or placebo plus aspirin (control). Patients in the intervention arm (n=2584) received an open-label aspirin of 75 mg or more than at the discretion of the treating physician and a loading dose of 300 mg of clopidogrel shortly after the randomisation (day 1), followed by 75 mg clopidogrel per day from day 2 through 90 and 75 mg aspirin per day from day 2 through 21. Our current study focused on 2584 patients in the intervention arm (see online supplementary figure 1). The CHANCE protocol was approved by the ethics committee at each study centre. Written informed consent was obtained from all the participants or their legal proxies.
Data collection
Baseline evaluation included patient demographics, symptoms of the index event, vascular risk factors, blood pressure at baseline and at each visit of follow-up, the severity of minor stroke measured by NIHSS, imaging data, laboratory tests and concurrent medications including dose of open-label aspirin at day 1, antidiabetic and lipid-lowering therapy. Vascular risk factors included history of stroke or TIA, hypertension, diabetes, dyslipidaemia, myocardial infarction, angina or congestive heart failure, atrial fibrillation and current or previous smoking. Hypertension was defined as a systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, any use of antihypertensive drug or self-reported history of hypertension. Diabetes was defined as fasting glucose concentration ≥7.0 mmol/L, non-fasting glucose concentration ≥11.1 mmol/L with classic symptoms of hyperglycaemia or hyperglycaemic crisis, any use of glucose-lowering drugs or any self-reported history of diabetes. Dyslipidaemia was defined as serum total cholesterol ≥200 mg/d, serum triglyceride ≥150 mg/dL, low-density lipoprotein cholesterol ≥130 mg/dL, high-density lipoprotein cholesterol ≤40 mg/dL, any use of lipid-lowering drugs or any self-reported history of dyslipidaemia. Presence of intracranial arterial stenosis (ICAS) was defined as 50%–99% stenosis or occlusion of at least one of the following arterial segments on MR angiography: intracranial portion of internal carotid arteries, middle cerebral arteries (M1/M2), intracranial portion of vertebral arteries and basilar artery.11 12
Outcome measures
The primary outcome was recurrent stroke (ischaemic or haemorrhagic) within 90 days after randomisation. Secondary outcomes included ischaemic stroke, and composite of stroke, myocardial infarction (MI) or vascular death within 90 days. The 90-day follow-up was done by face-to-face interview. Patients were evaluated by certified investigators who were blinded to patients’ baseline clinical status and treatment allocation. Imaging data in patients with events of interest were collected so as to ensure the accuracy of endpoint judgement by investigators. All reported endpoint events were verified by a central adjudication committee blinded to the assignments of study groups through a full review of the clinical and imaging information.
Statistical methods
Baseline demographic and clinical characteristics were compared between patients with and without 90-day stroke. Continuous variables were expressed as mean with SD or median with IQR, while categorical data were presented as proportions.
Cox proportional hazard model with backward selection was used to identify factors associated with outcomes of interest. The following candidate factors were included in the multivariable analysis: demographic features, vascular risk factors, severity of index events, time from symptom onset to randomisation (<12 or ≥12 hours), open-label aspirin dose at day 1, body mass index (BMI), blood pressure control within 90 days, antidiabetic or lipid-lowering therapy and laboratory parameters. The blood pressure was measured by the study coordinator at each visit of day 21 and day 90 after randomisation. If patients had a systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg at day 21 or day 90, high blood pressure would be determined. We categorised the blood pressure control status within 90 days into the following four groups according to history of hypertension and the blood pressure level during follow-up: (1) no hypertension and normal blood pressure within 90 days, (2) no hypertension and high blood pressure within 90 days, (3) hypertension and normal blood pressure within 90 days and (4) hypertension and high blood pressure within 90 days. The open-label aspirin dose at day 1 was not a continuous variable and grouped into three categories based on the commonly used doses of 100 mg (42.5%) and 300 mg (22.3%) as a cutting point:≤100 mg, 100–300 mg, and ≥300 mg. Patients were divided into three groups based on history of diabetes and status of antidiabetic therapy: no diabetes, diabetes without therapy and diabetes with therapy. NIHSS of 0, 1, 2 or three for severity of index events was analysed as the categorical variable. Considering TIA or the minor stroke being under an overarching umbrella of non-disabling ischaemic cerebrovascular events, TIA with the unilateral weakness was scored as NIHSS of 2, TIA with the speech impairment without weakness scored as NIHSS of 1 and TIA with other symptoms scored as NIHSS of 0. HR with 95% CI were reported for effect of identified factors on outcomes.
The variable of ICAS was not incorporated into the aforementioned multivariable model among the whole study population because only 531 patients were available for the imaging data. Given importance of ICAS for predicting stroke risk in ABCD2–MRI scoring systems, we made a sensitivity analysis, that is, cox proportional hazard model was used to identify factors for stroke outcomes among patients who had the imaging data.
Additionally, we generated Kaplan-Meier plot for each of independent factors to investigate whether or not the risk of a new stroke occurrence varied with time according to levels of the factor. Patients without any events during 90-day follow-up were censored at the time of study termination or death. Two-tailed p values of less than 0.05 were considered to be statistically significant. All analyses were conducted using SAS V.9.3 software.
Results
Study patients and characteristics
Of 2584 patients receiving dual antiplatelet therapy, 717 (27.7%) were TIA and 1867 (72.3%) were minor ischaemic stroke. Mean age was 63.9 years and 852 (33.0%) were female, and 1997 (77.3%) patients had high blood pressure measured at day 1 of the patient recruitment. Risk factors of stroke such as previous TIA or stroke, hypertension and diabetes were common in the study. Of 531 patients with imaging data, 231 (43.5%) had the intracranial arterial stenosis (table 1).
Demographic and clinical characteristics in CHANCE clopidogrel–aspirin patients with and without stroke within 90 days after index events
Stroke occurred in 212 (8.2%) patients within 90 days after randomisation (see online supplementary figure S1). Patients with recurrent stroke were more likely to have a medical history of hypertension and smoking, higher BMI and NIHSS score, to be randomised within <12 hours of symptom onset, to receive higher dose of aspirin at day 1 (≥300 mg), to have poor blood control during follow-up and higher proportion of ICAS, as compared with those without stroke. Additionally, they were also less likely to receive the lipid-lowering therapy as compared with patients without subsequent stroke (34.4% vs 43.5%, p=0.01) (table 1).
Factors associated with the primary outcome of stroke
Multivariable Cox proportional hazard model identified the following factors to be independently associated with the 90-day stroke events: history of hypertension with poor blood pressure control within 90 days as compared with the reference of no hypertension with the normal blood pressure (HR, 1.92; 95% CI 1.22 to 3.03; p=0.005), but the other two groups were not significantly different from the reference group; baseline NIHSS score of 2 and 3 as compared with the reference: 2.12 (1.07–4.21) and 4.11 (2.05–8.22), respectively, while the NIHSS scores of 1 was not found significant. Time from onset to randomisation of <12 hours (HR, 1.47; 95% CI 1.12 to 1.94; p=0.006); Lipid-lowering therapy (HR, 0.61; 95% CI 0.47 to 0.83; p=0.001); Open-label aspirin dose at day 1 of ≥300 mg as compared with the reference group of ≤100 mg (HR, 1.98; 95% CI 1.45 to 2.69; p<0.001) (table 2). Among 531 patients with imaging data, a multivariable analysis found that ICAS was significantly associated with stroke (HR, 2.17; 95% CI 1.16 to 4.04; p=0.01).
Effects of prognostic factors on 90-day outcomes in patients with clopidogrel plus aspirin treatment in multivariable analysis*
Incidences of stroke and Kaplan-Meier plots according to levels of identified factors
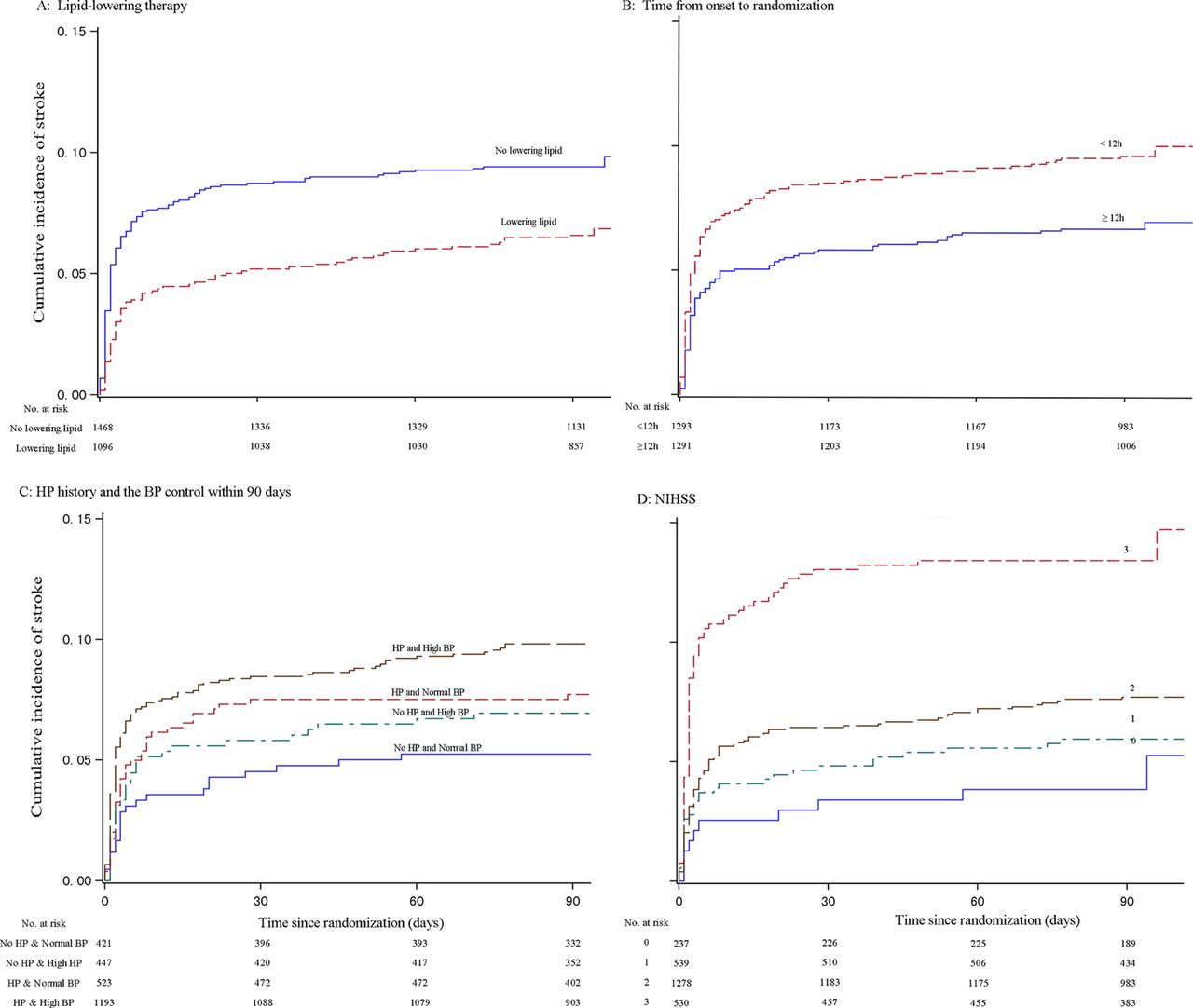
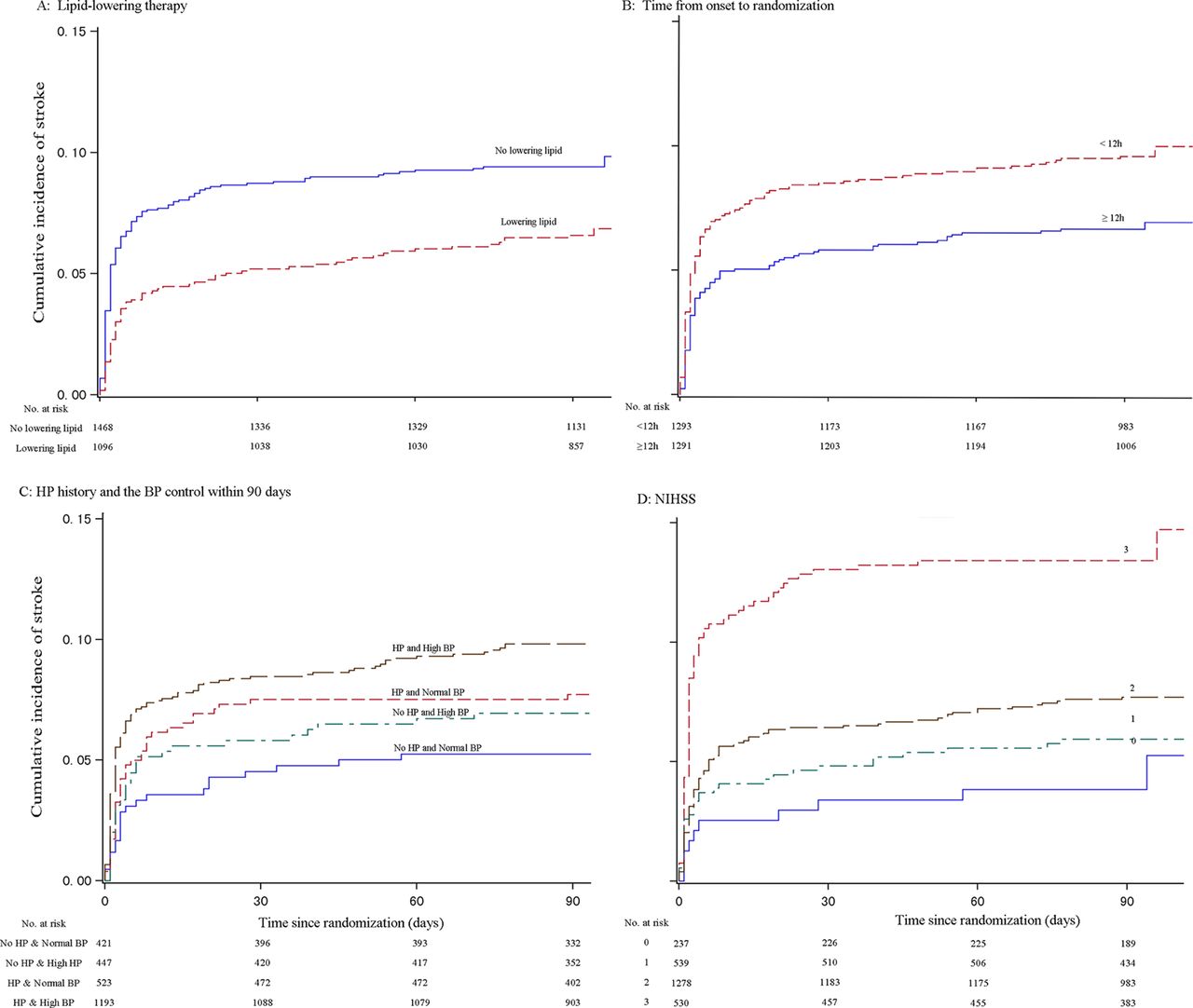
The incidences with 95% CI of stroke within 90 days after randomisation in patients according to levels of identified factors as follows: 5.2% (3.1%to 7.4%) for no hypertension with normal blood pressure within 90 days, 7.2% (4.8%to 9.6%) for no hypertension with high blood pressure within 90 days, 7.7% (5.4%to 9.9%) for hypertension with normal blood pressure within 90 days, 9.9% (8.2%to 11.6%) for hypertension with high blood pressure; 4.2% (1.7%to 6.8%) for NIHSS of 0, 5.9% (3.9%to 3.9%) for NIHSS of 1, 7.7% (6.2%to 9.1%) for NIHSS of 2 and 13.6% (10.7%to 16.5%) for NIHSS of 3; 9.7% (8.1%to 11.3%)) for randomisation time of <12 hours and 6.7% (5.4%to 8.1%) for randomization time of ≥12 hours; 9.5% (8.0%to 11.0%) for no lipid-lowering therapy and 6.7% (5.2%to 8.1%) for lipid-lowering therapy; 7.1% (5.8%to 8.4%) for the open-label aspirin dose of ≤100 mg, 7.0% (4.8%to 9.2%) for 100to 300 mg and 12.1% (9.4%to 14.8%) for ≥300 mg. Among 531 patients with imaging data stratified by ICAS, incidence of 90-day stroke was 5.3% (2.8%to 7.9%) for no ICAS, while 11.3% (7.2%to 15.3%) for ICAS. Figure 1 showed the accumulative incidence of stroke within 90 days versus time from randomisation based on levels of factors identified in the multivariable analysis.
![[SP1.jpg]](https://svn.bmj.com/content/svnbmj/2/4/176/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
Cumulative incidence of 90-day stroke versus time from randomisation in Clopidogrel in High-risk patients with Acute Non-disabling Cerebrovascular Events clopidogrel–aspirin group according to prognostic factors. Panel (A) is for patients stratified by the lipid-lowering therapy, panel (B) by time from onset to randomisation, panel (C) by history of hypertension and the blood pressure control status within 90 days and panel (D) by NIHSS. BP, blood pressure; HP, hypertension; NIHSS, National Institute of Health Stroke Scale.
Factors associated with secondary outcomes
Of 2584 patients receiving dual antiplatelet therapy, 216 (8.4%) had a composite of stroke, MI or vascular death within 90 days. Among these, 204 (7.9%) patients had an ischaemic stroke. Table 2 shows factors associated with secondary outcomes. Similar to the primary outcome predictors, patients receiving the open-label aspirin dose of ≥300 mg at day 1 and not lipid-lowering therapy and those with a medical history of hypertension with poor blood pressure control within 90 days, baseline NIHSS score of 2 and 3 as compared with the reference group of NIHSS score of 0 and time from onset to randomisation of <12 hours were associated with recurrent ischaemic stroke or a composite of a composite of stroke, MI or vascular death within 90 days. Among patients with imaging data, the sensitivity analysis showed that ICAS was also associated with these secondary outcomes: 2.17 (1.16–4.04) for the ischaemic stroke and the composite endpoint.
Discussion
The further analysis of CHANCE trial showed that the following factors were associated with risk of stroke within 90 days after randomisation in patients with high-risk TIA or minor stroke under the therapy of clopidogrel and aspirin: hypertension with poor blood pressure control, high baseline NIHSS score, time from onset to randomisation of less than 12 hours, no lipid-lowering therapy and the open-label aspirin dose of 300 mg or more than at day 1. The sensitivity analysis showed that ICAS was also identified as the risk factor of the 90-day stroke. We observed that the incidence of stroke within 90 days after randomisation was approximately 9%–14% in patients with mentioned-above conditions, and especially high for baseline NIHSS score of 3. Furthermore, the factors for secondary outcomes were the same as those for the primary outcome of stroke.
The multivariable analysis identified the high baseline NIHSS score as one of the independent predictors for 90-day vascular events in patients with high-risk TIA or minor stroke, in which NIHSS scores of 2 and 3 were statistically significant but not NIHSS scores of 1 as compared with NIHSS score of 0 as the reference. Remarkably, the incidence of 90-day stroke in patients with NIHSS of 3 still remains very high although the combination of clopidogrel and aspirin was administered to them. The curve for the accumulative incidence of stroke (panel D of figure 1) further showed that the incidence dramatically increased to more than 10% of stroke at the first few days and thereafter had a gentle upslope until to approximate 30 days after randomisation. This indicates that the other therapy strategy at the first few days of symptom onset might be explored for TIA or minor stroke patients with the high baseline NIHSS score of 2 or 3. Additionally, the duration of dual antiplatelet treatment might be expanded from 21 days to 30 days.
In the present analysis, we found that hypertension with poor blood pressure control is associated with risk of 90-day cardiovascular events or stroke as compared with no hypertension with normal blood pressure among minor stroke or TIA patients with dual antiplatelet therapy of clopidogrel and aspirin. Importantly, there is no significant difference in HR of stroke between patients with hypertension but with good BP control and patients with no hypertension. The sensitivity analysis of the study also demonstrated that ICAS, as an atherosclerotic-marker component of ABCD2-MRI, would contribute twofold risk of subsequent stroke, MI and cardiovascular death in patients with TIA or a minor stroke. Furthermore, the study showed that the lipid-lowering therapy was identified to be associated with approximately 35%–40% reduction of the 90-day vascular event risk in non-disabling ischaemic cerebrovascular disease. So, control of blood pressure in patients with hypertension and lipid-lowering therapy in patients with a condition of an atherosclerotic origin are the key interventions in the secondary prevention of minor ischaemic or TIA.
Previous studies demonstrated that about 50% of early recurrent strokes occurred within 24–48 hours of TIA or minor stroke.1 6 The current study showed that time from onset to randomisation of less than12 hours was independently associated with the primary or secondary outcomes within 90 days after randomisation, indicating that the high-risk period of stroke occurrence might be narrowed to within 12 hours after high-risk TIA or minor stroke. There was still approximately 10% incidence of 90-day stroke although patients were admitted to hospital and given dual antiplatelet therapy within 12 hours of TIA or minor stroke, which suggests that the dual antiplatelet therapy in the CHANCE trial might be not enough to prevent the early occurrence of stroke. Thus, it might be a beneficial strategy that patients with high-risk TIA or minor stroke would be assessed as early as within 12 hours of events and more intensive antiplatelet regimen than that of the CHANCE trial would be initiated. However, the addition of a third antiplatelet drug did nothing to prevent strokes but it did increase bleeding risks in the Triple Antiplatelets for Reducing Dependency in Ischaemic Stroke trial.13
The guideline for the early management of patients with acute ischaemic stroke suggested that oral administration of aspirin (initial dose is 325 mg) within 24 to 48 hours after stroke onset is recommended for treatment of most patients to produce additional benefits (class I; level of evidence A).14 However, our study found that the open-label aspirin dosage of 300 mg or more than at day 1 was associated with high risk of primary or secondary endpoints compared with the dosage of 100 mg or less. There was no significant difference in haemorrhagic strokes between two groups (see online supplementary table S1). The study seems to reveal a paradox phenomenon that an increased thrombocyte inhibition leads to more ischaemic strokes. The further analysis of the current study showed that the qualifying event of minor ischaemic stroke versus TIA or the high blood pressure at randomisation was associated with the high dose of the open-label aspirin prescribed by the treating physician (see online supplementary table S2). There would be a possibility of unmeasured confounding factors, for example, a more complex clinical presentation or complex imaging prior to randomisation, which would lead to a higher dose of the initial aspirin. Thus, we cautioned against overstatement of these results which are based on post hoc analysis.
The strength of the study was that the data were drawn from the large-scale, well-performed, randomised controlled trial which ensured integrity and reliability of measured data. We added components of ABCD215 and ABCD3-I16 to the multivariable model, especially the clinical feature of hemiparesis or dysphasia for TIA and the imaging data of ICAS. Moreover, treatment information such as blood pressure control during the follow-up and lipid-lowering therapy was also included into the analysis, but the study also had some limitations. First, there might be some residually unmeasured or unknown factors which might confound the association of identified predictors with stroke. Second, age and diabetes established and validated in risk models of ABCD2 were not identified as risk factors for stroke in the study, which might be attributable to not large sample size leading to random low in the study population selection. Lastly, data of genetics and diffusion-weighted imaging patterns of signal abnormality were not incorporated into the analysis because they were unavailable for most study participants.
In summary, we identified the high-baseline NIHSS score, hypertension with poor blood pressure control, intracranial arterial stenosis, time from onset to randomisation of less than 12 hours and no lipid-lowering therapy to be independently associated with increased risk of 90-day stroke in patients with high-risk TIA or minor ischaemic stroke under the therapy of clopidogrel and aspirin. We should bear in mind that patients with one of identified risk factors still have a high incidence of 90-day stroke, suggesting that it would be not ignorable to explore the optimal and appropriate therapy strategy for high-risk patients with minor ischaemic stroke or TIA in the future.
Acknowledgments
We thank all participating investigators. A full list of the CHANCE investigators is available at: http://www.nejm.org/doi/suppl/10.1056/NEJMoa1215340/suppl_file/nejmoa1215340_appendix.pdf
References
Footnotes
RW and XW contributed equally.
Contributors YJW, YLW, XQZ contributed to conception and design of the study. RQW and XWW drafted the manuscript or tables or figures. YJW, YLW and YX contributed to comments on the draft manuscript and revised the report. Site investigators contributed to data acquisition not analysis. YLW and LPL coordinated the study. XM and XWW oversaw the subject recruitment and monitored gathering clinical data. HL conducted the statistical analysis.
Funding The study was supported by grants from the Ministry of Science and Technology of the People’s Republic of China and Program for New Century Excellent Talents in University. The grant numbers are 2008ZX09312-008, 2011BAI08B02, 2012ZX09303, 200902004 and NCET-13–0917.
Competing interests None declared.