Article Text

Abstract
With modern intensive medical therapy, the annual risk of ipsilateral stroke in patients with asymptomatic carotid stenosis (ACS) is now down to ∼0.5%. Despite this, there is a widespread practice of routine intervention in ACS with carotid endarterectomy (CEA) and stenting (CAS). This is being justified on the basis of much higher risks with medical therapy in trials conducted decades ago, compared with lower risks of intervention in recent trials with no medical arm. Such extrapolations are invalid. Although recent trials have shown that after subtracting periprocedural risks the outcomes with CEA and CAS are now comparable to medical therapy, the periprocedural risks still far outweigh the risks with medical therapy. In the asymptomatic carotid trial (ACT) 1 trial, the 30-day risk of stroke or death was 2.9% with CAS and 1.7% with CEA. In the CREST trial, the 30-day risk of stroke or death among asymptomatic patients was 2.5% for stenting and 1.4% for endarterectomy. Thus, intensive medical therapy is much safer than either CAS or CEA. The only patients with ACS who should receive intervention are those who can be identified as being at high risk. The best validated method is transcranial Doppler embolus detection. Other approaches in development for identifying vulnerable plaques include intraplaque haemorrhage on MRI, ulceration and plaque lucency on ultrasound, and plaque inflammation on positron emission tomography/CT. Intensive medical therapy for ACS includes smoking cessation, a Mediterranean diet, effective blood pressure control, antiplatelet therapy, intensive lipid-lowering therapy and treatment with B vitamins (with methylcobalamin instead of cyanocobalamin), particularly in patients with metabolic B12 deficiency. A new strategy called ‘treating arteries instead of risk factors’, based on measurement of carotid plaque volume, is promising but requires validation in randomised trials.
- carotid stenosis
- Endarterectomy
- Stenting
- Transcranial Doppler
- Medical therapy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Patients with asymptomatic carotid stenosis (ACS) have severe atherosclerosis and, besides a moderate risk of stroke, are at high risk of myocardial infarction. Although screening for asymptomatic stenosis is not justified for the purpose of identifying patients for inappropriate intervention, ultrasound assessments of atherosclerosis severity may be useful in identifying patients at high risk, in whom intensive medical therapy would markedly reduce risk.1 Indeed, the risk of myocardial infarction in ACS is higher than the risk of stroke. It is thus immaterial that randomised controlled trials have not been carried out to test the efficacy of interventions such as antiplatelet therapy. In the Veteran's Administration trial of ACS,2 patients with no prior history of coronary disease had a 33% 4-year risk of myocardial infarction. Among patients with diabetes, intracranial stenosis and peripheral vascular disease, the 4-year risk of a coronary event was 69%. It is axiomatic, therefore, that all patients with ACS should receive intensive medical therapy. However, despite widespread belief that carotid endarterectomy (CEA) and stenting (CAS) are justified in ACS, most patients (∼90%) with ACS would be better treated with intensive medical therapy than with either stenting or endarterectomy. In this narrative review, we will summarise the evidence for that statement, and describe optimal medical management for patients with ACS.
Intensive medical therapy
Lifestyle
Intensive medical therapy (best medical therapy) for ACS has recently been reviewed.3 The effect of a healthy lifestyle is much greater than most physicians suppose. Among women in the US Health Professionals Study and Nurses' Health Study, adopting all five healthy lifestyle choices (not smoking, moderate alcohol intake, a body mass index <25, 30 min of daily exercise and a healthy diet score in the top 40%) reduced the risk of stroke by 80%.3 Unhealthy lifestyle choices accounted for half of stroke. The US lifestyle is so unhealthy4 that this might not be very surprising. However, in Sweden, where the population may be healthier, healthy lifestyles reduced the risk of stroke by 60% among women,5 and the risk of myocardial infarction by 80% among men with hypertension and hyperlipidaemia.6
Smoking cessation
Smoking increases the risk of stroke approximately sixfold, and even secondhand smoke nearly doubles cardiovascular risk.7 It is likely that smoking cessation is the single most important measure for stroke prevention. Physicians should therefore not simply accept that patients will not quit smoking; it is vital to persuade patients to quit. Governments should also be implementing measures to reduce smoking. An important measure in smoking cessation is the use of adequate nicotine replacement. Smoking is very hard to quit, because it is not due to just a powerful addiction to nicotine; it is also a habit, a social activity, a crutch and for some patients even an identity. It is important to advise the patient to use enough nicotine replacement to deal with the addiction, while becoming accustomed to becoming a non-smoker. In severe addicts (who may get up at night to smoke), this may require two nicotine patches, plus a nicotine inhaler when cravings strike. Medications such as bupropion and varenicline may also be helpful. A good review of strategies for smoking cessation is a chapter by Pipe.8
Smoking is a particular problem among Chinese men. In a 2010 survey, 68% of men over age 15 smoked, compared with 3% of women; smoking was more prevalent in rural than urban sites.9
Diet
The diet for which the best evidence exists for vascular prevention is the Cretan Mediterranean diet. This is a mainly vegetarian diet10 that is high in olive oil, canola oil, fruits, vegetables, lentils, beans, chickpeas, nuts and whole grains. It is possible that a vegan diet may be even better for cardiovascular prevention, but this has not been tested. Furthermore, for many patients, a vegan diet may not be achievable. In an important Israeli study, the Cretan Mediterranean diet was compared with a low-fat diet and a low-carbohydrate diet. Among diabetic participants, the Mediterranean diet was clearly the most efficacious at reducing fasting blood sugar, fasting insulin levels and insulin resistance.11 In secondary prevention, this diet reduced stroke and recurrent myocardial infarction by more than 60%.12 In primary prevention, this diet reduced stroke by nearly 50%.13
Although in the past the diet in China was largely protective against atherosclerosis, with increasing prosperity there has been increased intake of fat and cholesterol, and a corresponding major increase in atherosclerosis. Between 1980 and 2013, coronary artery disease increased by 9.5% per year.9 Whereas in the past stroke was more common than myocardial infarction, the latter became more common than the former in 2010.
Blood pressure control
Effective blood pressure control requires attention to patient compliance, substances that patients consume that may aggravate hypertension, and identifying the underlying cause of the hypertension.
Approximately half of the patients will admit that they are not taking their medication; follow-up with the patient's pharmacy can determine if the patient has refilled prescriptions in a timely manner. Substances that patients consume that may impair blood pressure control include salt, licorice, alcohol, decongestant, birth control medications and non-steroidal anti-inflammatory agents (NSAIDS). The only NSAID that does not raise blood pressure is sulindac.14 Salt restriction to 2–3 g/day of salt (∼780–1200 mg of sodium) and a Mediterranean diet similar to the Dietary Approaches to Stop Hypertension (DASH–Salt) diet15 and moderation of alcohol intake may be important measures in resistant hypertension. Sodium restriction may be particularly important in China.16 ,17 A high intake of sodium and high prevalence of hypertension go hand in hand, and are particularly prevalent in the central provinces.18
An important problem in blood pressure control is the common assumption that all patients are the same. They are not. When a patient has uncontrolled hypertension despite two or more classes of drugs, it is important to identify the underlying cause of the hypertension. Once rare causes of hypertension have been excluded (such as pheochromocytoma, aortic coarctation, licorice and renal tumours), an efficient approach is to measure plasma renin and aldosterone.
Table 1 shows an algorithm for identifying the appropriate treatment for patients with resistant hypertension.19 If plasma renin is low and plasma aldosterone is high, the problem is primary aldosteronism, and the best treatment is an aldosterone antagonist (spironolactone for women, or eplerenone for men). If plasma renin is high and aldosterone is high (secondary hyperaldosteronism), the primary treatment would be an inhibitor of angiotensin II (ARB). If the renin and aldosterone levels are both low (a Liddle syndrome phenotype), the primary treatment would be amiloride. Primary aldosteronism accounts for ∼20% of resistant hypertension; variants of Liddle's syndrome account for ∼6% of resistant hypertension, and are important because there is a specific therapy—amiloride.
Physiologically individualised therapy* based on renin/aldosterone profile
Antiplatelet therapy
There is unwarranted controversy regarding absence of evidence that antiplatelet agents reduce stroke in ACS. Since patients with ACS are at high risk of myocardial infarction, they should all receive antiplatelet agents. Although dual antiplatelet agents have not been validated in randomised controlled trials in ACS, there are reasons to think they may be beneficial. On the basis of several issues, dual antiplatelet therapy with aspirin and clopidogrel or other P2Y12 antiplatelet agents may be more effective than either alone.20 That approach was more effective in secondary stroke prevention,21 in coronary disease, in prevention of microemboli in carotid stenosis and intracranial stenosis, and was used in the SAMPPRIS trial22 of intracranial stenosis.
Several pharmacokinetic issues are important in antiplatelet therapy. Although true aspirin resistance may exist, enteric coating may account for much of aspirin ‘pseudoresistance’;23 probably uncoated low-dose aspirin should be used. Higher doses are less effective,24 probably because maximal inhibition of platelet thromboxane is achieved with low-dose aspirin, and higher doses have more prolonged inhibition of endothelial prostacycline.
Both clopidogrel and prasugrel are prodrugs that require metabolism to the active form, and polymorphisms of cytochrome P450 (CYP) subtypes that result in poor metabolism to the active form are not uncommon. Polymorphisms of CYP2C19 may be particularly important in China,25 ,26 where they are more frequent than in other populations. Importantly, this is not an issue for ticagrelor.27
Lipid-lowering drugs
Although evidence for lipid-lowering drugs may also be lacking with regard to asymptomatic stenosis, all patients with asymptomatic stenosis should receive them, if only because of their high risk of coronary disease. Diet is not a substitute for lipid-lowering drugs, because the effects of diet are mainly postprandial,28 whereas effects of drugs are mainly on fasting lipids. Both diet and lipid-lowering drugs are needed. As discussed below, intensive medical therapy that includes lipid-lowering therapy markedly reduced cardiovascular risk in patients with ACS.
Statin drugs reduce the formation of cholesterol by blocking the rate-limiting step in cholesterol synthesis (hydroxymethylglutarate coenzyme A reductase). However, in the pathway for synthesis of cholesterol (figure 1), levels of many intermediate metabolites are also reduced. One of these is converted to ubiquinone (coenzyme Q10, CoQ10). It is likely that most of the true causal adverse effects of statins (myopathy and a slight increase in the risk of diabetes) are due to impaired mitochondrial function resulting from depletion of CoQ10.30 High doses of CoQ10 may be beneficial, but the evidence for that is weak. Many putative adverse effects of statins are probably not valid, including hepatotoxicity, intracerebral haemorrhage, nephrotoxicity and cognitive impairment.30
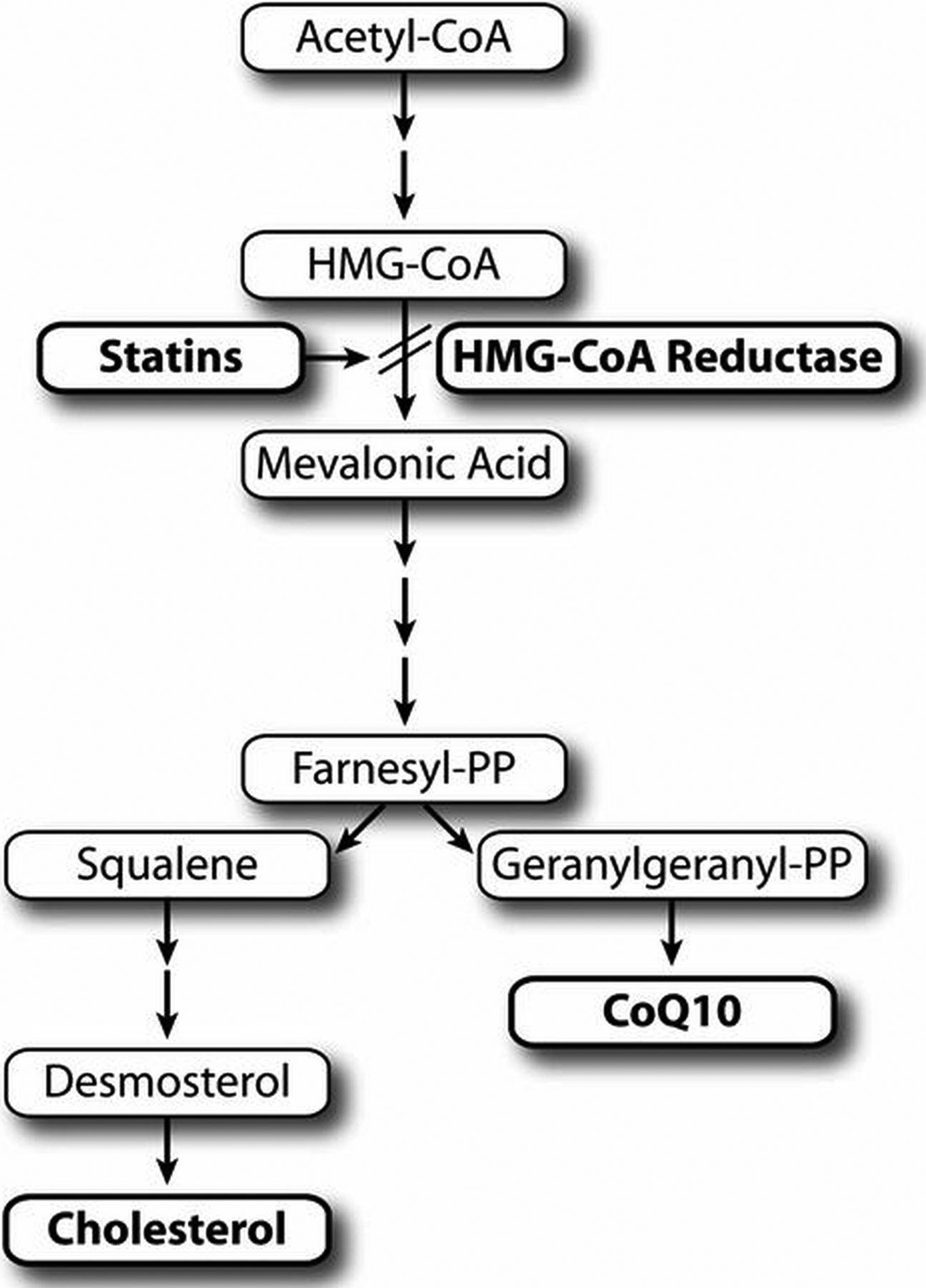
Effects of statins (hydroxymethylglutarate (HMG) coenzyme A reductase inhibitors) on synthesis of ubiquinone (coenzyme Q10, CoQ10). Between the inhibition of HMG coenzyme A reductase and cholesterol are many intermediate metabolites. By the same action that lowers levels of low-density lipoprotein cholesterol, statins also lower levels of CoQ10; this may lead to mitochondrial dysfunction contributing to myopathy and insulin resistance/diabetes (reproduced by permission of Vanderbilt University Press from: Spence).29
A number of genetic factors predispose patients to adverse effects of statins; these have recently been reviewed.30 Some of these may be more common in Asian patients, who may require lower doses of statins. In patients who cannot take high doses of statins, and in patients with severe atherosclerosis, it is useful to add ezetimibe. Ezetimibe specifically blocks absorption of cholesterol (both dietary cholesterol and cholesterol recycled in bile salts), and is synergistic with statins: daily doses of 10 mg of atorvastatin with 10 mg of ezetimibe lower low-density lipoprotein (LDL) cholesterol to nearly the same extent as 80 mg of atorvastatin. Approaches to minimising adverse effects of statins were recently reviewed.30
B vitamin therapy
In recent years, there has been unwarranted pessimism about prevention of stroke with B vitamin therapy. The negative results of the VISP and NORVIT trials, and misinterpretation of the HOPE 2 trial, led many to think that B vitamin therapy does not prevent stroke. However, the HOPE 2 trial actually showed a statistically significant 23% reduction of stroke, as did the French SuFolOM3 trial, and there was also significant stroke reduction with B vitamins in a subgroup of the VITATOPS trial not receiving antiplatelet therapy.
The reasons that the VISP trial was null included initiation of folate fortification in North America at the time the trial was begun (thus negating the benefit of folic acid), treatment with injections of vitamin B12 in participants with low serum B12 level in both arms of the study (thus negating the benefit of B12 in the very participants who would have benefited most), and, as it turns out, the harm of cyanocobalamin among participants with impaired renal function. A subgroup analysis of VISP from which participants in the lowest 10% of estimated glomerular filtration rate (eGFR; 48), and those who received B12 injections, showed a clear benefit of high-dose B vitamins over low-dose vitamins: among participants receiving high-dose vitamins and who had a baseline serum B12 above the median (313 pmol/L), there was a 34% reduction in stroke/death/myocardial infarction, compared with participants who had a serum B12 below the median (implying poor absorption of B12) and received low-dose vitamins. Then everything became clear with the publication of the DIVINe trial in patients with diabetic nephropathy. High-dose B vitamins (including cyanocobalamin 1000 µg) were actually harmful, accelerating the decline of GFR, and doubling cardiovascular events. Loscalzo had hypothesised in an editorial accompanying the NORVIT and HOPE 2 trials that toxicity from unmetabolised folate may have accounted for the null results. Then Spence and colleagues hypothesised in 2011 that it was harm from the cyanide in cyanocobalamin among participants with low eGFR that may have accounted for the null result in VISP (some of which probably also apply to the NORVIT trial, with a similar older, sicker study population). Reasons for the harm of cyanide and thiocyanate from cyanocobalamin have recently been reviewed.31
The key missing piece of the puzzle has now been found, with the publication of the China Stroke Primary Prevention Trial,32 showing that in China, where folate fortification has not been implemented, folic acid significantly reduced the risk of stroke. Importantly, results that are not as yet published show that among participants with an eGFR below 60, folic acid slowed the decline of eGFR and significantly reduced events. This substantiates the hypothesis that it was the cyanide in cyanocobalamin that was harmful in the VISP and DIVINe trials. We should be using methylcobalamin instead of cyanocobalamin.31
This strategy is particularly important in patients with metabolic B12 deficiency, which is much more common than most physicians would suppose. A serum B12 in the ‘normal’ range is not sufficient to establish metabolic adequacy of functional B12; to do so, it is necessary to measure holotranscobalamin, or one of the metabolic products resulting from metabolic B12 deficiency:31 methylmalonic acid (MMA) is specific and total homocysteine (tHcy) is a surrogate for MMA in folate-replete participants (however, impaired renal function also elevates tHcy).
Treating arteries instead of treating risk factors
In 2002, our group reported33 that carotid plaque burden measured by ultrasound was a strong predictor of the 5-year risk of stroke, death or myocardial infarction: after adjustment for age, sex, blood pressure, smoking, serum cholesterol, tHcy, diabetes and treatment of blood pressure or cholesterol, patients in the top quartile of total plaque area had a 3.4-fold higher risk of those events, compared with those in the lowest quartile. Risk was graded; approximately 5%, 10%, 15% and 20% 5-year risk of events, by quartile of plaque area. That finding was subsequently validated in the Tromsø study in Norway.34 ,35 In our 2002 report, we also observed that during the first year of follow-up, half the patients had plaque progression, a quarter had plaque regression and a quarter were stable. Patients with plaque progression despite treatment according to guidelines had twice the risk of events compared with those with stable plaque or regression. This meant that treatment according to guidelines was failing half of our patients. This led us to develop an approach that we call ‘treating arteries instead of treating risk factors’. By this, we mean that the objective of therapy is not simply to achieve a blood pressure below 130/80 and an LDL cholesterol below 1.8 mmol/L; it is to stop plaque progression or achieve regression.
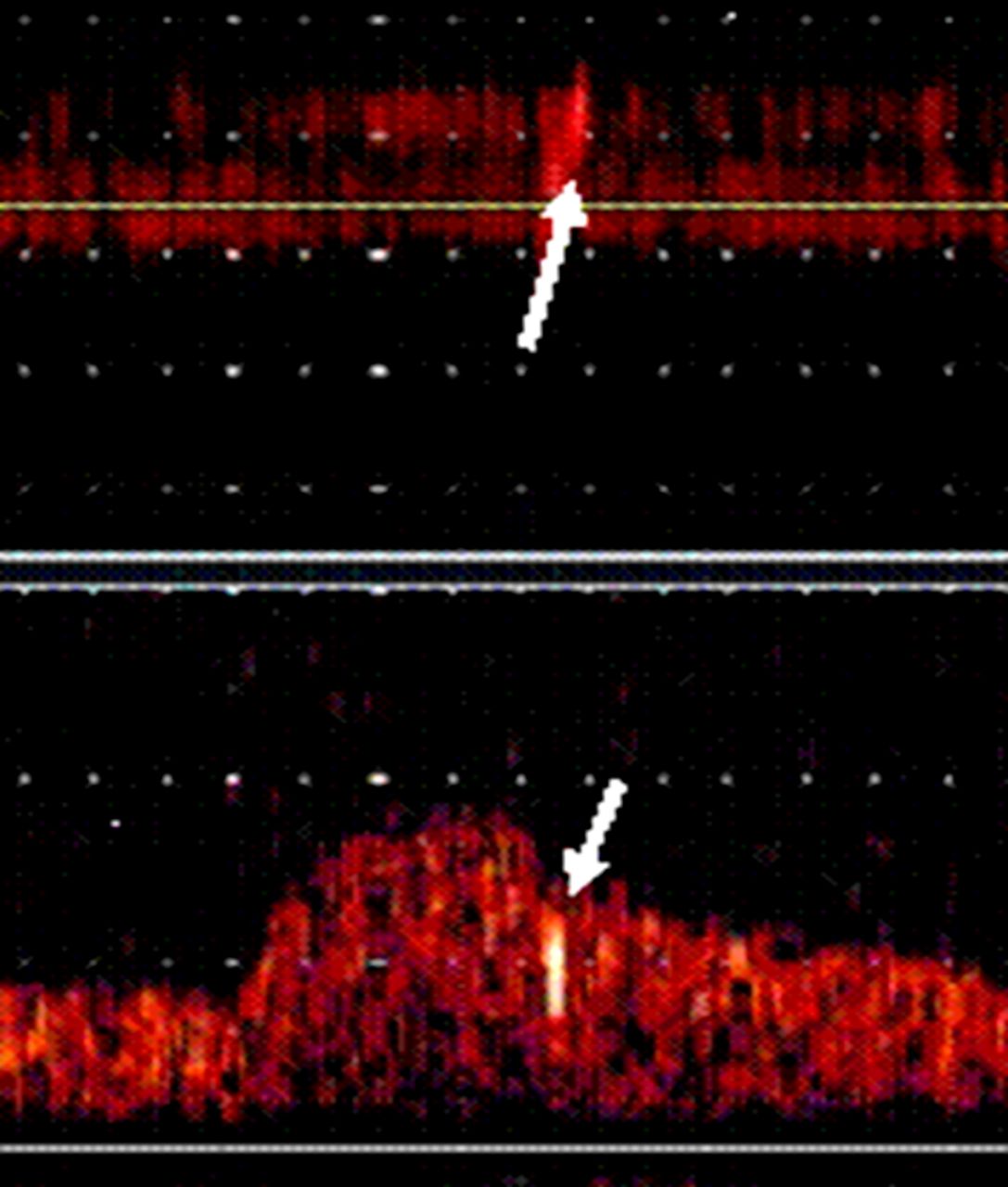
In 2010, we reported that this approach had reversed the proportion of patients with plaque progression; we were now observing regression of plaque in approximately half the patients and progression in only approximately a quarter. What that accomplished in patients with asymptomatic stenosis was dramatic. We had observed in 200536 that patients with asymptomatic stenosis with microemboli on transcranial Doppler (TCD; figure 2) had a 15% 1-year risk of stroke, compared with only a 1% risk among patients without microemboli. In 2010, we reported that more intensive medical therapy based on ‘treating arteries’, implemented in our clinic in 2003, had reduced the proportion of patients with microemboli from 12.6% to 3.7% (probably by stabilising plaques). The rate of plaque progression declined significantly and, more importantly, cardiovascular events declined markedly: the 2-year risk of stroke dropped from 8.8% to 1%, and the 2-year risk of myocardial infarction dropped from 7.6% to 1%.37 Much of that benefit was probably due to ezetimibe, which became available on the market in 2003.38 Efforts are now under way to mount a randomised trial of usual care versus ‘treating arteries’ in China, using three-dimensional (3D) measurement of carotid plaque volume. That approach is much more sensitive to effects of therapy than measurement of carotid intima-media thickness or coronary plaque by intravascular ultrasound.39

Detection of microemboli by transcranial Doppler identifies high-risk asymptomatic carotid stenosis. The white arrow in the upper channel shows the M-mode image of a microembolus in the middle cerebral artery ipsilateral to an asymptomatic carotid stenosis; the high-intensity transit signal is seen (white arrow) in the Doppler channel below (reproduced by permission of Wolters Kluver from: Spence JD et al).36
Risk of stenting and endarterectomy in ACS
The widespread practice of routinely intervening in asymptomatic stenosis with CEA or CAS is justified by comparisons of modern risks of intervention with historical risks in the medical arm of randomised trials conducted decades ago. Such extrapolations across studies and eras are not legitimate. Routine intervention for asymptomatic stenosis varies widely: from 90% of carotid procedures in the USA, to ∼60% in Italy and Germany, to ∼15% in Canada and Australia, and 0% in Denmark. Although data are not available, one estimate provided in 2016 was that ∼30–40% of carotid interventions in China were for asymptomatic stenosis (Liping Liu, Beijing and Yin Quin, Nanjing, personal communication, 2016). Such disparities call into question the advisability and even the ethics of routine intervention. Reasons for this practice do not bear scrutiny.40 Although two recent studies41 ,42 indicated that after the perioperative risks are deducted, both CAS and CEA are associated with annual stroke risks of only ∼0.5%, this does not justify intervention in asymptomatic stenosis. With modern medical therapy, the annual risk of ipsilateral stroke in asymptomatic stenosis is also only ∼0.5%,37 ,43 ,44 but the periprocedural risk does not exist. In the ACT 1 trial, the 30-day risk of stroke or death was 2.9% with CAS and 1.7% with CEA. In the CREST trial, the 30-day risk of stroke or death among asymptomatic patients was 2.5% for stenting and 1.4% for endarterectomy. Thus, medical therapy is much safer with modern intensive medical therapy than with either CAS or CEA. An editorial accompanying the two recent papers20 called for a moratorium on intervention for asymptomatic stenosis outside trials being conducted with a contemporaneous medical treatment arm.
The risk of myocardial infarction is higher with CEA than with CAS, but most studies show that the risk of stroke, the clinically more important and relevant issue in a procedure being carried out for the purpose of preventing stroke, is approximately twice as high with CAS than with CEA. Reasons for this are shown in figure 3, which shows microemboli on TCD during stent deployment.45 Several studies of diffusion-weighted MRI show that small silent infarctions are more common after CAS than after CEA.20 In principle, shoving a catheter into a stiff, tortuous craggy artery is not a good idea. This is probably why stenting is worse in older patients.

Microemboli during deployment of a carotid stent. Microemboli during carotid stenting. Showers of emboli commonly (even usually) occur during carotid stenting. Panel A shows microemboli in both middle cerebral arteries while crossing the aortic arch during stenting of a common carotid; panel B shows microemboli in the middle cerebral artery during stenting of the ipsilateral internal carotid artery (courtesy of Dr Claudio Muñoz. Reproduced by permission of Springer to reproduce from: Spence et al).45
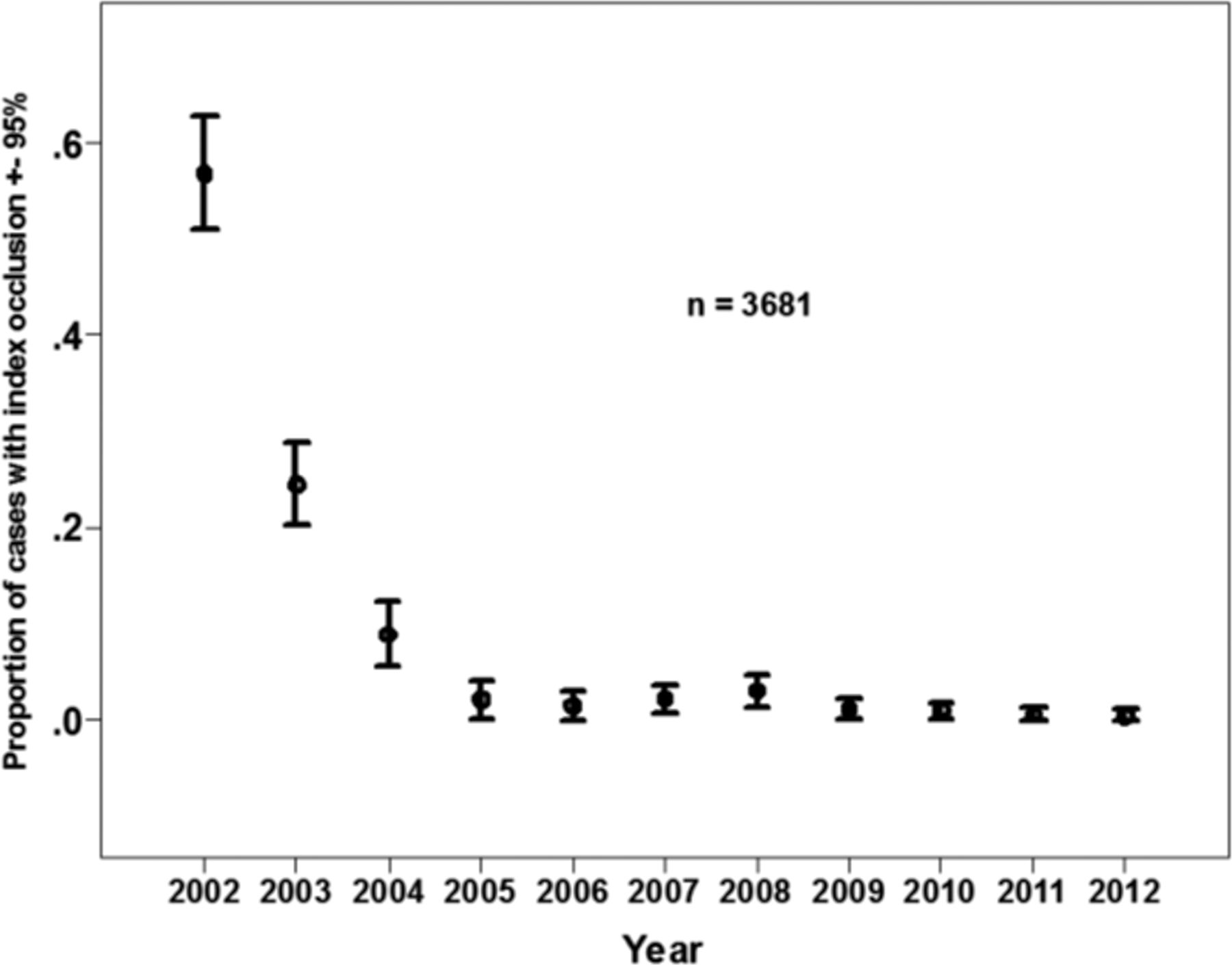
Too often, carotid stenting is performed for the purpose of preventing carotid occlusion. This may be more prevalent among cardiologists, who perform a disproportionate share of stenting in the USA (30% of interventionalists are cardiologists, but they perform half the procedures). This may be due to a mistaken perception that a carotid occlusion would be analogous to occlusion of a left main coronary artery—often called a ‘ticking time bomb’. However, since the circle of Willis is so effective in maintaining perfusion beyond a carotid stenosis or occlusion, the risk of stroke at the time of carotid occlusion is actually very low: 0.3%,46 well below the risk of either endarterectomy or stenting. Prevention of occlusion is not a valid reason for carotid intervention in ACS. Figure 4 shows the decline in the rate of carotid occlusion over time, with more intensive medical therapy. Most patients with ACS (∼90%) would be better served by intensive medical therapy than by either CEA or CAS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Decline in the risk of carotid occlusion with more intensive medical therapy. Among 3681 patients in the database, the percentage of patients who progressed to occlusion was much higher before 2002; the frequency decreased markedly after implementation in 2002–2003 of more intensive therapy based on plaque measurements. Error bars indicate 95% CI (reproduced by permission of the American Medical Association from: Yang et al).46
Identifying patients who could benefit from intervention
Although most patients with asymptomatic stenosis would be better treated with intensive medical therapy, ∼10% would be better treated with CAS or CEA. Such patients can be identified by several methods. The best validated is TCD embolus detection. In 2005, Spence and colleagues reported that patients with ACS with two or more microemboli in 1 h of TCD monitoring had a 15% 1-year risk of stroke, much higher than the risk of CEA or CAS. The 10% without microemboli had only a 1% 1-year risk of stroke, well below the risk of intervention. This result was replicated in 2010 among 468 patients with asymptomatic stenosis by Spence and colleagues, and validated in 467 patients by Markus et al.47 Other approaches in development to detecting high-risk ACS include cerebrovascular reserve,48 ,49 intraplaque haemorrhage on MRI,50 ulceration on 3D ultrasound51 and plaque inflammation on PET/CT.52 In contrast to symptomatic stenosis, degree of stenosis is not a reliable way to identify high-risk patients with ACS.44 ,53 Identifying high-risk plaques would be helpful both in symptomatic mild carotid stenosis and in asymptomatic stenosis.
How should patients with ACS be managed in 2016?
Most patients with ACS should receive intensive medical therapy; only those who can be identified as having a high risk of stroke, as described above, should have intervention. Intensive medical therapy for ACS54 includes smoking cessation, a Mediterranean diet, antiplatelet agents, lipid-lowering drugs, blood pressure control, and intensive lipid lowering using an approach called ‘treating arteries instead of treating risk factors’ and B vitamins to lower homocysteine.
Conclusion
Most patients with ACS would be better treated with intensive medical therapy than with either stenting or endarterectomy. The few (∼10%) who could benefit from intervention can be identified by TCD embolus detection, or by other methods in development.
References
Footnotes
Contributors JDS wrote the first draft, and HS and GC contributed to revisions; JDS wrote the final draft.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No additional data are available.